
Abstract
The capacity of the blood enzyme glutamate oxaloacetate transaminase (GOT) to remove glutamate from the brain by means of blood glutamate degradation has been shown in experimental models to be an efficient and novel neuroprotective tool against ischemic stroke; however, the beneficial effects of this enzyme should be tested in patients with stroke to validate these results. This study aims to investigate the association of GOT levels in blood with clinical outcome in patients with acute ischemic stroke. In two clinical independent studies, we found that patients with poor outcome show higher glutamate and lower GOT levels in blood at the time of admission. Lower GOT levels and higher glutamate levels were independently associated with poorer functional outcome at 3 months and higher infarct volume. These findings show a clear association between high blood glutamate levels and worse outcome and
Introduction
Ischemic stroke is a devastating disease that is a leading cause of death and disability in developed countries. However, therapeutic interventions are notably limited, and the administration of thrombolytic therapy with recombinant tissue plasminogen activator remains as the only pharmacologic treatment that has been shown to be effective in acute ischemic stroke (Hacke et al, 2008; Wahlgren et al, 2008). Therefore, it is mandatory to develop new and effective therapies that can improve outcome after ischemic stroke.
It is a well-established fact that during brain ischemia, glutamate acts as an important mediator of neuronal degeneration; in fact, studies conducted by our group have shown that neurologic deterioration of patients with ischemic stroke is associated with higher glutamate levels in blood and cerebrospinal fluid (Castillo et al, 1996, 1997).
Previous studies have described that glutamate can diffuse through brain capillary endothelial cells from the brain to the blood torrent in a unidirectional manner following a gradient of concentration (Hawkins, 2009; O'Kane et al, 1999; Teichberg et al, 2009). As ischemic stroke is associated with an excessive release of glutamate into the brain parenchyma (Castillo et al, 1996, 1997), a decrease in blood glutamate levels provides a mechanism to increase the gradient concentration and to remove this neurotransmitter from the brain at early times, with possible therapeutic implications after an ischemic insult (Gottlieb et al, 2003; Teichberg et al, 2009).
According to this, the capacity of the enzyme glutamate oxaloacetate transaminase (GOT) to metabolize glutamate represents a strategy to decrease glutamate levels in blood (Gottlieb et al, 2003; Teichberg et al, 2009). In fact, we observed that oxaloacetate-mediated GOT activation in an animal model of ischemia induces a neuroprotective effect, thus showing this endogenous blood enzyme as a novel neuroprotective tool against ischemic stroke (Campos et al, 2011).
However, evidences about the benefits of this enzyme in stroke patients have not yet been tested. In this clinical study, we aim to show that high blood levels of GOT in ischemic stroke patients are associated with lower glutamate levels in blood and subsequently with good outcome.
Materials and methods
Studied Population and Patients Characteristics
Two independent cohorts of ischemic stroke patients were studied. In the development cohort, between February 2009 and August 2009, 155 patients with a delay from symptom onset < 12 hours duration and previously independent for their daily living activities were prospectively evaluated to be included in the study. Patients had been admitted to the University Hospital of Santiago de Compostela, Spain. Patients with stroke on awakening (
A validation cohort of patients treated at another institution (Hospital Universitari Dr Josep Trueta of Girona, Spain) was selected to meet the same inclusion and exclusion criteria as the development cohort. Between June 2008 and September 2009, a second independent group of patients (
All patients were prospectively evaluated using cerebral computed tomography (CT), neurologic, and functional scales during a follow-up period of 90 days. Sample size was calculated using EPIDAT software (EPIDAT 3.1. (2006), Conselleria de Sanidade, Xunta de Galicia, Spain) assuming α- and β-errors of 0.05 and 0.2, respectively. Protocol was approved by the ethics committee of the participating hospitals. Informed consent was obtained from each patient or from their relatives after full explanation of the procedures.
Clinical Variables
All patients were admitted in the Acute Stroke Unit and treated by the same unit staff according to the Guidelines of the Cerebrovascular Diseases Study Group of the Spanish Society of Neurology (Comité
Neuroimaging Studies
Computed tomography scans were carried out at admission between days 4 and 7 of hospitalization. Early CT signs of infarction were evaluated at admission, and infarct volume was assessed at the second CT scan. Infarct volume (mL) was calculated on the radiographic plate using the formula 0.5 ×
All CT scans were evaluated by neuroradiologists blinded to clinical and biochemical data.
Outcome Variables
The primary end point was defined as good functional outcome (modified Rankin Scale ≤2) at 3 months. The correlation between GOT levels and infarct volumes was considered as the secondary outcome variable.
Laboratory Tests
Blood samples, obtained from all patients at admission, were collected in chemistry test tubes, centrifuged at 3,000
Statistical Analysis
Results are expressed as percentages for categorical variables and as mean (s.d.) or median (quartiles) for continuous variables, depending on the normal or nonnormal distribution of data. Proportions were compared using the χ2 test, and Student's
The influence of GOT and glutamate levels on functional outcome was assessed by logistic regression analysis, after adjusting for the main baseline variables related to outcome in the univariate analyses. Given the sample size, variables with
Results were expressed as adjusted odds ratios (ORs) with the corresponding 95% confidence intervals (95% CIs). The influence of GOT and glutamate levels on infarct volumes was evaluated by general linear models after adjusting for variables associated in bivariate comparisons. Statistical analyses were performed using SPSS 16.0 (SPSS, IBM Corporation, Somers, NY, USA).
Results
Descriptive Analysis
In the group of 111 acute ischemic stroke patients, 60.4% were men and the average age was 70.9 ± 11.2 years. The median (quartiles) NIHSS score on admission was 11 (5, 16), and the average time from symptom onset was 3.9 ± 2.3 hours, the average of diffusion weighted imaging volume on admission was 39.7 ± 56.2 mL, and the number of tissue plasminogen activator-treated patients was 32 (28.8%). Stroke subtype was classified as atherothrombotic (10.8%), cardioembolic (37.8%), undetermined (37.8%), and lacunar (13.6%). Glutamate oxaloacetate transaminase levels correlated negatively with serum levels of glutamate at admission (
In the validation group of 254 patients with acute ischemic stroke, 56.3% were men and the average age was 70.3 ± 11.6 years. The average NIHSS score on admission was 13 (7, 19), the average time from symptom onset was 2.6 ± 1.9 hours, the average of diffusion weighted imaging volume on admission was 31.6 ± 48.5 mL, and the number of tissue plasminogen activator-treated patients was 101 (39.8%). Stroke subtype was classified as atherothrombotic (14.2%), cardioembolic (54.1%), undetermined (26.5%), and lacunar (5.2%). Glutamate oxaloacetate transaminase levels correlated negatively with serum levels of glutamate at admission (
Effect of Glutamate Oxaloacetate Transaminase and Glutamate Levels on Functional Outcome in Ischemic Stroke Patients
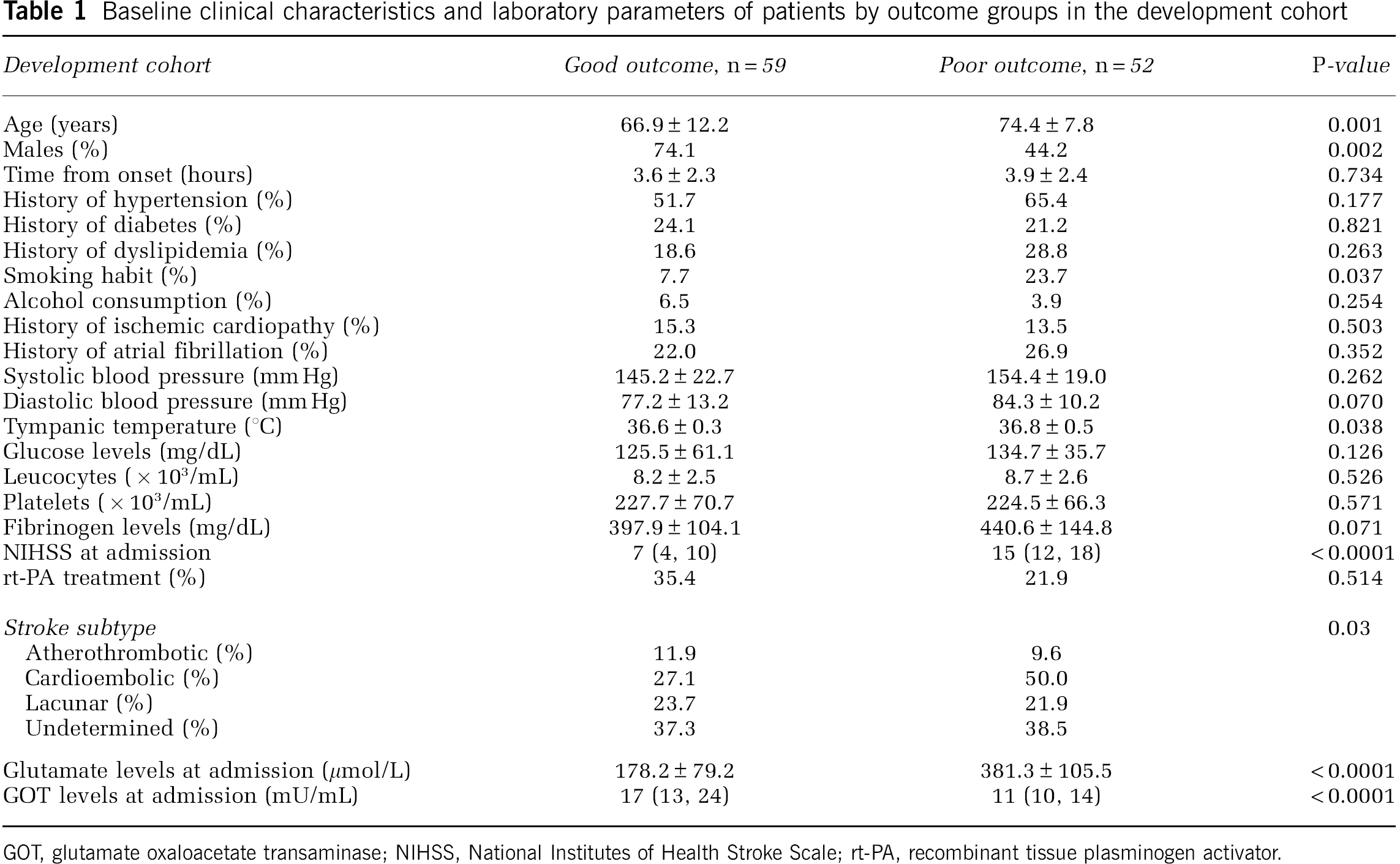
Table 1 shows the main characteristics of patients from the development cohort by outcome groups. A total of 52 patients (46.8%) showed poor functional outcome at 3 months. Females, smoking habit, and cardioembolic stroke subtype were significantly more frequent, and temperature was significantly higher at admission for patients with poor outcome. Besides, patients with poor outcome were older and showed higher stroke severity. With regard to molecular markers, patients with poor outcome showed higher glutamate levels at admission, and presented lower GOT levels at admission.
Baseline clinical characteristics and laboratory parameters of patients by outcome groups in the development cohort
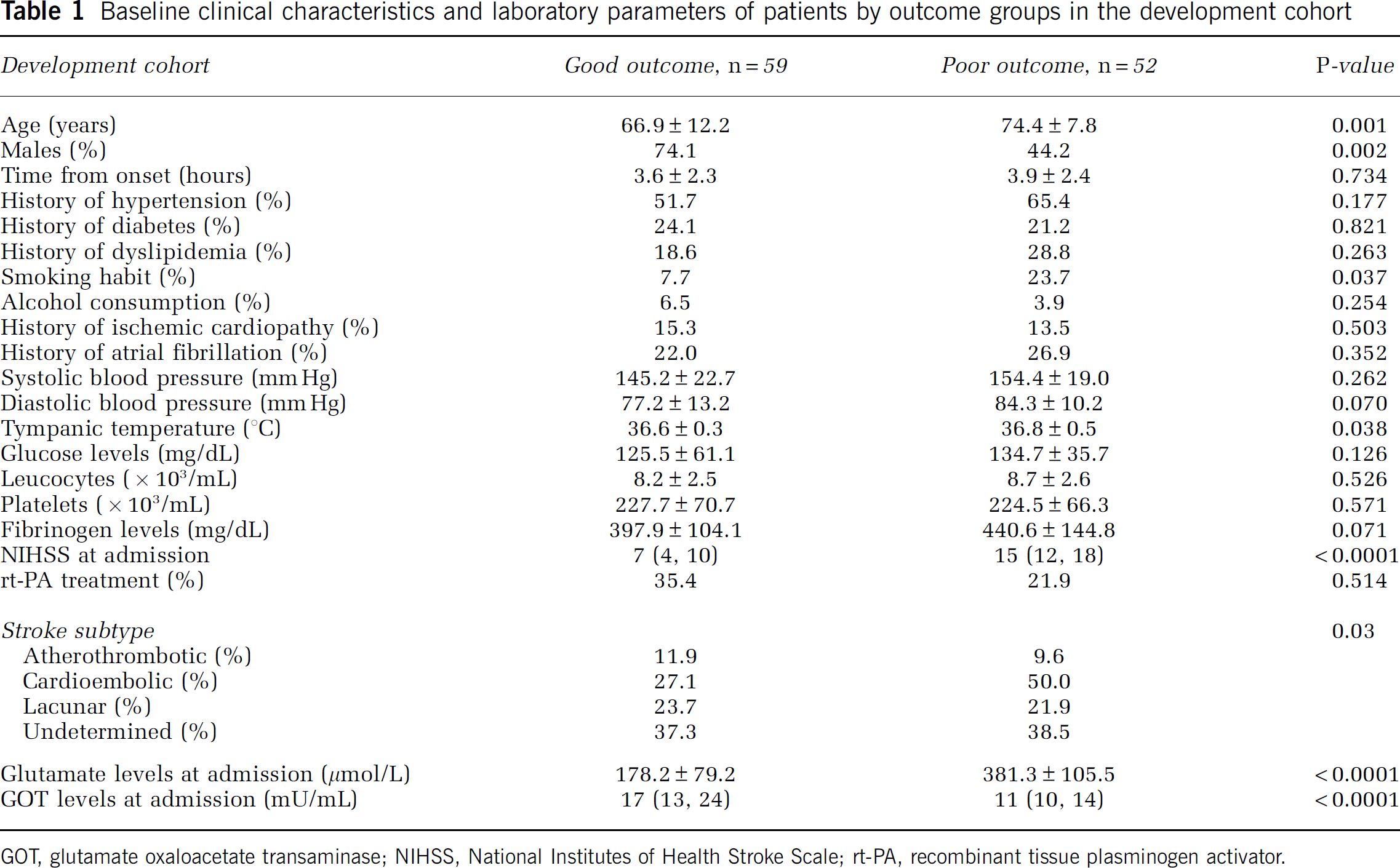
GOT, glutamate oxaloacetate transaminase; NIHSS, National Institutes of Health Stroke Scale; rt-PA, recombinant tissue plasminogen activator.
In the validation cohort (see Supplementary Table 1), patients with poor outcome were older and showed higher glucose levels and stroke severity at admission. With regard to molecular markers, patients with poor outcome showed higher glutamate levels at admission and presented lower GOT levels at admission.
In both cohort of patients, the higher glutamate levels at admission corresponded to the higher modified Rankin Scale score at 3 months (Figures 1A and 1B).
Glutamate serum levels at admission versus mRS score. The higher glutamate levels at admission corresponded to higher mRS scores at 3 months. Panel
In the development cohort (Table 2, Model A), GOT levels at admission were independently associated with poor outcome (OR, 0.81; 95% CI, 0.71 to 0.93,
Adjusted OR of poor functional outcome for GOT levels (Model A) and for glutamate levels at admission (Model B) in the development cohort
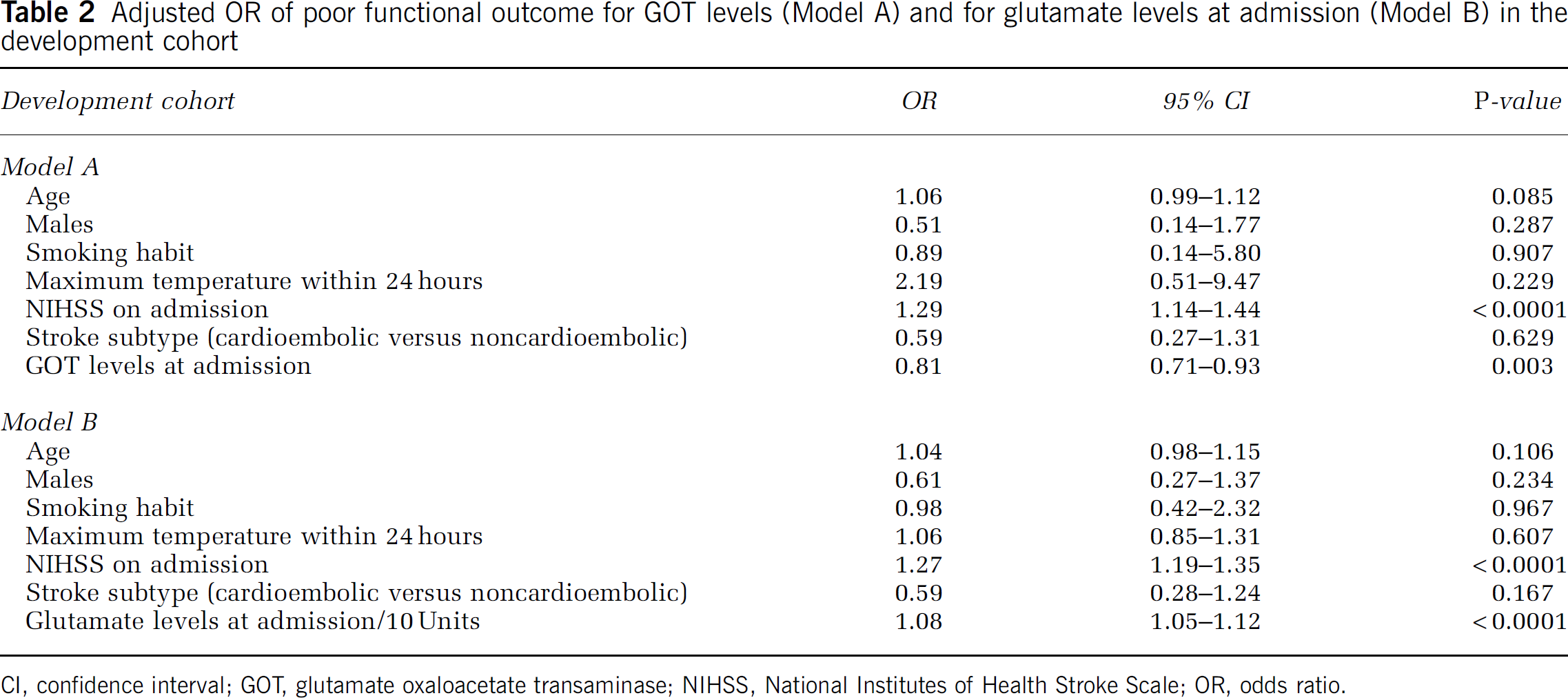
CI, confidence interval; GOT, glutamate oxaloacetate transaminase; NIHSS, National Institutes of Health Stroke Scale; OR, odds ratio.
In the validation cohort (see Supplementary Table 2, Model A), GOT levels at admission were independently associated with poor outcome (OR, 0.88; 95% CI, 0.84 to 0.92,
Effect of Glutamate Oxaloacetate Transaminase and Glutamate Levels on Infarct Volume in Ischemic Stroke Patients
In the development cohort, infarct volume was associated with male gender (
Baseline clinical characteristics and laboratory parameters for infarct volume in the development cohort
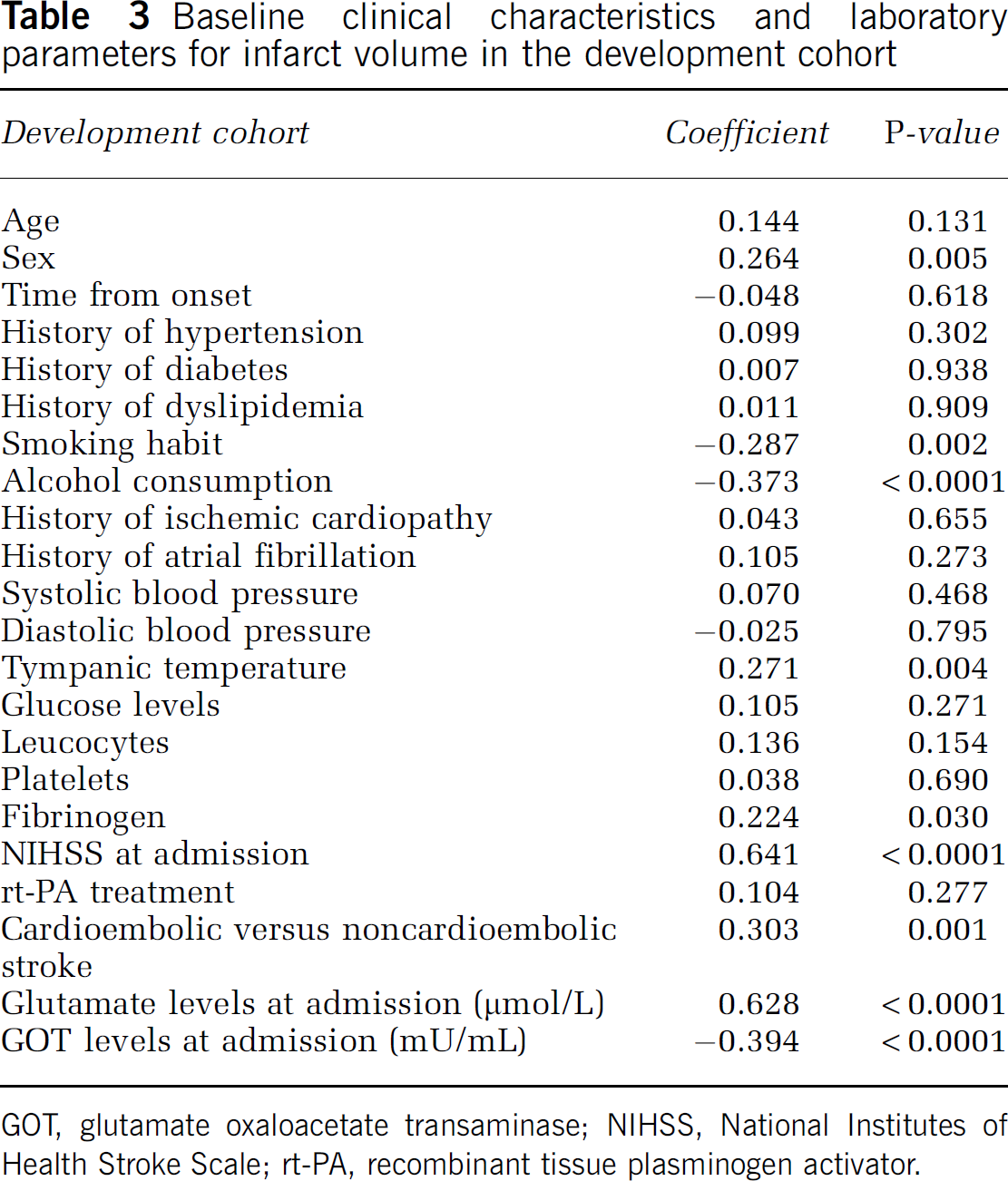
GOT, glutamate oxaloacetate transaminase; NIHSS, National Institutes of Health Stroke Scale; rt-PA, recombinant tissue plasminogen activator.
In the validation cohort, history of hypertension (
In the multivariate analysis (Table 4, Model A), GOT levels at admission were independently associated with infarct volume (
Adjusted
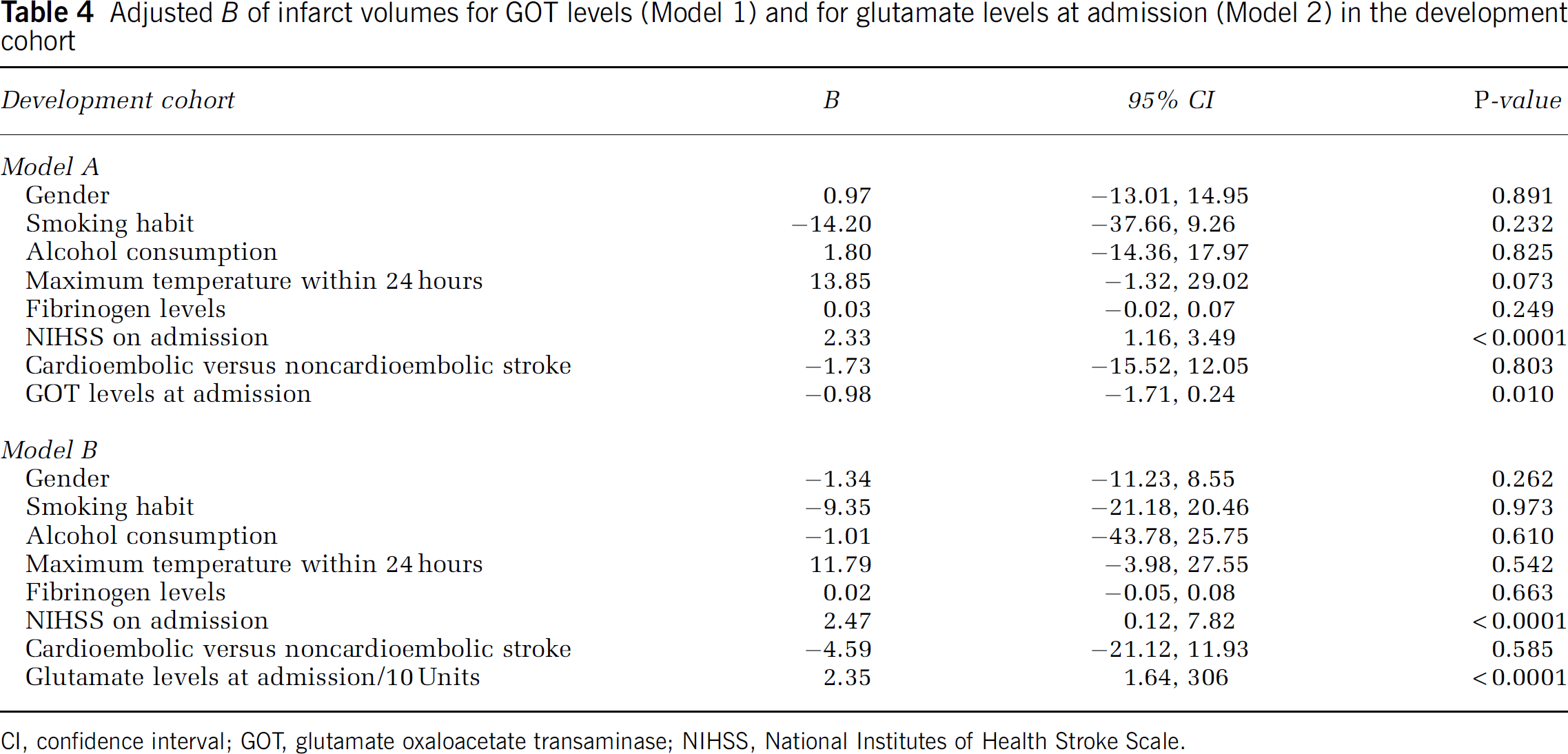
CI, confidence interval; GOT, glutamate oxaloacetate transaminase; NIHSS, National Institutes of Health Stroke Scale.
In the validation cohort (see Supplementary Table 4, Model A), GOT levels at admission were independently associated with infarct volume (
When multiple linear regression is calculated with glutamate levels at admission instead of GOT, glutamate seems independently associated with infarct volume (
Discussion
During ischemic stroke, glutamate is highly released into the extracellular space leading to a marked increase in intracellular calcium, followed by the activation of intracellular enzymes, which provokes neuronal death. As glutamate has a central role in the ischemic cascade, this neurotransmitter represents a good target in the search for neuroprotective agents in ischemic stroke. In this sense, calcium and glutamate antagonists have been attractive tools used as neuroprotective agents in experimental studies of cerebral ischemia, but they failed when tested in clinical trials and many of them also showed adverse effects (Ginsberg, 2008). Nevertheless, the relevant role of glutamate in the ischemic cascade of stroke makes it necessary to look for new neuroprotective strategies based in glutamate.
In experimental models, the capacity of the enzyme GOT to remove glutamate from the brain by means of blood glutamate degradation has been shown to be an efficient and novel neuroprotective strategy against ischemic damage; however, the beneficial effects of this enzyme have not yet been tested in stroke patients (Gottlieb et al, 2003; Teichberg et al, 2009; Zlotnik et al, 2007).
Glutamate oxaloacetate transaminase is an enzyme that is normally expressed in the liver and heart cells and released into blood under different kinds of pathologies (Ladue et al, 1954; Lin et al, 2010). Owing to the effect of GOT on glutamate metabolism, we hypothesize that high blood levels of GOT could correlate with a better functional outcome and lower infarct volume in ischemic stroke patients.
To prove the association between blood GOT levels and clinical outcome in ischemic stroke patients, we carried out two clinical independent and observational studies, the primary end point of which was functional outcome at 3 months. We found that patients with poor outcome showed higher glutamate levels and lower GOT levels in blood at admission. Higher GOT levels at admission were independently associated with good functional outcome at 3 months. This favorable effect on the primary variable was also supported by positive effects on the reduction of lesion volume.
The confirmation of these clinical results in another independent cohort of ischemic stroke patients shows a clear association between high blood glutamate levels and worse outcome and
According to this, in a previous experimental study with animal model of cerebral ischemia by means of a middle cerebral arterial occlusion and following the Stroke Therapy Academic Industry Roundtable (STAIR) group guidelines (Campos et al, 2011), we observed that oxaloacetate-mediated GOT activation inhibits the increase in blood and cerebral glutamate after middle cerebral arterial occlusion, inducing a reduction of infarct size, smaller edema volume, and lower sensorimotor deficits with regard to controls, thus showing the neuroprotective effect of the enzyme GOT.
Attending to these experimental results and these clinical findings, it is tempting to postulate that the administration of GOT might be an effective therapy in ischemic stroke because of its capacity to decrease blood and brain glutamate. In fact, previous studies by our group have shown that neurologic deterioration and infarct growth in acute ischemic stroke is associated with higher glutamate levels in blood (Castellanos et al, 2006; Castillo et al, 1996, 1997).
However, as the inclusion of patients was not randomized, our study has some limitations, such as the different percentages of cardioembolic patients observed in both cohorts, 37.8% versus 54.1%. Nevertheless, this limitation has not affected the aim of this study.
In conclusion, these clinical findings show a clear association between low blood glutamate levels and high blood GOT levels with good outcome, probably mediated by the capacity of this enzyme to metabolize blood glutamate. In this regard, further clinical trials based on the administration of GOT or agents that can increase GOT expression or activity are necessary to show the neuroprotective effects of GOT in stroke patients.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.