
Abstract
Combination therapy has been identified as a promising strategy to improve stroke management. We conducted a systematic review and meta-analysis of evidence from animal models of ischemic stroke to determine whether combining treatments improved efficacy. Multiple databases were searched and data were extracted from focal ischemia experiments comparing control groups, single treatments, and combination treatments. Of 11,430 papers identified, 142 met the inclusion criteria; these tested 126 treatments in 373 experiments using 8,037 animals (
Introduction
With no single ‘magic bullet’ for stroke, combination therapy is an increasingly appealing strategy (Cheng et al, 2004; Danton and Dietrich, 2004; Adams et al, 2003; Rogalewski et al, 2006; Fisher, 2003; Fisher et al, 2005, 2007). Combination therapies might raise the efficacy above levels achievable with single therapies; or extend the time window for thrombolysis with tissue plasminogen activator (tPA). Indeed, the multifaceted manifestations of stroke and its complications mean that most patients already receive a number of different interventions, notwithstanding that they may be administered for purposes ranging from management of hypertension, blood sugar levels, infection, and fluid balance through to those interventions aimed at improving mobility and speech. Testing combination therapies with the intention of reducing brain injury requires increased trial complexity and may present significant intellectual property and regulatory issues (European Ad Hoc Consensus Group, 1998; Saver and Kalafut, 2001). Combination therapies also raise the specter of a Pyrrhic victory where the adverse effects of multiple treatments outweigh real but small benefits; where patients take more than four medications, the risk of adverse events increases substantially (Byrne, 2003).
Combination therapy has been used in the treatment of blood pressure (Brown et al, 2003), cancer (Corn, 2004), and coronary artery disease (Ramanath and Eagle, 2007). Currently, there is little evidence to support the routine use of specific combinations to reduce brain injury in acute stroke (Adams et al, 2007), but this is an active area of research—driven by scientific and commercial imperatives—and is the subject of many patent applications (Brimble and Levi, 2006; Novartis, 2007; Moleac, 2007; Neurokey A/S, 2007).
Meta-analysis allows the aggregation of data from a number of experiments to give a summary estimate of efficacy. We aimed to use meta-analysis of data from experiments testing combination therapies in animal models of ischemic stroke—identified using systematic review—to establish first, whether the use of therapies in combination resulted in greater efficacy than might be expected from their use as monotherapy; and second, whether the use of therapies in combination with thrombolysis extended the delays to treatment at which efficacy was seen.
To protect from the risks of
The specific aims of the study were to examine (1)
Materials and methods
Scope
We included nonhuman animal studies in focal cerebral ischemia experiments that reported infarct size in a control group (no treatment), a single treatment group, and a combination group receiving the single treatment plus an additional treatment. Experiments without both single and dual groups were excluded since both were necessary to establish the additional effect of the second treatment. Experiments investigating treatment mechanisms using a second agent intended to counteract the effect of the first were also excluded. Where studies measured behavior, inclusion of data was restricted to neurological scores (results aggregating data from two or more behavioral test items into a single score).
Search Strategy
The following databases were searched: Web of Science, Current Contents, Biosis Previews, Pubmed, CAB abstracts, and Society for Neuroscience (search 21 September 2010). Search criteria were (1) combination neuroprotection; (2) neuroprotection AND (thrombolysis OR hypothermia); (3) (drug interaction OR combination therapy OR synergistic effect OR drug combination OR multiple drugs OR additive effect OR combinatorial treatment OR combinatorial therapy OR multimodal therapy) AND (stroke OR focal ischemia OR focal ischaemia OR cerebral ischaemia OR cerebral ischemia OR neuroprotection). Where possible, searches were restricted to animals.
Study Selection and Data Extraction
Studies were included if delivery and dose regimes for the single treatment were replicated in the combination condition. Information extracted included infarct size and neurological score summary statistics (mean, standard deviation/error, sample size); Intervention (treatment time, delivery method, mechanism of action); Study characteristics (species, animal age, and stroke model) and study quality. Animals of 6 months or older were defined as ‘old.’ Study quality was rated as a composite of 10 criteria (Supplementary Table 1) (Macleod et al, 2004). Where volumetric data were not available, estimates were based on areas. Where data were presented only graphically, values were estimated using an electronic ruler.
Results of meta-analysis of efficacy of therapies tested alone and in combination with a second therapy in animal models of ischemic stroke
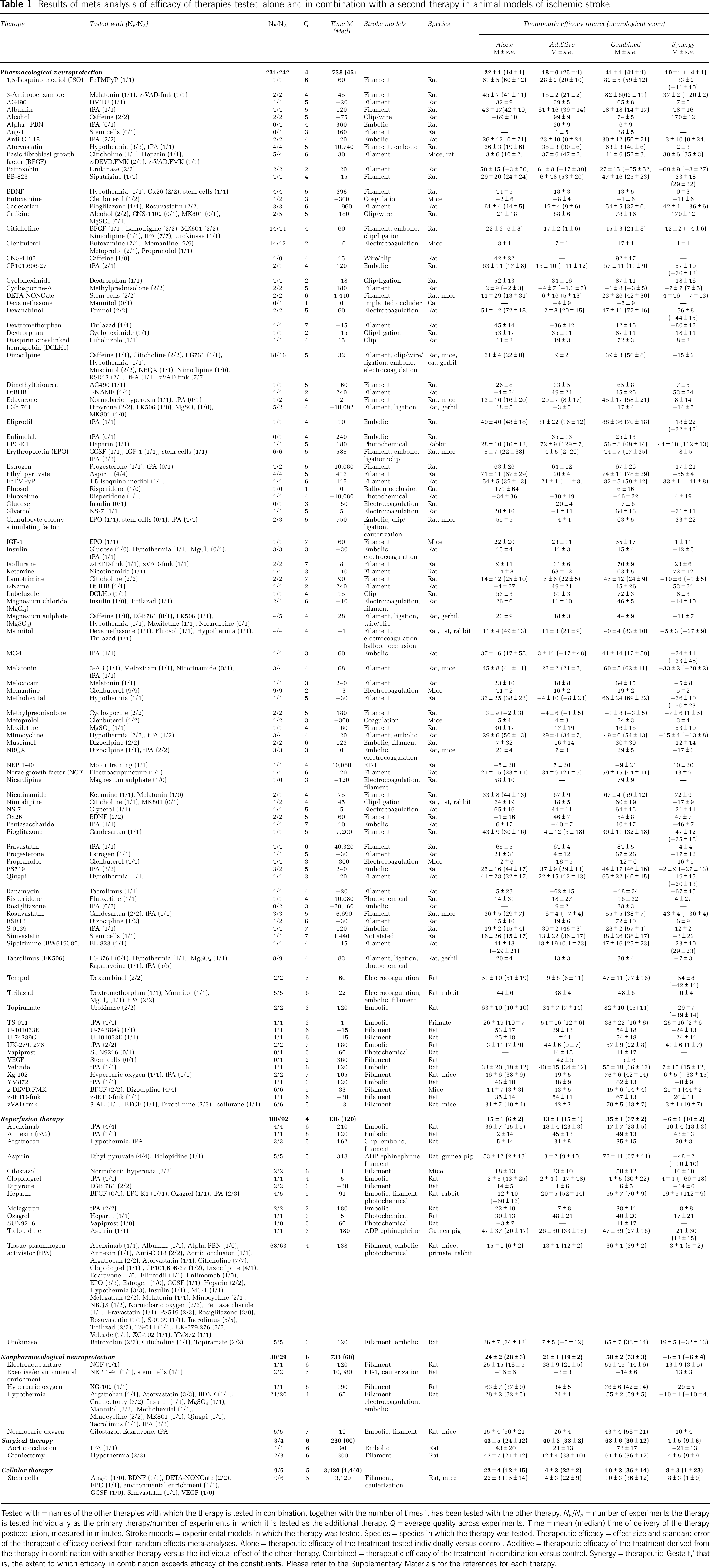
Tested with = names of the other therapies with which the therapy is tested in combination, together with the number of times it has been tested with the other therapy.
Sensitivity Analysis and Meta-Analysis of Therapeutic Effect
Behavioral data were transformed to the same direction of effect and normalized to the size of the scale. Within each experiment, means and standard deviations (s.d.) in the single and combination groups were expressed as a percentage of control group outcomes (Macleod et al, 2004). Sample sizes in the control groups were adjusted for multiple comparisons (Macleod et al, 2004). We did not use a standardized mean difference approach because where sample size is small the observed s.d. is an imprecise measure of the population s.d., thereby introducing measurement error and reducing the power of the analysis. Mean outcomes were extracted to obtain: (1) single treatment effect (single treatment versus control); (2) combination treatment effect (combined treatment versus control); (3) additive effect (difference between the combination and single treatment effect for the other therapy); and (4) synergistic effect (the extent to which the combination efficacy exceeds the sum of the individual therapeutic efficacies of the constituents when tested individually). For instance, if treatment A and B tested individually reduced infarct size by 10% and 40%, respectively, and by 45% when used in combination, then the single treatment effect for A is 10%, the additive effect for A is 5% (45% to 40%), and the synergistic effect for A is −5% (45%–10%–40%). Because this calculation of synergy requires reporting of the single treatment effect of both treatments, it was not possible to calculate this for all included combinations.
Sensitivity analysis was undertaken by sequentially removing experiments—individually and in blocks—to determine their contribution to heterogeneity as measured by their effect on Cochran's
Both fixed effect and random effect meta-analysis were undertaken, and due to heterogeneity, results from the conservative random effects model are presented (DerSimonian and Laird, 1986; Macleod et al, 2004, 2005a, b ). Overall estimates of effect were calculated for (1) single treatment therapy; (2) combination therapy; and (3) synergistic efficacy. The effect size for the combination does not necessarily equal the sum of the single and additive effects, because combination treatment effect was calculated for each experiment and then a summary estimate derived using random effects meta-analysis, an approach that is more sophisticated than a simple averaging.
Data were tested for publication bias using Egger's test, a statistical analog of the funnel plot (Metabias, Stata v.10, Statacorp, TX, USA) (Egger et al, 1997); significant results (
Ceiling Effect
To investigate overall limits to acute stroke therapy (ceiling effects), meta-analysis results were partitioned into 10% bands on the basis of the level of efficacy of a single treatment when tested individually (designated here as the ‘primary treatment’). Where both treatments were tested individually, both could alternatively be considered as the primary treatment for the purpose of this analysis, with additional therapy building on this base. Meta-regression (STATA v.10) (Thompson and Sharp, 1999; STB-42, 1998) was used to test whether combination or synergistic efficacy were influenced by the effectiveness of the primary treatment. Note, the designation of primary and additional therapies was created for the purpose of this analysis and was not a classification described within individual papers themselves.
Tissue Plasminogen Activator Thrombolysis
To determine whether combination therapies extended the time window for efficacy, we examined tPA thrombolysis in greater detail. We carried out an unweighted meta-regression; treatment effects for thrombolysis alone and in combination were regressed against time of drug delivery (measured relative to stroke onset) with treatment as the within-subject factor and time of delivery as a covariate (SPSS v18, PASW Statistics, Chicago, IL, USA). We also conducted a stratified analysis of the relationship between tPA efficacy and the model of stroke (embolic, filament, photochemical) and the timing of the other treatment (pre, post, or simultaneously with tPA).
Efficacy by Treatment and Class
Data were partitioned to obtain therapeutic efficacy for individual treatments. For each therapy, the following information was tabulated: treatments with which it had been combined; extent of testing individually as the primary therapy (number of experimental contrasts (
Treatments were categorized by treatment class: (1) pharmacological neuroprotection (e.g. citicholine); (2) reperfusion therapy (e.g. tPA); (3) nonpharmacological neuroprotection (e.g. hypothermia); (4) surgical therapy (e.g. craniectomy); or (5) cell-based therapies (e.g. stem cells) (see Table 1 for the categorization of individual therapies). We used partitioned analyses to investigate the association between outcome and the treatment class of the primary treatment or the combination. Significance was tested using meta-regression (STATA v.10) (Thompson and Sharp, 1999) (STB-42, 1998).
Results
Characteristics of Experiments
The search identified 11,430 publications of which 142 met the inclusion criteria (Figure 1). From these publications, we extracted 373 three-way comparisons of a control group (1,811 animals), a single treatment (3,888 animals) and a combination of that single treatment with an additional therapy (2,268 animals). In total, data from 8,037 animals were included, with a median number of animals per treatment arm of 10 (Control IQR (interquartile range): 8 to 14; Single treatment IQR: 7 to 13; Combination treatment IQR: 7 to 13).
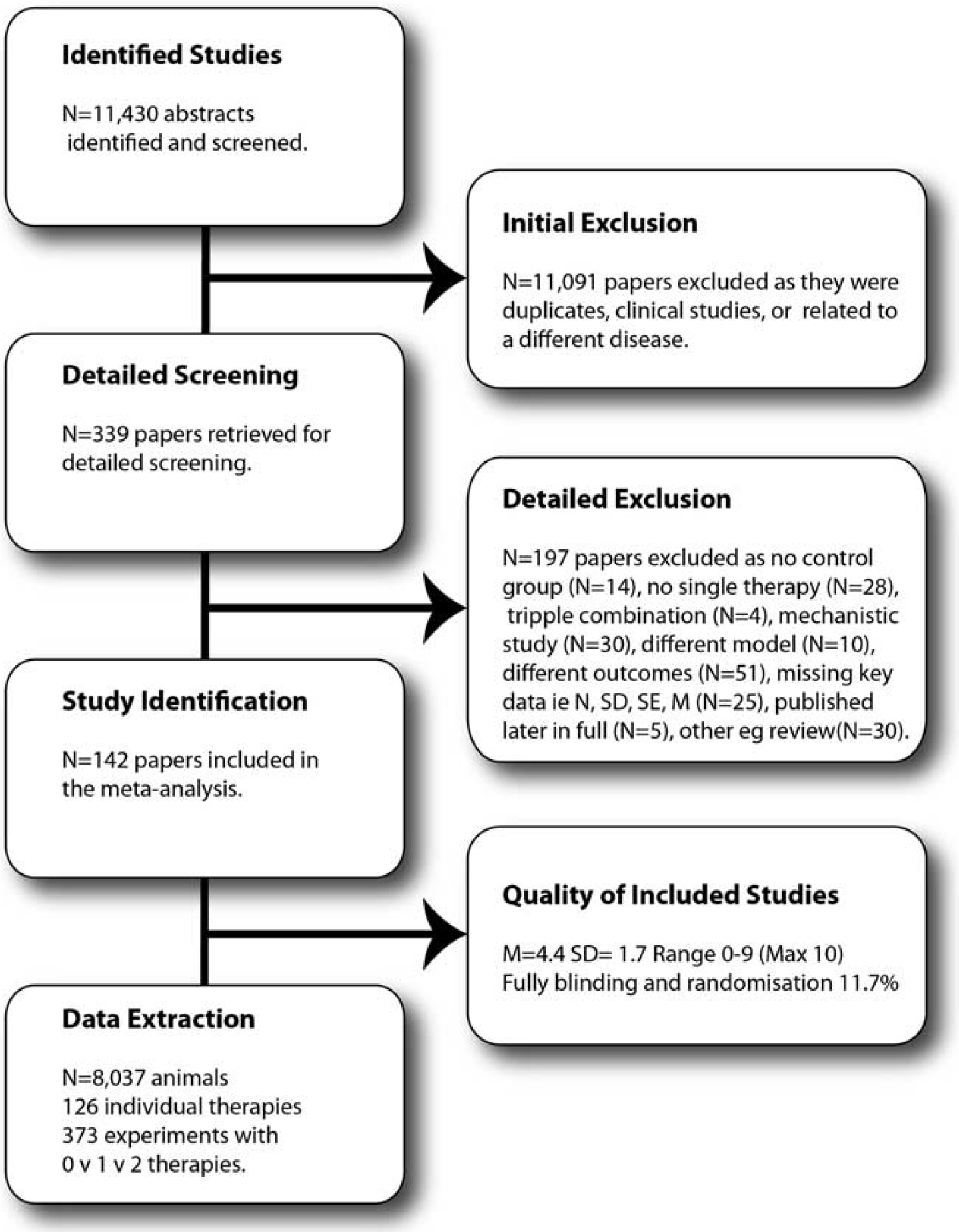
Flowchart of inclusions and exclusions in the systematic review.
Experiments were predominantly undertaken in young (98%), male animals (89% male, 2% female, or both, 9% unstated) without comorbidities (97% healthy, 3% hypertensive). The following papers used older animals (Toung et al, 2004; Zhao et al, 2005; Zhang et al, 2010; Fang et al, 2010), female animals (Toung et al, 2004; Carter et al, 1992; Liu et al, 2010), or hypertensive animals (Teichner et al, 2003; Bochelen et al, 1999; Asahi et al, 2000; Fujiwara et al, 2009; Maeda et al, 2009; Murata et al, 2008). Most experiments were conducted in rats (76% of experiments) or mice (18%), with some studies in rabbits (3%), gerbils (1.3%), guinea pigs (0.5%), cats (0.8%), or primates (0.5%). Of note, stroke was induced in gerbils using an uncommon (for gerbils) distal ischemia model rather than the standard model of global ischemia typically employed in this species. Quality ranged from 0 to 9 with a median of 4 (
Characteristics of Treatments
Overall, 126 single interventions were reported, with 118 therapies tested alone and in combination and 8 tested only in combination (Table 1). Most individual therapies were not tested extensively (median of one experiment as the first treatment, mean 2.9), with the exception of tPA (
Sensitivity Analysis
Substantial heterogeneity exists within the data, with
Meta-Analysis of Therapeutic Effect
Estimates of therapeutic efficacy are shown in Figure 2A, infarct size and 2B, neurological score), together with estimates corrected for potential publication bias. Overall, administration of a single treatment improved infarct size by 20.5% (95% confidence interval (CI): 19.6 to 21.3, 373 experiments) and neurological score by 12.3% (95% CI: 10.86 to 13.8,
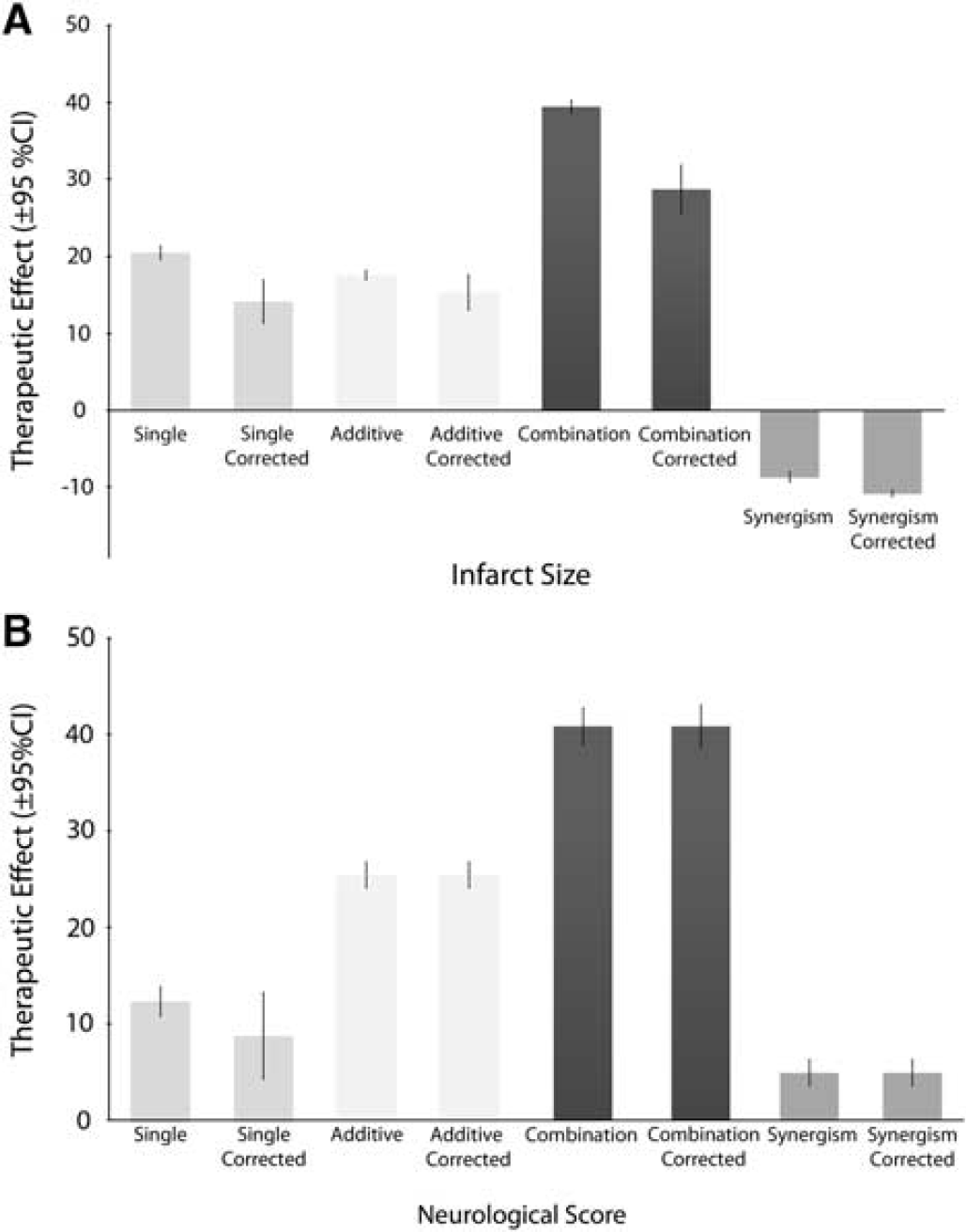
Overall estimates of treatment efficacy: raw and adjusted for potential bias. Estimates for the single treatment effect, the additive effect, and the combination treatment effect derived from DerSimonian and Laird meta-analysis and after correcting for potential publication bias using the Trim and Fill technique (
Egger's test found evidence for publication bias in the estimation of infarct effect size in single treatments (
Ceiling Effect
Combination efficacy increased as primary efficacy increased and plateaued when primary efficacy reached around 60% protection (Figure 3A, infarct size). When the primary efficacy exceeded 80%, there was little benefit from the addition of a second therapy, although CIs were wide for neurological score estimates (Figure 3B, neurological score). Synergistic effects were most pronounced when the efficacy of individual treatments was < 30%.
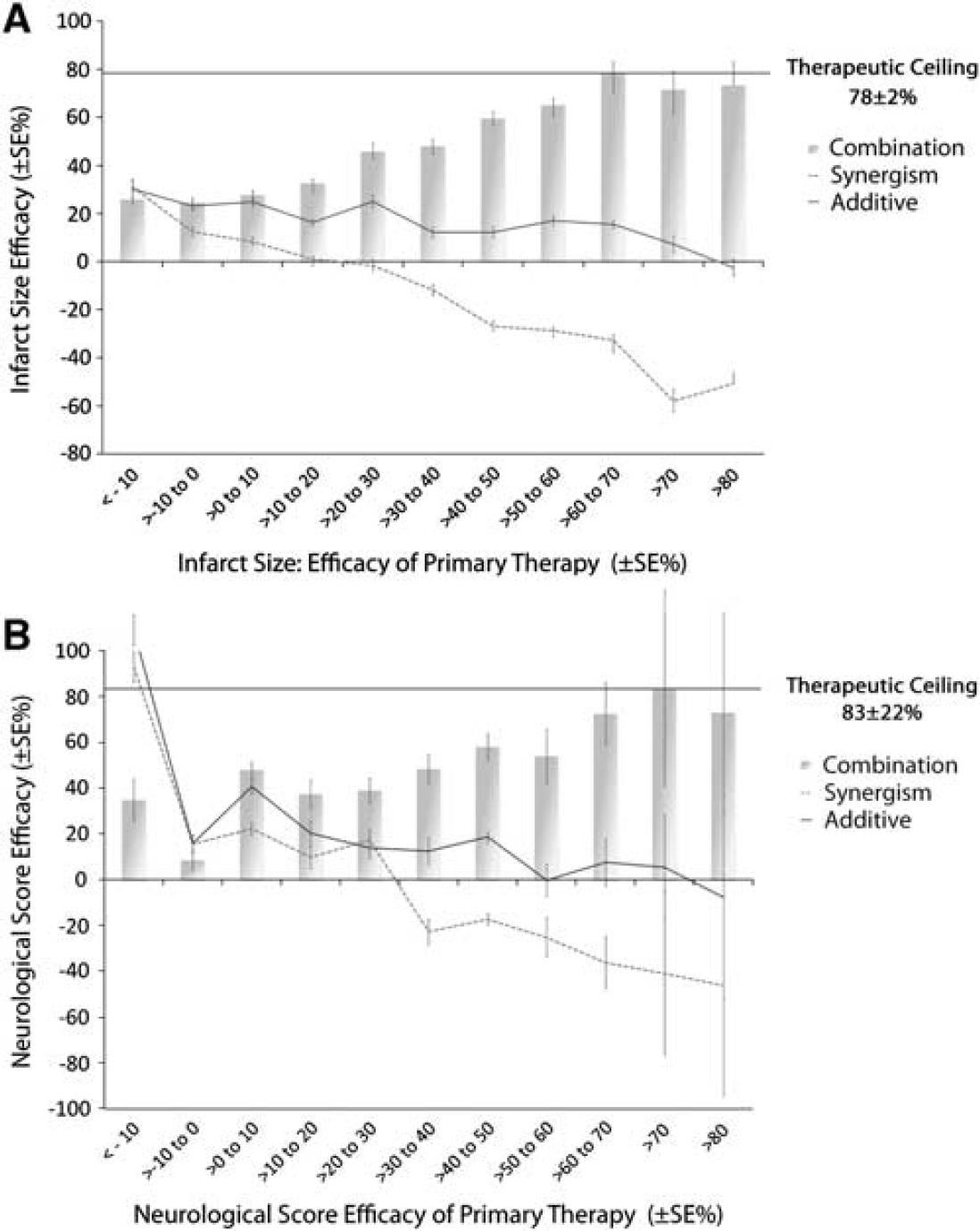
Ceiling effect to level of protection evidenced by combination therapy. (
For infarct size, there was a significant association between efficacy in primary therapy on the one hand, and efficacy in combination (β = 0.50,
Tissue Plasminogen Activator Thrombolysis in Combination
Tissue plasminogen activator was tested individually in 68 experiments and as the additional therapy in the combination in 63 experiments. When given alone, the ability of tPA to reduce infarct size was greatest in the embolic model, but when given in combination efficacy was greatest in the filament occlusion model (embolic model (
The effect of thrombolysis on infarct size was significantly related to treatment time (F(1,62) = 13.1,
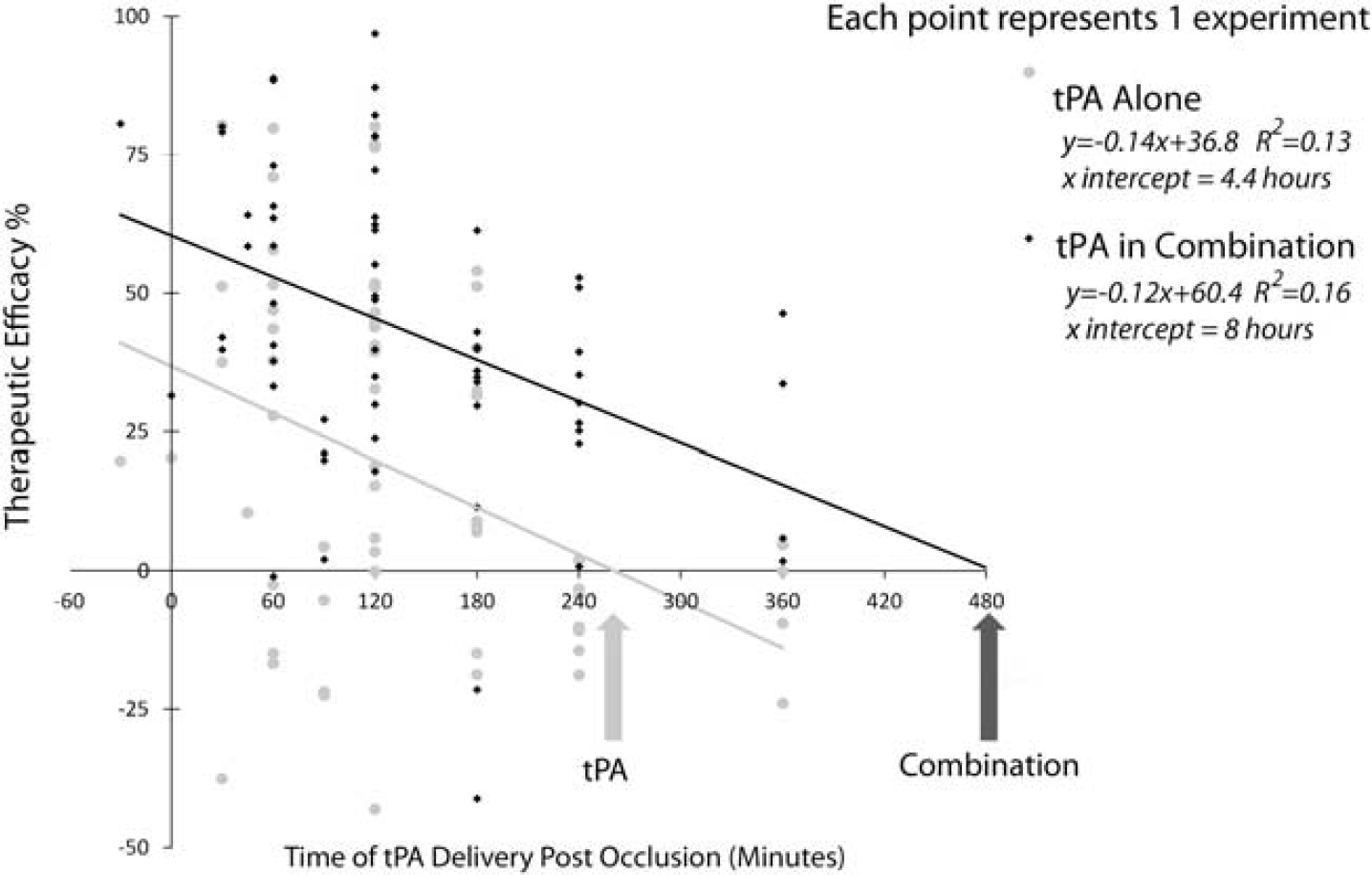
Time window for thrombolysis alone and in combination. Results from regression analysis of therapeutic efficacy of tissue plasminogen activator (tPA) thrombolysis alone and in combination with a second treatment. Therapeutic efficacy (vertical axis) is measured as the effect on infarct size with higher values indicating a better outcome in the treatment group compared with the control condition. The horizontal axis depicts the time of tPA treatment measured in minutes postocclusion (note, combination treatment time is graphed as timing of tPA in the combination, while the second treatment may have been given before or at the same time as tPA (see Figure 5 for mean differences for the second therapy). Each point represents the result from a single experiment and the lines represent the linear regression of tPA alone or in combination. With increasing delays between the time of treatment with tPA thrombolysis and the occlusion, the estimate of efficacy declines. Extrapolating from the regression curve, the predicted time of no effect for tPA is combination is extended from 4.4 to 8 hours.
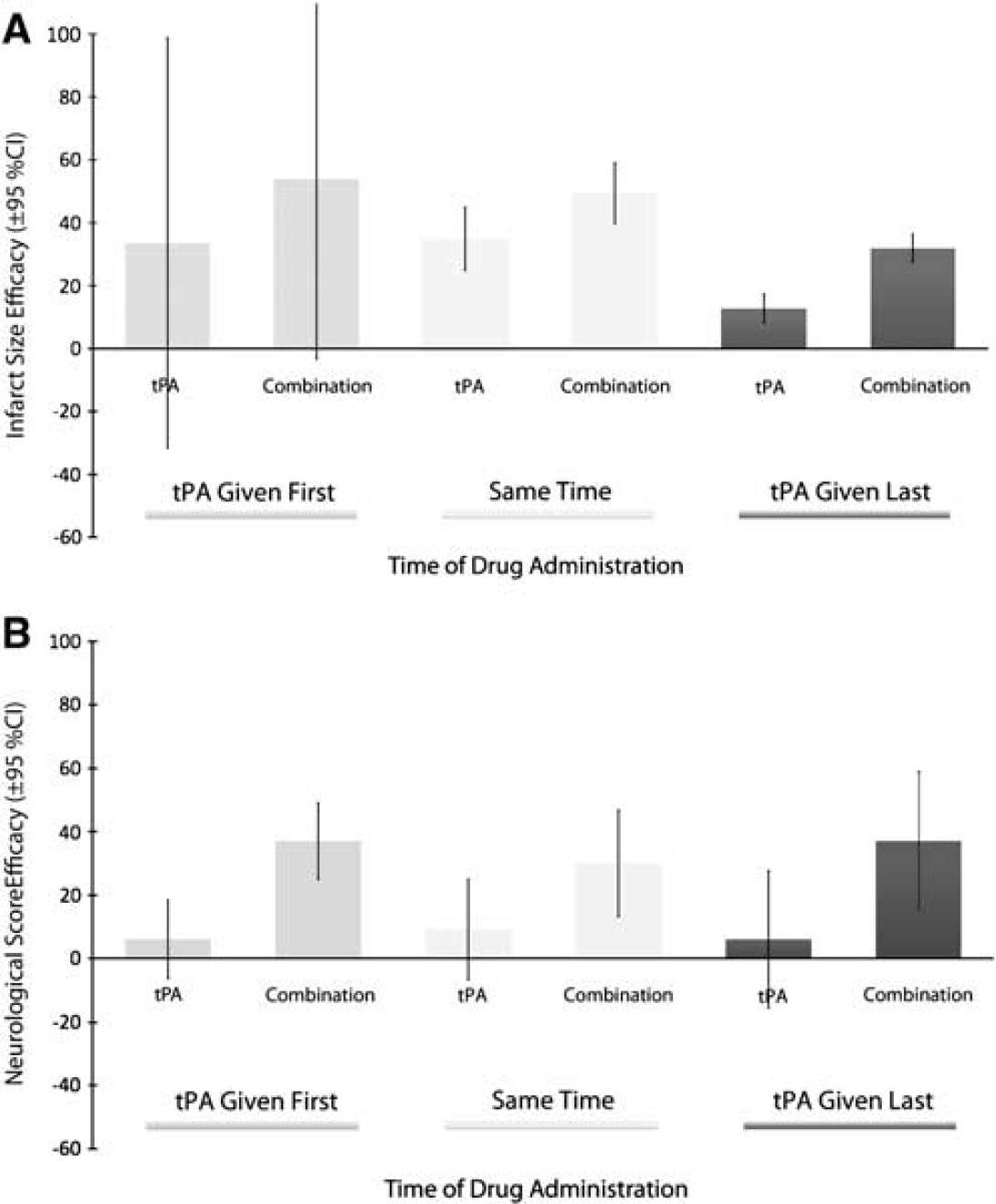
Thrombolysis in combination: relative timing of treatments. Effects sizes (with 95% confidence intervals) for tissue plasminogen activator (tPA) alone and in combination with a second treatment. Results are portioned on the basis of whether tPA was given first (
Efficacy by Class
The most common combination therapies reported were the use of two pharmacological neuroprotectants (
The most effective combinations for improving neurological score were nonpharmacological with pharmacological neuroprotection (effect size = 56.4, 95% CI: 51.2 to 61.1,
Discussion
The absence of a single magic bullet for stroke has encouraged exploration of combination therapy. We found 126 treatments that have been tested in combination in 373 experimental comparisons of control, single, and dual treatment conditions using 8,037 animals. On average, one treatment improved infarct size (or neurological score) by 20% (or 12%) compared with control, and the inclusion of a second intervention improved efficacy by an additional 18% (or 26%). The addition of a second therapy to thrombolysis may extend the time window from 4 hours 20 minutes to as much as 8 hours in animal models of stroke, although experiments testing time windows beyond 6 hours are needed to confirm this prediction.
As the efficacy of the primary therapy increases, the marginal benefits gained from the addition of a second therapy falls, and at higher levels of primary protection, negative effects may be encountered with use of a second therapy. Combination therapy appears to plateau when the efficacy of the primary therapy reaches 60%. These are of course global estimates and at higher efficacies, the small number of findings and wide CIs may mask important effects for particular combinations. For instance, in individual experiments, tPA was highly effective when combined with other treatments, notably: eliprodil (Lekieffre et al, 1997), hypothermia (Meden et al, 1994), dizocilpine (Sereghy et al, 1993), YM872 (Suzuki et al, 2003), and heparin (Carter et al, 1992). Further, the positive relationship between the efficacy of the primary and combination treatments and the inverse relationship between additive and combination efficacy will also reflect regression toward the mean. However, the importance of the efficacy of the first therapy in the overall therapeutic effect also suggests the need to build combination therapy on a solid therapeutic foundation.
The results also have implications for the design and interpretation of animal models. Surgical therapy with craniectomy—a treatment of most benefit to patients with malignant infarct rather than small strokes—was remarkably successful in reducing brain damage in animals, although the number of experiments was small. Further, animal studies typically use anesthetics. The substantial additional efficacy brought by anesthetic agents (e.g., ketamine and isoflurane) raises questions about the importance of this confounding factor—common to most animal studies but absent from clinical stroke—and also, about whether this protective mechanism may be exploited clinically to reduce brain damage.
Our analysis was observational rather than experimental and should therefore be viewed as hypothesis generating (Thompson and Higgins, 2002). However, we reduced the possibility of multiple ‘significant’ findings by prespecifying analyses (Alder et al, 2006; Thompson and Higgins, 2002). Results can be swayed by outlying studies, but we conducted sensitivity analyses with these excluded and our conclusions were not substantially different.
Owing to heterogeneity in the data, the scope of the paper was restricted in terms of end points; however, end points other than neurological score and infarct volume may be relevant to the treatment under investigation and to the external validity of animal models. In a nod to heterogeneity, random effects analyses were performed and individual treatments were listed so that readers may make a more detailed study of treatments of interest. Analysis of specific factors affecting ceiling effects might provide greater insight into the relationship between the combination therapies and potential ceiling effects. This analysis is currently being undertaken.
Publication bias clouds the interpretation of meta-analyses (Sena et al, 2010). Here, estimates of efficacy on infarct were revised downward by 10.7% to 28.7%, although neurological score effects remained the same. Techniques to correct for bias are not without critics, and there are many reasons for funnel plot asymmetry other than publication bias (e.g., poor methodological quality of smaller studies, true heterogeneity, other selection biases, chance) (Higgins and Green, 2006). Nevertheless, the similarity of the bias-adjusted estimate (28.7%) to the overall effect found in a broad sweep of neuroprotectives (O'Collins et al, 2006) provides further evidence that there may be a substantial positive ‘offset’ in preclinical neuroprotection publications.
Because this meta-analysis is not based on direct comparisons of different combination treatments under identical conditions and because the range of testing is likely to be low (O'Collins et al, 2009), it is not possible to recommend one particular approach to combination therapy. Such considerations are further constrained by the impact of additional therapies given in clinical trials as part of standard care (Lees, 2002), and in animal experiments as part of periprocedural treatments such as anesthetics (Danton and Dietrich, 2004).
Combining data are important if we are to critically examine not just combination therapy, but the validity and utility of animal models themselves. However, as demonstrated by the NXY059 animal data (Macleod et al, 2008; Savitz, 2007), careful analysis of individual experiments is critical. Both approaches can coexist and both approaches are important.
Conclusion
Combining two treatments brings additional benefits for the treatment of acute ischemic stroke in animals, although findings are constrained by potential publication bias and heterogeneity. We have yet to discover a magic bullet for acute stroke, but there is room for some optimism in the development of combination therapy as a viable therapeutic strategy.
Footnotes
Acknowledgements
The authors extend their thanks and appreciation to the following researchers: Ana Antonic and Candace Loy for ordering several papers used in this analysis; Dr Emily Sena for her advice on STATA syntax; Dr Leonid Churilov for his comments on adjusted sample sizes; Dr Neil Spratt, Dr Peter Batchelor, and Dennis Young for their comments on combination neuroprotection.
DWH, GAD, and MRM have been the recipients of industry and government awards for research into neuroprotection. VOC was the recipient of an APA scholarship. While no author has been involved in studies included in this paper, they have an interest in developing effective combination therapy for acute ischemic stroke.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.