
Abstract
Studies in transgenic mice overexpressing amyloid precursor protein (APP) demonstrate impaired autoregulation of cerebral blood flow (CBF) to changes in arterial pressure and suggest that cerebrovascular dysfunction may be critically important in the development of pathological Alzheimer's disease (AD). Given the relevance of such a finding for guiding hypertension treatment in the elderly, we assessed autoregulation in individuals with AD. Twenty persons aged 75±6 years with very mild or mild symptomatic AD (Clinical Dementia Rating 0.5 or 1.0) underwent 15O-positron emission tomography (PET) CBF measurements before and after mean arterial pressure (MAP) was lowered from 107±13 to 92±9 mm Hg with intravenous nicardipine; 11C-PIB-PET imaging and magnetic resonance imaging (MRI) were also obtained. There were no significant differences in mean CBF before and after MAP reduction in the bilateral hemispheres (−0.9±5.2 mL per 100 g per minute,
Keywords
Introduction
Considerable evidence links cerebrovascular disease with the development and expression of Alzheimer's disease (AD) (Farkas and Luiten, 2001; Jellinger, 2002). Both share risk factors, such as hypertension, diabetes mellitus, and hyperlipidemia, and ischemia may trigger or worsen amyloid deposition (Kalaria, 2000; Kudo et al, 2000). Furthermore, AD is associated with nonatherosclerotic disease of small blood vessels and infarcts with a predilection for cortical borderzones (Suter et al, 2002). Periventricular white matter lesions, presumably caused by incomplete ischemia, occur in many individuals with AD (Brun and Englund, 1986; Barber et al, 1999). Although the close association of cerebrovascular disease with AD has been well established by clinical studies, the pathophysiological mechanism for this association has not.
Studies in transgenic mice overexpressing amyloid precursor protein (APP) demonstrate globally impaired autoregulation of cerebral blood flow (CBF) to changes in arterial pressure, suggesting that cerebrovascular dysfunction may be of critical importance in the development of pathological AD (Zhang et al, 1997; Niwa et al, 2002). If autoregulation is disordered, moderate reductions in arterial pressure within the normal autoregulatory range will lead to cerebral hypoperfusion, favoring amyloid deposition in the brain (Kalback et al, 2004). Globally impaired autoregulation would produce ischemic damage predominantly in the cortical borderzones and in periventricular white matter (Matsushita et al, 1994), regions that are selectively affected by ischemia in AD (Brun and Englund, 1986; Suter et al, 2002). If autoregulation is intact, the causal relationship between β-amyloid and autoregulatory dysfunction suggested by the APP mouse model would need to be questioned.
Given the potential clinical importance that knowledge of disordered cerebrovascular control would have on management of hypertension in the elderly, we performed a quantitative 15O-positron emission tomography (PET) study to test the hypothesis that individuals with clinically diagnosed AD have impaired autoregulation of CBF.
Materials and methods
Participants
Participants were recruited from the Washington University Alzheimer's Disease Research Center, which evaluates individuals 60 years and older who are cognitively healthy or demented. Details about the recruitment and assessment methods for these individuals have been published (Berg et al, 1998). Participants were eligible for inclusion in this study if they were at least 60 years old, met the NINCDS-ADRDA (National Institute of Neurological and Communicative Diseases and Stroke/Alzheimer's Disease and Related Disorders Association) criteria for a clinical diagnosis of probable AD, and had a Clinical Dementia Rating (CDR) (Morris, 1993) of 0.5 (very mild dementia) or 1 (mild dementia). Exclusion criteria included a mean arterial pressure (MAP) of <90 mmHg (as measured by arterial catheter before PET scanning), a history of stroke, carotid artery stenosis >70% (as determined by carotid Doppler ultrasound performed before PET scanning), a known allergy to calcium channel blockers, a known history of hemodynamically significant aortic stenosis, or contraindications for magnetic resonance imaging (MRI). Informed consent with written documentation was obtained from participants with cosignature from a legally authorized representative. The study was approved by the Human Research Protection Office and the Radioactive Drug Research Committee of Washington University.
The following demographic and clinical data were recorded: age, gender, race, age at dementia onset, apolipoprotein E genotype, and a general medical history including history of hypertension and use of antihypertensive medications. The CDR, CDR sum of boxes (a more quantitative representation of the CDR (Berg et al, 1992)), and minimental state exam (Folstein et al, 1975) scores from the most recent annual Alzheimer's Disease Research Center evaluation were recorded as well.
15O-Positron Emission Tomography Studies
All participants were studied on an ECAT EXACT HR 47 PET scanner (Siemens/CTI, Knoxville, TN, USA) located in the Neurology-Neurosurgery Intensive Care Unit at Barnes-Jewish Hospital. This scanner collects 47 contiguous transverse slices encompassing an axial field of view of 15 cm. Spatial resolution is ∼4.3 mm full width at half maximum at the center of the field of view. Antihypertensive medications were held on the morning of the study. All participants had a radial arterial catheter placed for continuous measurement of arterial pressure and for arterial blood sampling and a venous catheter placed in a peripheral arm vein for administration of radiotracers and nicardipine infusion. The PET scanner was calibrated for conversion of PET counts to quantitative radiotracer concentrations. Emission data were obtained in the 2D mode (interslice septa extended) and reconstructed with filtered backprojection with a ramp filter cutoff at the Nyquist frequency using measured attenuation, scatter, and randoms corrections.
The MAP (defined as 2/3 of diastolic plus 1/3 of systolic blood pressure) and heart rate were monitored throughout the entire PET study except for during acquisition of the PET emission data when arterial blood was being sampled. Partial pressure of carbon dioxide in the blood was measured by arterial blood gas analysis immediately before each emission scan.
The CBF was measured using an adaptation of the Kety autoradiographic method with a 40-second emission scan after rapid intravenous injection of 50 mCi of 15O-labeled water (Raichle et al, 1983; Videen et al, 1987). Simultaneously with acquisition of the PET emission data, arterial blood was sampled, and the arterial activity curve was determined using a scintillation counter calibrated to the same well counter as the PET scanner. The arterial time–radioactivity curve recorded by the sampler was corrected for delay and dispersion using previously determined parameters. Baseline measurement of CBF was performed. An intravenous infusion of nicardipine was then started at 2.5 mg/h and titrated up to a maximum of 15 mg/h to achieve a reduction in MAP by 10 to 15mmHg from baseline. The MAP was held constant at this level for 7 to 10 minutes before repeat CBF measurement, sufficiently long to permit the cerebrovascular responses to MAP reduction to reach a new steady state (Kontos et al, 1978). A clinical assessment was performed at baseline and after blood pressure lowering by asking participants about symptoms of focal (lateralized weakness, numbness, visual difficulty, or language problems) or general cerebral hypoperfusion (lightheadedness, bilateral visual problems, tinnitus) and testing immediate memory with digit span. After completion of the repeat CBF measurement, nicardipine infusion was stopped, allowing MAP to return quickly to baseline.
11C-PIB-Positron Emission Tomography Studies
Amyloid imaging was performed using 11C-Pittsburgh Compound B (11C-PIB) in 19 subjects (Mathis et al, 2003). The PET scans were obtained using either a Siemens ECAT EXACT HR 47 scanner or an ECAT EXACT HR+ PET scanner (Siemens/CTI) on a separate day from the 15O-PET scan. All participants had a venous catheter placed in a peripheral arm vein for administration of radiotracers. Simultaneous with intravenous administration of 10 to 20mCi of 11C-PIB, a 60-minute dynamic PET scan in 3D mode (septa retracted) was initiated. Images were reconstructed with filtered backprojection with a ramp filter cutoff at the Nyquist frequency using measured attenuation, model-based scatter, and randoms corrections.
Magnetic Resonance Imaging Studies
All participants underwent brain MRI scanning using Magnetom Sonata 1.5T or Trio 3T scanners (Siemens, Erlangen, Germany). A midsagittal scout T1-weighted spin-echo pulse sequence was used for positioning. A 3D MPRAGE (Magnetization Prepared Rapid Acquisition Gradient Echo) sequence (TR (repetition time) = 2400 milliseconds, TE (echo time) = 3.16milliseconds, TI (inversion time) = 1000milliseconds, FA (Fractional Anisotropy) = 8°, 1 × 1 × 1 mm3 voxels) produced a high-resolution T1-weighted image. T2-weighted images were obtained using FLAIR (Fluid Attenuated Inversion Recovery) (
Data Analysis
The CBF images were aligned to MR anatomic images (Woods et al, 1993), coregistered to a standard mean CBF image in Talairach atlas space (Woods et al, 1992; Talairach and Tournoux, 1998), and masked to exclude noncerebral structures. Hemispheric CBF measurements were made using a mask in Talairach space restricted to brain between
Composite 11C-PIB-PET images of PET counts were created from dynamic scans collected 40 to 60 minutes after PIB injection, filtered to a 3D resolution of 8 mm full width at half maximum, normalized to cerebellar gray matter, and coregistered with the two CBF scans for each subject. An automated search routine using a 1-cm sphere identified all PIB peaks separated by at least 16 mm (2 × full width at half maximum) within the proscencephalon of each subject. The 10% of all peaks with the highest PIB deposition were identified. PIB uptake in these peaks was at least 2.5 times that of cerebellar gray matter (Jack Jr et al, 2009). For 11 subjects in whom these peaks comprised at least 10 mL, mean CBF values within the spheres were computed before and after blood pressure reduction. The remaining eight subjects had 0 to 3 peaks each sampling <2 mL, which was not large enough for meaningful CBF comparisons.
The CBF measurements were also obtained in 1-cm diameter spheres placed in the cortical borderzones as identified on MRI (Carpenter et al, 1990). In each hemisphere, one region was placed in the anterior borderzone located in the depths of the superior frontal sulcus where the pial anastomoses between the orbitofrontal branches of the middle cerebral artery and the anterior frontal branches of the anterior cerebral artery occur, and two were placed in the posterior borderzone located in the inferior interparietal sulcus where the pial anastomoses between the temporal branches of the middle cerebral and posterior cerebral arteries occur.
The CBF measurement within regions of leukoaraiosis was restricted to the eight participants with Atherosclerosis Risk in Communities leukoaraiosis scores (Wong et al, 2002) of ≥ 5, as regions in participants with lower scores would necessarily comprise narrow bands too small to obtain meaningful PET data. Regions were defined by thresholding only the larger aggregates of high-intensity areas in T2-weighted MR images and then resampling these regions in the coregistered PET.
The cerebral autoregulatory index was calculated as the ratio of the percentage change in CBF and the corresponding percentage change in MAP, where an autoregulatory index of 0 would indicate perfect autoregulation.
The presence and size of radiographic cerebral infarcts (<1.5 or ≥ 1.5cm) evident on T2-weighted MRI sequences and the number and location of microbleeds (deep, lobar, or infratentorial) evident on gradient-echo MRI sequences were recorded. Microbleeds were defined as 2 to 10 mm rounded areas of homogeneous signal loss on gradient echo images. Symmetric areas of hypointensity in the globus pallidus (considered to represent calcification or iron deposition) and hypointensities in cortical sulci or in areas of cortex near the inner table of the skull (considered to represent blood vessels or signal averaging from adjacent bone) were excluded. The degree of leukoaraiosis was scored on T2-weighted MRI sequences using the 9-point scale described in the Atherosclerosis Risk in Communities study (Wong et al, 2002).
Mean cortical binding potential values for PIB were calculated as the average of binding potentials in prefrontal cortex, precuneus, laterotemporal cortex, and gyrus rectus (Mintun et al, 2006).
The CBF before and after blood pressure reduction was compared by paired
Results
Twenty-three individuals were enrolled in the study. The PET scanning was not performed in two because MAP as measured by arterial catheter was <90 mm Hg. One was excluded due to technical difficulties during the 15O-PET scan. Clinical and radiographic characteristics of the remaining 20 participants are shown in Table 1 and Supplementary Table 1.
Clinical and radiographic characteristics
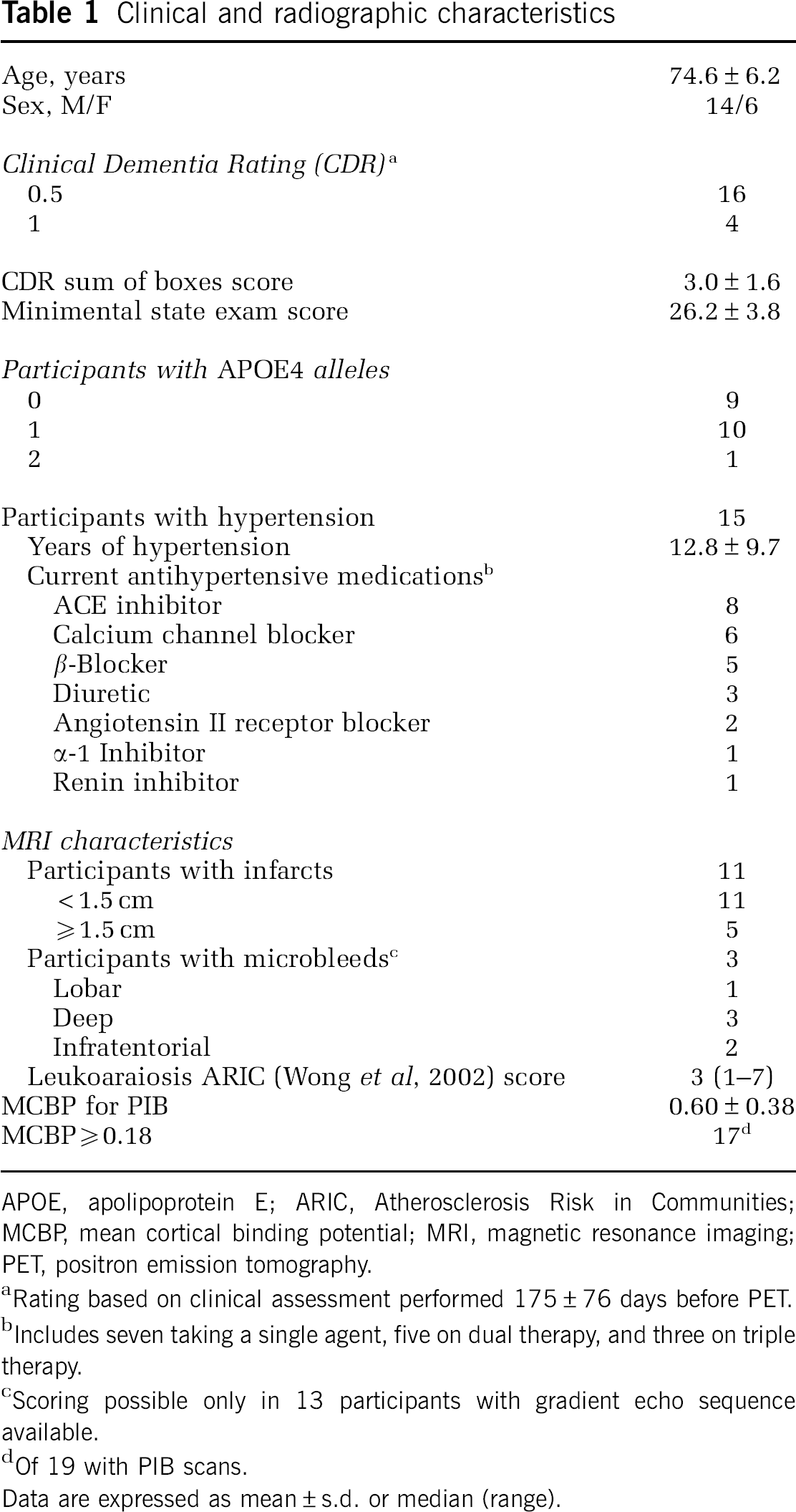
APOE, apolipoprotein E; ARIC, Atherosclerosis Risk in Communities; MCBP, mean cortical binding potential; MRI, magnetic resonance imaging; PET, positron emission tomography.
Rating based on clinical assessment performed 175 ± 76 days before PET.
Includes seven taking a single agent, five on dual therapy, and three on triple therapy.
Scoring possible only in 13 participants with gradient echo sequence available.
Of 19 with PIB scans.
Data are expressed as mean ± s.d. or median (range).
Mean arterial pressure was lowered 14.6 ± 5.6 mmHg (13.5%) from a baseline of 107.0 ± 12.6 mm Hg without clinical change or other adverse event. There was a concomitant 12% increase in heart rate (
There was no significant change in CBF within the bilateral cerebral hemispheres (−0.9 ± 5.2mL per 100g per minute,
Change in mean arterial blood pressure (MAP) and cerebral blood flow (CBF)
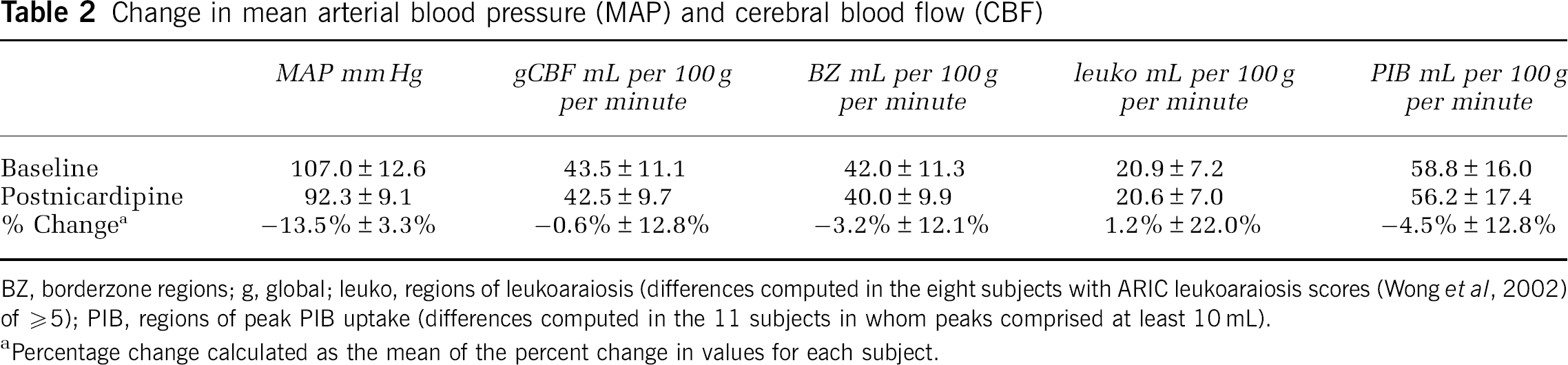
BZ, borderzone regions; g, global; leuko, regions of leukoaraiosis (differences computed in the eight subjects with ARIC leukoaraiosis scores (Wong et al, 2002) of ≥ 5); PIB, regions of peak PIB uptake (differences computed in the 11 subjects in whom peaks comprised at least 10 mL).
Percentage change calculated as the mean of the percent change in values for each subject.
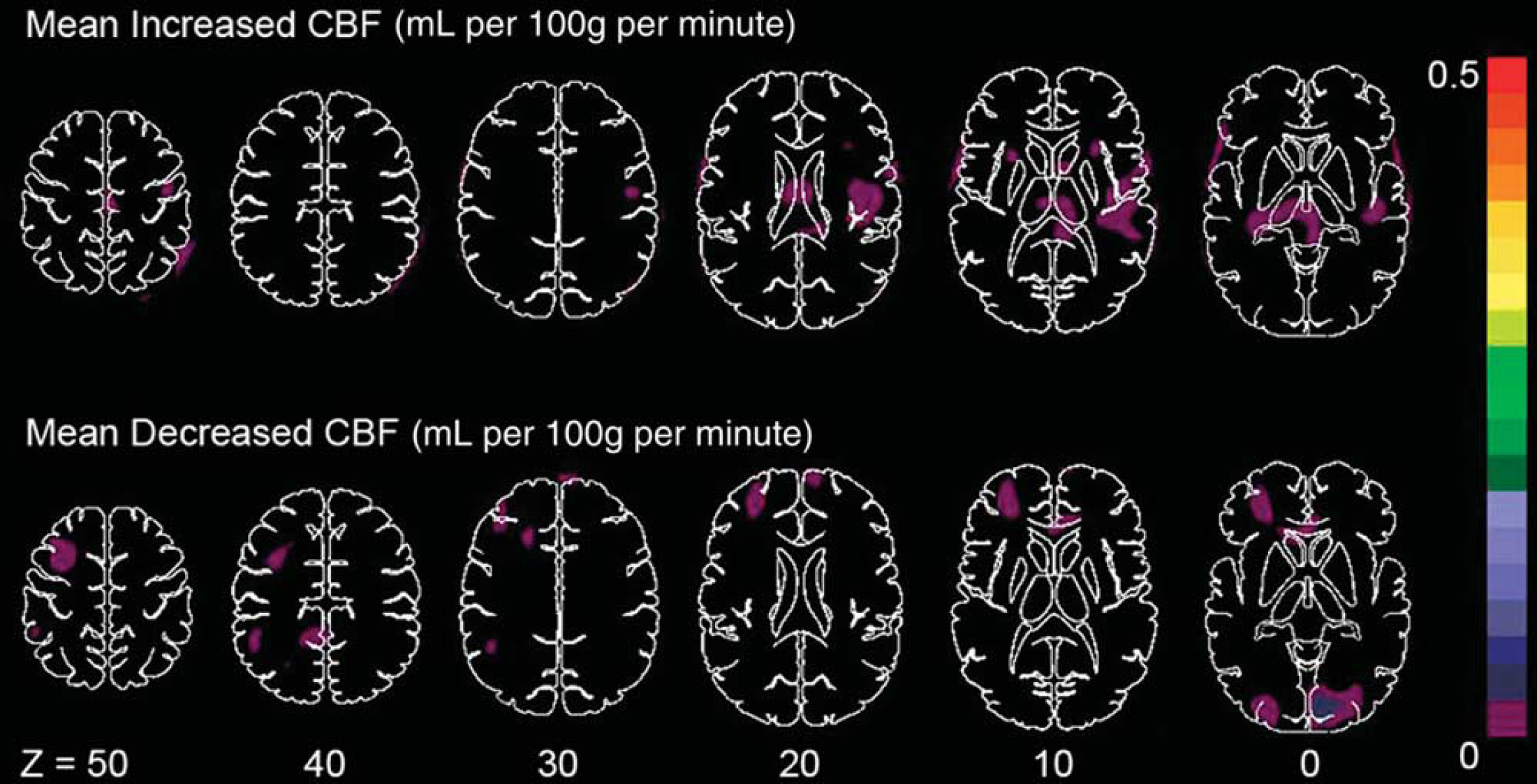
Composite mean cerebral blood flow (CBF) difference image. Composite mean difference image of all 20 participants, showing that the maximum mean decrease in CBF anywhere in the brain is <0.1 mL per 100 g per minute or <0.2%.
Discussion
In this study of 20 individuals with mild AD, we did not find autoregulatory impairment globally or in cortical borderzones, regions of leukoaraiosis, or regions of high-PIB uptake with a 10 to 15mmHg reduction in MAP within the normal autoregulatory range. Our results suggest that impaired autoregulation is unlikely to be of pathogenic importance in the development of AD.
We targeted a blood pressure reduction sufficient enough to determine if autoregulation is impaired but not to a degree that it fell outside the normal autoregulatory range. Strandgaard (1976) found that the lower limit of autoregulation was 25 mmHg below resting blood pressure in normotensive and 20mmHg below in well-controlled hypertensive individuals. Using a computerized method, Schmidt et al (1990) reported smaller decreases of 13 mmHg for normotensive and 18mmHg for hypertensive individuals before the lower limit was reached. We achieved a blood pressure reduction of 13mmHg in our normotensive and 15 mmHg in our chronically hypertensive subjects. Had our subjects behaved similarly to the transgenic mice overexpressing APP, the 14.6 mmHg reduction in MAP within the normal autoregulatory range that we achieved would have been expected to produce a 16.8% reduction in CBF in severely impaired autoregulation and a 11.5% reduction in moderately impaired autoregulation (Niwa et al, 2002). Instead, we observed only a nonsignificant 0.6% decrease in hemispheric CBF in our subjects. In addition, the autoregulatory index we determined is well within the normal autoregulatory index range of 0 to 0.4 reported in other studies using various species and protocols (Kawamura et al, 1975; Donegan et al, 1985; Jones et al, 2002). Although there was some variability in the percentage change in CBF from subject to subject, such variability in response to a reduction in blood pressure is a known phenomenon in normal animals (Jones et al, 2002). Both a paradoxical rise in CBF as perfusion pressure is dropped (hyperautoregulation) and a linear response of CBF to perfusion pressure changes have been reported within the control group of normal animals. Thus, an aggregate autoregulation index from all subjects provides the most meaningful data.
Our methodology has been demonstrated to be sensitive enough to detect changes in CBF with physiological manipulations in human subjects (Diringer et al, 2000; Jost et al, 2005). Using this method, we have observed clinically evident autoregulatory dysfunction in the MAP range above the lower limit but during induced moderate hypotension (Powers et al, 2009). Had we found a decrease in CBF with blood pressure reduction within the normal autoregulatory range in this study, data from normal control subjects would have been important to ensure that the decrease was significantly different from normal. However, we observed <1 mL per 100g per minute change in CBF in our subjects, which is clinically irrelevant whether or not it differs from controls.
Before this study, comparable data on autoregulation of CBF in patients with AD did not exist. Two groups have reported preserved vascular reactivity to changes in arterial CO2 in patients with AD (Kuwabara et al, 1992; Nagata et al, 1997, 2002). As CO2 reactivity and autoregulation may be dissociated (Fieschi et al, 1968; Paulson et al, 1972), these observations do not bear on the issue of autoregulation. Passant et al (1996) measured cortical CBF with Xenon-133 inhalation in 13 subjects with AD and severe orthostatic hypotension. Although they report no change in CBF, the results are difficult to interpret. As the CBF measurement took place over 11 minutes and the blood pressure was fluctuating during this period, it is not possible to obtain an accurate CBF measurement with this steady state technique.
In addition, no CBF data from white matter or deep gray matter structures can be obtained with this technique. We chose subjects in the early stages of AD (CDR 0.5 and 1) for this study. Even in the earliest stages, histological criteria of AD are demonstrable in the majority of individuals—>90% of those who die at the CDR 0.5 or 1 stage have neuropathological AD (Storandt et al, 2006). All but two of the 19 participants who had PIB scans had elevated PIB binding. In our previous work, we found that participants with dementia of the Alzheimer type typically showed mean cortical binding potential values for PIB of ≥ 0.18 (Mintun et al, 2006), but that PIB binding can be negligible even in individuals with a CDR of 0.5 and pathologically proven AD (Cairns et al, 2009). Explanations for a ‘negative’ PIB scan include misdiagnosis in which the clinical dementia is not due to AD and inability of PIB to detect AD variants that are characterized predominantly by diffuse amyloid plaques. Our data do not allow us to address whether autoregulatory impairment occurs in the late stages of human AD, but this information would have low clinical relevance as intervention to prevent progression at this stage would be of little value.
Because of the exclusion criterion of an MAP <90 mm Hg, the mean MAP of 107 mm Hg in our participants was higher than normal and three quarters of them had a history of hypertension. Although chronic hypertension shifts the autoregulatory curve to higher pressures, it does not lengthen the autoregulatory plateau and so would not be expected to alter the interpretation of our negative results. In fact, the autoregulatory plateau may actually be shorter in some hypertensive individuals (Strandgaard, 1983).
Evaluating the status of autoregulation is complicated by the effects of antihypertensive agents on the cerebral vasculature. We chose intravenous nicardipine for this study because we have used it to produce acute MAP reductions of 16 to 23 mm Hg in patients with acute intracerebral hemorrhage and ischemic stroke without any change in CBF (Powers et al, 2001, 2009). Many of the participants in this study were being treated with antihypertensive agents, but none of the agents has been shown to impair autoregulation with chronic use.
In conclusion, a reduction in arterial pressure within the normal autoregulatory range in individuals with AD did not reduce CBF globally or in cortical borderzones, regions of leukoaraiosis, or regions of high-PIB uptake. Unlike in animal models of AD, impaired autoregulation of CBF to changes in arterial pressure is not present in early AD and is therefore unlikely to be important in the development of pathological AD in humans. Our data suggest that the association between β-amyloid and autoregulatory dysfunction in the APP mouse model may be an epiphenomenon that has no bearing on the cerebrovascular consequences of human AD; thus caution is warranted in applying this aspect of the APP mouse model to human AD.
Footnotes
Acknowledgements
The authors thank Angela M Shackleford, RN, for coordinating and assisting in the performance of the studies; Lennis L Lich for help in performing the PET studies; the cyclotron staff at Washington University for production of radiotracers; John T Hood Jr for help with data analysis; the Clinical and Genetics Cores of the Washington University Alzheimer Disease Research Center for participant evaluations and apolipoprotein E genotype; and Mark Mintun, MD, for helpful discussions.
Dr Morris previously was involved in clinical trials of molecular imaging agents for β-amyloid sponsored by Avid Pharmaceuticals, MH, but has no current disclosures.