
Abstract
The objective of the present study was to evaluate fetal cerebral circulation by using three-dimensional (3D) power Doppler ultrasound in normal and growth-restricted fetuses. A total of 100 normal grown fetuses were compared with other 25 with growth restriction (FGR). Three-dimensional power Doppler ultrasound was used to assess fetal cerebral 3D vascular indices: vascularization index, flow index (FI), and vascularization flow index (VFI). Both FI and VFI correlated positively with gestational age. On average, all the 3D vascular indices were increased in fetuses with FGR. The proportion of fetuses detected as having hemodynamic redistribution was higher when using 3D power Doppler indices than by means of the middle cerebral artery pulsatility index (52% versus 20%,
Keywords
Introduction
Three-dimensional (3D) quantification of blood flow information obtained from color Doppler has been used in normal fetuses to describe blood flow along pregnancy in several organs (Chang et al, 2003a, b , c ). Liver, kidney, and brain have been studied showing increasing blood flow patterns as gestation progresses. Also this technique has been used to study samples of placental circulation (De Paula et al, 2009). However, up to now, little is known about the clinical usefulness of this technology in pregnancy complications.
Because the analysis of fetal brain circulation is of great interest when following up fetuses with growth restriction (FGR), 3D power Doppler studies may add valuable information to that obtained from 2D standardized Doppler evaluation.
Hemodynamic redistribution, which consists of blood flow redistribution toward essential fetal organs (brain, heart, and adrenal glands) at the expense of the other organ systems (lungs, kidneys, and bowel), represents one of the major fetal mechanisms to preserve vital organs, such as brain, from hypoxic damage. Currently this situation is normally diagnosed by using a combination of color and pulsed Doppler detecting decreased vascular impedance, usually caused by vasodilatation, at the middle cerebral artery (MCA). However, this technique has limitations: first, it analyses one single vessel, so circumstances that may be occurring in other brain areas may be not well represented by these measurements. Second, its reliability depends strongly on several technical aspects including a correct view, an appropriate insonation angle, and an adequate selection of the segment of the artery to be studied. Finally it evaluates only arterial but not venous blood flow, which has been suggested to have an additional value to discriminate between fetal adaptation and fetal decompensation in chronic fetal hypoxia (Senat et al, 2000). Potentially, 3D power Doppler mode does not have these limitations. This technique let us to study the whole-brain circulation, including arterial and venous vessels and technically, it does not require so many conditions to be reliable.
The aim of the present study was to build normal ranges for 3D power Doppler indices of fetal cerebral circulation throughout pregnancy and to compare these indices between normal grown fetuses and those with growth restriction. Moreover, the rate of fetuses having hemodynamic redistribution when using 3D power Doppler ultrasound (cases with measures out of the normal range) was compared with that diagnosed by standard pulsed and color Doppler technique.
Materials and methods
A total of 135 pregnant women were studied. Of them, 110 were healthy women who attended our ultrasound clinic for routine growth scans between 17 and 41 weeks of gestation with normal fetal growth (more than 10th centile of both abdominal circumference and estimated fetal weight). All of them were followed up and 10 of them subsequently developed FGR, so they were excluded from the study. They were not considered to be included in the FGR group because when they were scanned, the fetuses had normal growth. Data from the rest of the 100 women, considered as the control group, were used to construct normal ranges for 3D power Doppler indices along pregnancy. The distribution of the 100 measurements along gestation was as follows: 4 before 20 weeks, 19 between 21 and 25 weeks, 20 between 26 and 30 weeks, 34 between 31 and 35 weeks, and 23 between 36 and 41 weeks. There were no cases of either preeclampsia or preterm delivery. So the duration of time between the ultrasound measurement and delivery in each case was the difference between the gestational age at study week and full-term pregnancy (37 to 41 weeks). The other 25 women were cases of FGR who attended our Fetal Medicine unit for assessment. Scans for the study were performed at the first visit to the Unit; most of them after the diagnosis of FGR. The interval between the ultrasound examination and delivery was 2.52 ± 2.15 weeks (range 0 to 7 weeks). Fetal growth restriction was first defined by a fetal abdominal circumference below the fifth percentile for gestation and second, at delivery all infants had a weight below the fifth percentile for gestation. All of them had Doppler-defined placental insufficiency defined by a pulsatility index (PI) in the umbilical artery greater than 97.5th percentile for gestation.
The study was approved by the local research ethical committee and all women signed an informed consent to participate in the study.
Transabdominal sonography was performed by one of two operators (JLB or EM). In 30 cases, both operators scanned the fetuses to estimate the repeatability of the technique. When a woman was scanned for the two operators to calculate the interobserver repeatability, the first measurement was registered for the study. The second measurement was masked to the first operator until the final analysis. The equipment used was a GE Voluson 730 Expert ultrasound system (GE Healthcare, Zipf, Austria) equipped with a 5 MHz transabdominal obstetric transducer.
Before the study, measurements were obtained to assess fetal growth, amniotic fluid volume, and pulsatility and resistance indices in the umbilical artery, in both uterine arteries and in the MCA. Peak systolic velocity was also measured in the MCA. In addition, fetal anatomy was checked and no fetal anomalies were found.
Oligohydramnios was considered if amniotic fluid index was under the fifth centile for gestational age (Moore and Cayle, 1990).
Hemodynamic redistribution was defined according to the following criteria: for MCA measurements, as the presence of a PI in the fetal MCA below the fifth centile for gestational age (Parra-Cordero et al, 2007); for the 3D power Doppler indices as the presence of a value of vascularization index (VI), flow index (FI), or vascularization flow index (VFI) above the 95th centile for gestational age.
Scans of the cerebral circulation were performed with the woman in a semirecumbent position and during fetal apnea. The fetal head was scanned in its transverse plane at the level of the base of the skull. Middle cerebral artery Doppler assessment was performed as previously described (Mari et al, 1995). The pulsed Doppler gate was placed in the proximal one-third of the MCA, with the angle between the ultrasound beam and blood flow kept as close as possible to 0° and, in all cases, was less than 20°. An appropriate high-pass filter was chosen and when the end-diastolic flow was absent this was reduced to 65 Hz.
Power Doppler was then activated and switched on to visualize the circle of Willis. Pulse repetition frequency was set to 0.9 kHz. Only when an appropriate view of the complete circle was achieved volume acquisition was performed. The probe was displaced until the biparietal diameter view. Then the system was switched into the 3D mode. The fetal head was centralized within the 3D sector appearing on the ultrasound screen, and data were obtained by holding the transducer stationary whereas its crystals were mechanically rotated across the sector with a sweep angle of 90°. The fast volume acquisition setting was always used to minimize periodic flashing artifacts arising from pulsation of the maternal arteries and from fetal movements. The duration of the volume acquisition was approximately 10 to 15 s. The acquired volumes were stored digitally for analysis offline.
The Virtual Organ Computer-aided AnaLysis (VOCAL) software, which is integrated into the Voluson 730 ultrasound system, was used to calculate the 3D power Doppler indices from the samples of the fetal head obtained from the volume acquired. The contour mode in the VOCAL program was set automatically (generating a sphere between the two contour points). The two contour points were placed onto the anterior and posterior fetal parietal bones, respectively. Once the sphere had been drawn, the body glass mode was used to confirm that the whole circle of Willis was included in the sample (Figure 1; video). Then the 3D power Doppler indices were calculated automatically by using the histogram facility of the VOCAL software. The following Doppler indices were calculated: VI, FI, and VFI. Vascularization index is the ratio of the number of color voxels to the total number of voxels (voxel = smallest unit of volume) in the region of interest, and it reflects the density of blood vessels (Rovas et al, 2005). The voxel size is constant as the brain enlarged but the number of voxels increases as the brain volume increase with gestation. This is the reason to use a ratio color/gray to make the index. Flow index is calculated as the sum of weighted color voxels divided by the number of color voxels, and is related to the energy reflected from the blood corpuscles in the vessels in the region of interest, that is, the more blood corpuscles the higher the FI values. Vascularization flow index is the sum of weighted color voxels divided by the total number of voxels. It reflects both the density of blood vessels and the number of blood corpuscles flowing in the blood vessels. Before calculating the parameters all measurements were repeated at least twice. All 3D ultrasound results were unavailable to the clinical staff.
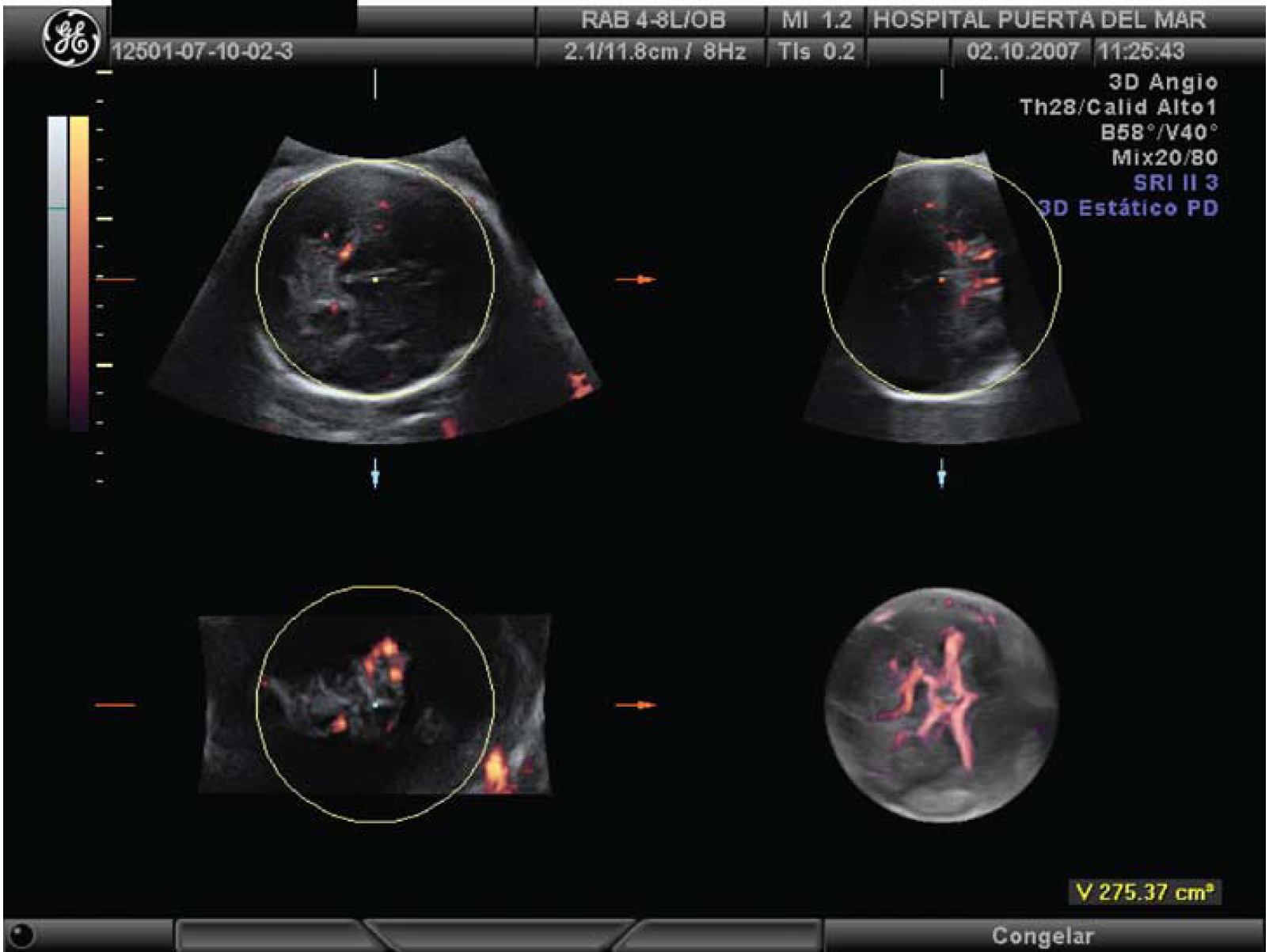
The contour mode in the VOCAL program is set automatically (generating a sphere between the two contour points). The two contour points were placed onto the anterior and posterior fetal parietal bones, respectively. Once the sphere had been drawn, the body glass mode is used to confirm that the whole circle of Willis was included in the sample (see also video).
Distributions of variables were checked by using the Kolmogorov—Smirnov test and the analysis of histograms. If variables followed nonnormal distributions log-transformed values were used for analysis. Blood flow indices (VI, FI, and VFI) were plotted against gestational age and percentiles for gestation were calculated by using the LMS method (Silverwood and Cole, 2007), which provides a general method for fitting smooth centile curves. So, the result of the analysis is not only calculated by the actual observed data but also as a result of calculating the trend of the curves and after the smoothing procedure. The relationships between numeric variables were studied by using both the Pearson correlation coefficient and stepwise linear regression. Inter- and intraobserver reproducibility was assessed with the intraclass correlation coefficient. This is a true index of agreement between observers, in contrast to the conventional Pearson product moment correlation coefficient, which is a measure of linear association rather than of agreement. Intraclass correlation coefficient is derived from a two-way mixed analysis of variance with subjects treated as a random effect and observers treated as a fixed effect. Differences between FGR and control fetuses were studied by using the Student's
Results
Demographics of women participating in the study are shown in Table 1. There were no significant differences between the two studied groups.
Demographics and 3D power Doppler indices
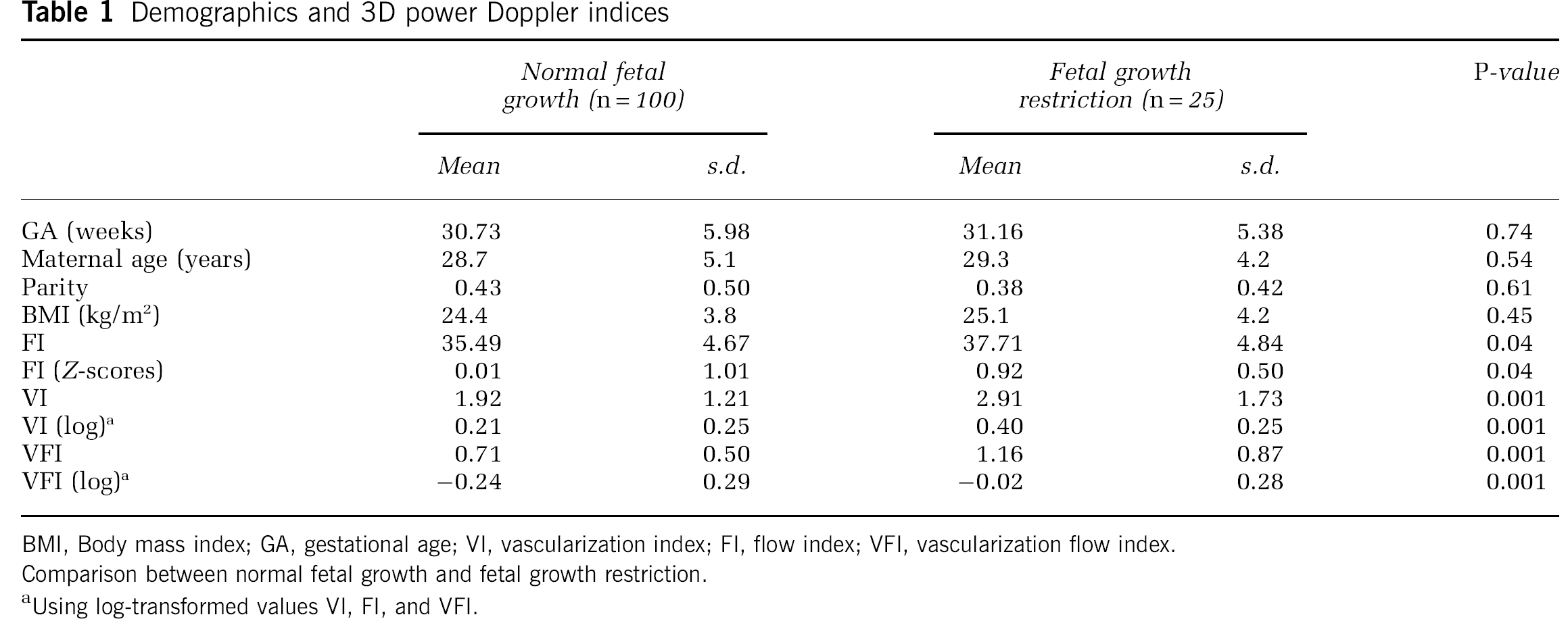
BMI, Body mass index; GA, gestational age; VI, vascularization index; FI, flow index; VFI, vascularization flow index.
Comparison between normal fetal growth and fetal growth restriction.
Using log-transformed values VI, FI, and VFI.
Intraobserver intraclass correlation coefficients were 0.85, 0.96, and 0.92 for FI, VI, and VFI, respectively. Interobserver intraclass correlation coefficients were 0.67, 0.92, and 0.88 for FI, VI, and VFI, respectively. Correlation values between gestational age and the studied variables in normal grown fetuses were analyzed. Flow index increased very significantly with gestational age (
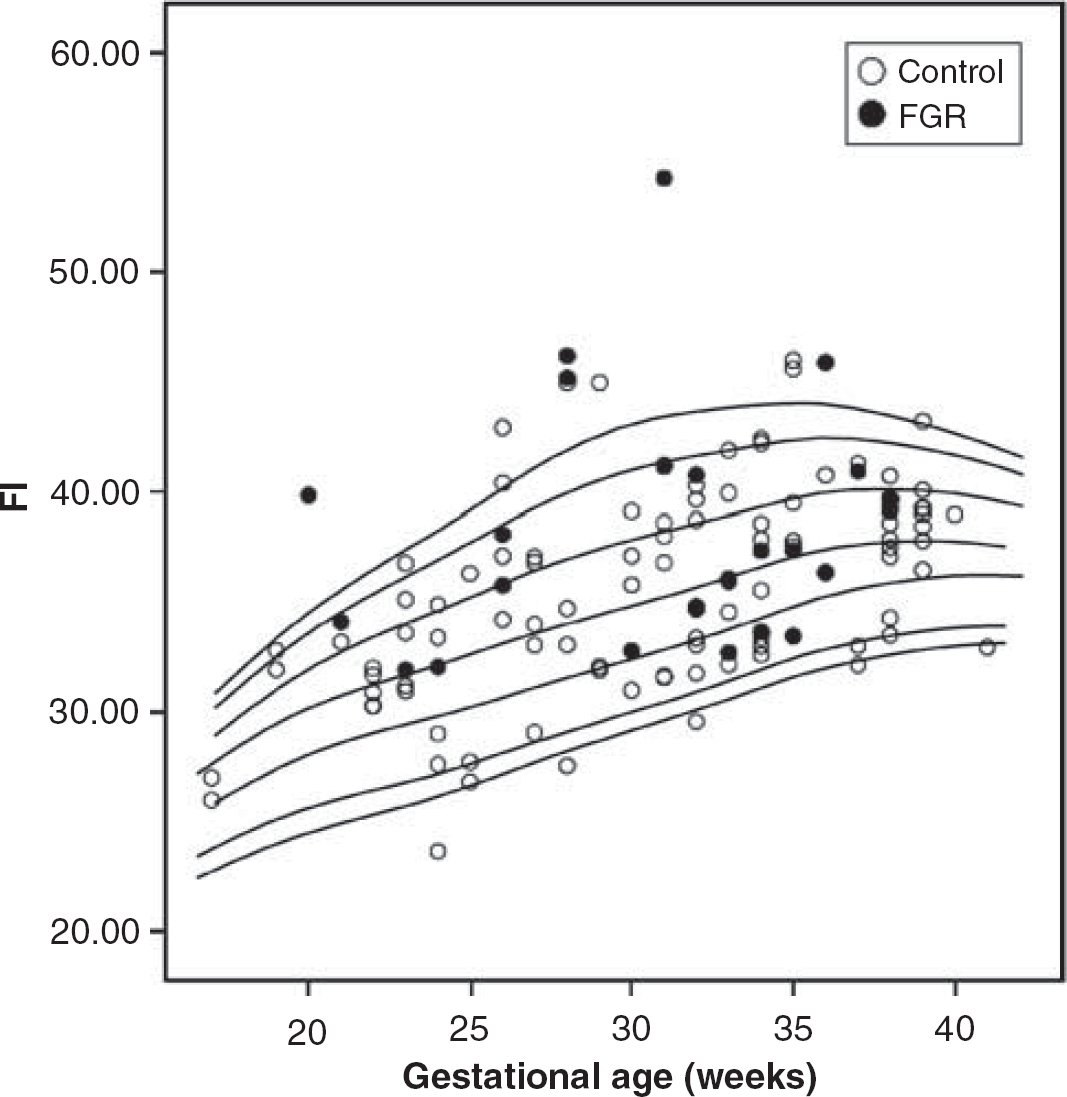
Flow index (FI) throughout pregnancy in normal and growth-restricted fetuses. Lines represent percentiles (p5, p10, p25, p50, p75, p90, and p95) adjusted by the LMS method.
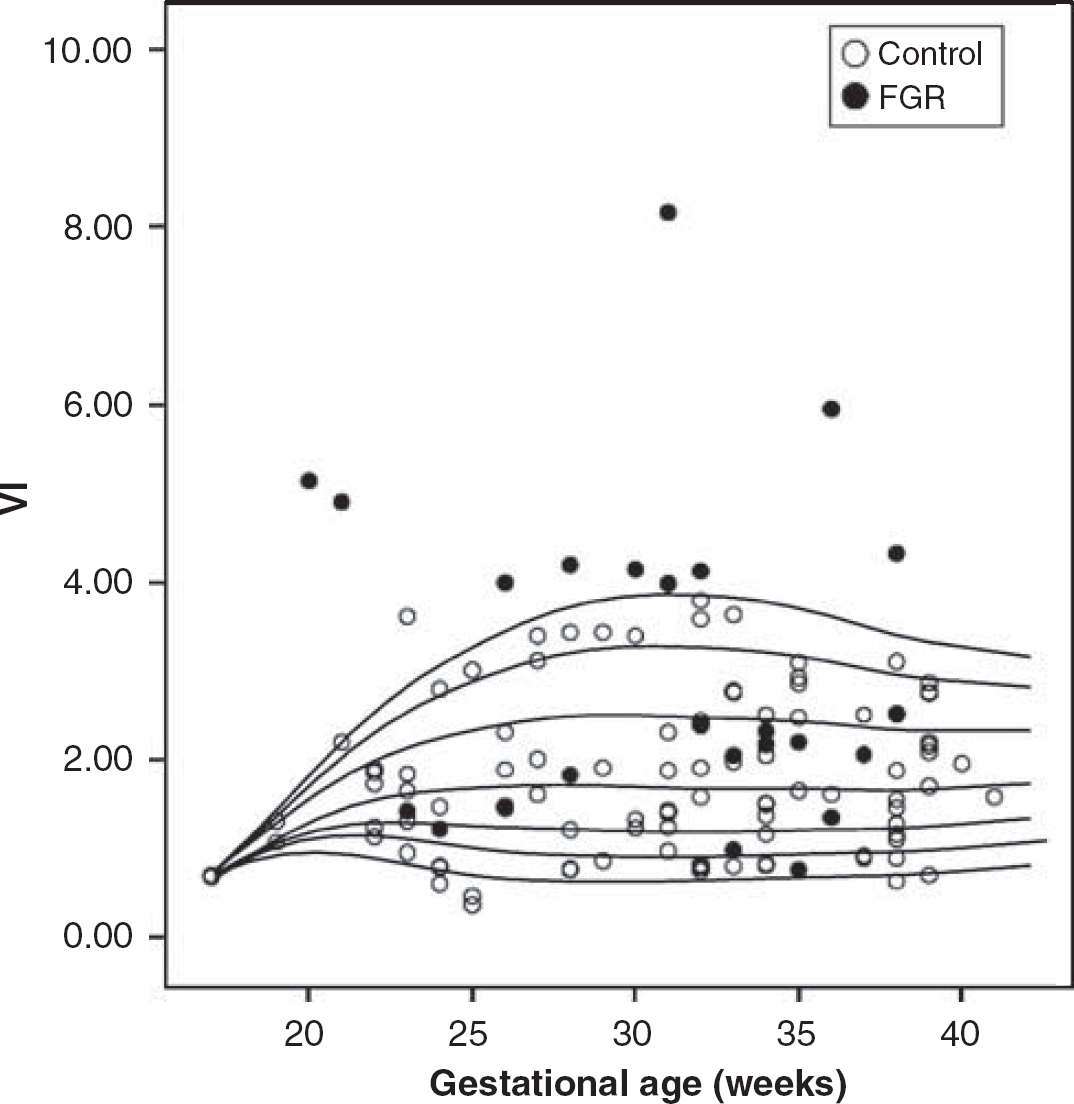
Vascularization index (VI) throughout pregnancy in normal and growth-restricted fetuses. Lines represent percentiles (p5, p10, p25, p50, p75, p90, and p95) adjusted by the LMS method.
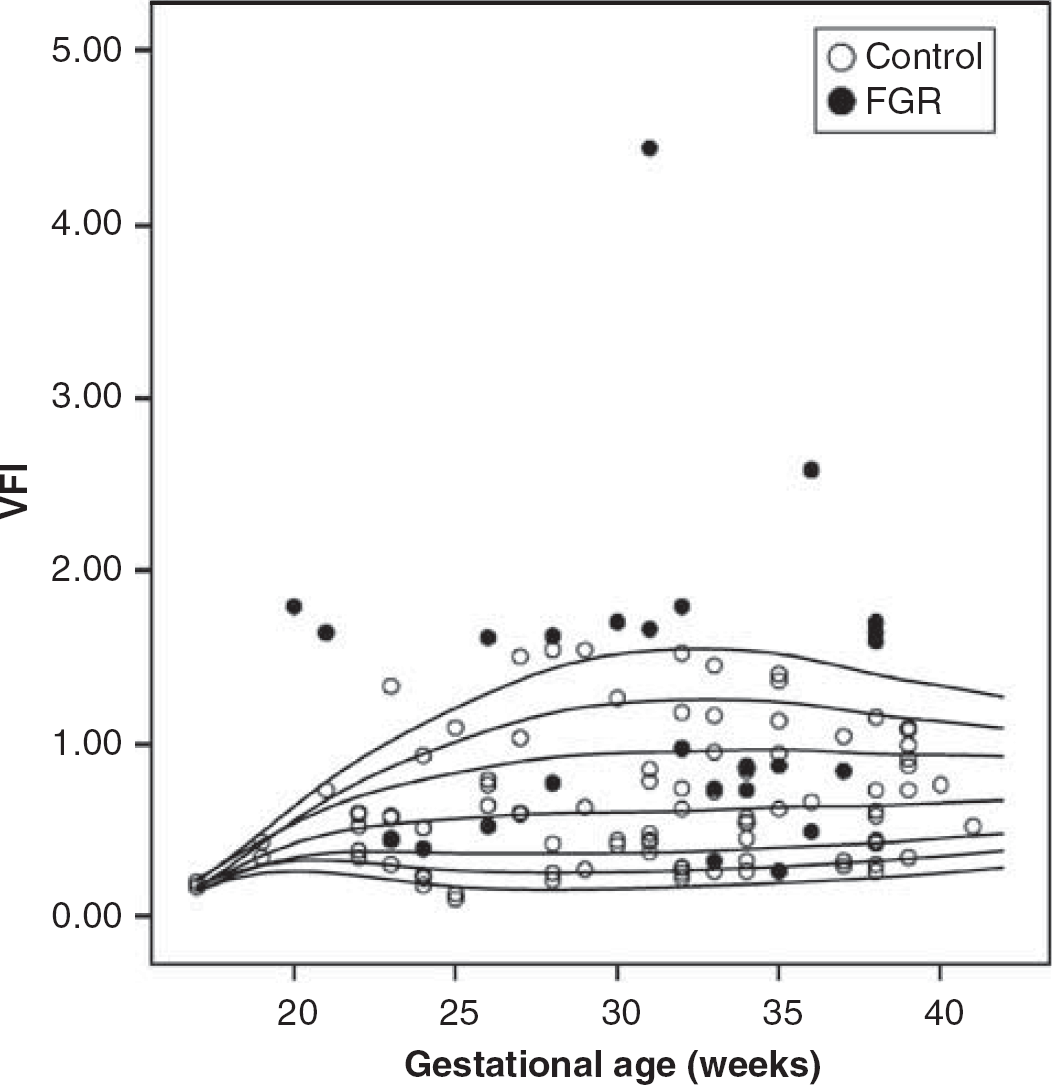
Vascularization flow index (VFI) throughout pregnancy in normal and growth-restricted fetuses. Lines represent percentiles (p5, p10, p25, p50, p75, p90, and p95) adjusted by the LMS method.
Percentiles for the three 3D power Doppler variables according to gestational age were calculated and are shown in Table 2. Nevertheless, there seems to be relatively few changes after 25 weeks for the three 3D indices. Selecting only controls after 25 weeks, only FI had borderline statistical significant correlation with gestational age (
Three-dimensional power Doppler indices percentiles for gestational age
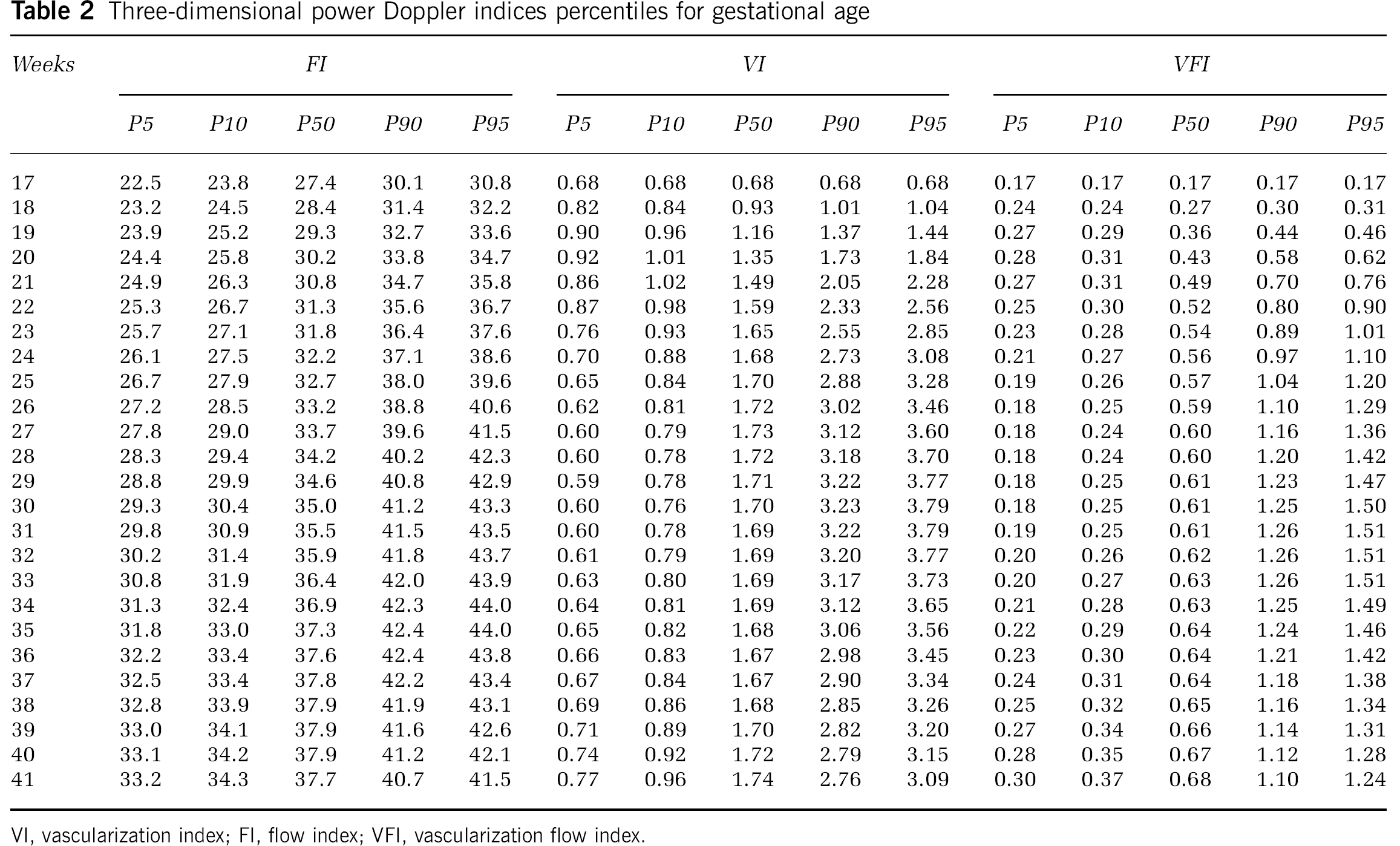
VI, vascularization index; FI, flow index; VFI, vascularization flow index.
Only FI significantly correlated with MCA Doppler measurements (
The three 3D power Doppler indices were significantly higher in fetuses in the FGR group than in those with normal growth (Table 1).
The proportion of fetuses with measurements out of the normal range, suggesting hemodynamic redistribution was much higher when using 3D power Doppler indices (any of the 3D indices >95th centile) than by means of the MCA PI (13 of 25, 52% versus 5 of 25, 20%;
We repeated measurements in some controls (
Estimated fetal weight in the FGR group was 2.6 ± 2.4 centiles (adjusted for gender and gestational age). Estimated fetal weight significantly correlated with both VI (
Caesarean section was the mode of delivery in 13 cases (52%). There were three cases of perinatal mortality, two of them were cases of intrauterine death and the other was a case of neonatal mortality. There was one case of intraventricular hemorrhage, three cases of sepsis, two cases of anemia, one case of thrombocytopenia, and three cases of bronchopulmonary dysplasia. Only FI was abnormal in the 3 cases of perinatal mortality and none of the 20 fetuses with normal FI died. Thus, there was a statistically significant difference in the rate of perinatal death between those fetuses with or without hemodynamic redistribution according to FI (
Sensitivity, specificity, and predictive values to detect perinatal mortality of MCA PI and 3D vascular indices
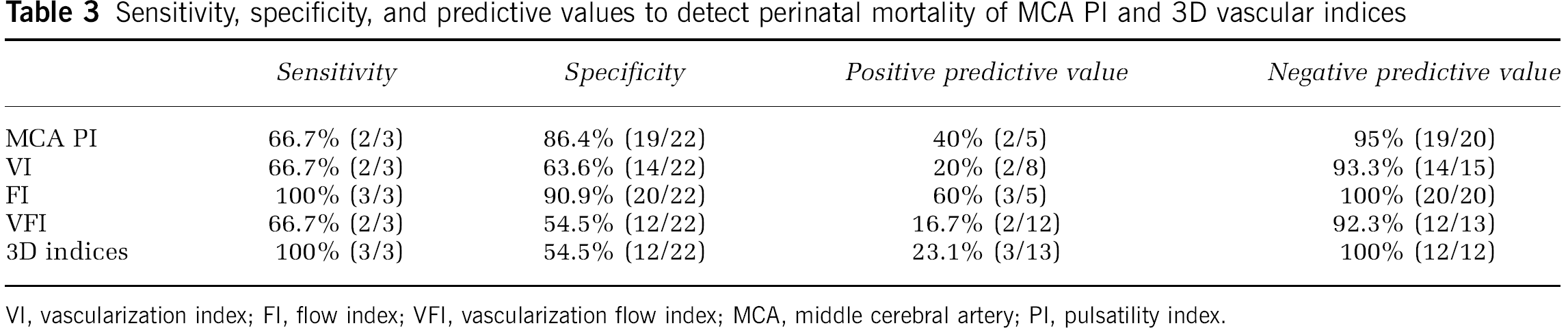
VI, vascularization index; FI, flow index; VFI, vascularization flow index; MCA, middle cerebral artery; PI, pulsatility index.
Discussion
Three-dimensional power Doppler fetal cerebral indices could be easily measured showing a high level of intra- and interobserver repeatability. This finding has been previously reported by studies focusing on different tissues (Pairleitner et al, 1999; Rovas
Chang et al (2003c) reported quantitative 3D power Doppler histogram analysis of cerebral blood flow in normal pregnancy. In their approach they did not use the sphere method of the VOCAL technique, but a manual method. In our opinion the use of an automated routine diminished the chance of errors and probably the inter- and intraobserver variability. In addition, we carefully defined the ultrasound axis to make the measurements to better standardize the technique. In addition, we also reported normal ranges in percentiles for each index and we also evaluated the relationships between normal 2D cerebral Doppler values and the new 3D vascular indices. Previous studies have reported that cerebral vascular density increases with gestation. Ballabh et al (2004) using immunohistochemical staining using antilaminin primary antibody found that vessel density and the percentage of blood vessel area increased as a function of gestational age in the gray matter and white matter (
We found increasing fetal brain blood flow, represented by both FI and VFI with gestation but, in contrast to the previous report (Chang et al, 2003c), we found that VI, representing the ‘number of brain vessels’ detected by 3D power values, remains unchanged during pregnancy except in cases of FGR.
Another study measuring a different index, the mean image pixel signal intensity, showed an increasing signal with gestational age (Dubiel et al, 2005). In our study, fetal cerebral FI correlated with both MCA PSV and PI, which also changed with gestation suggesting increasing cerebral blood flow as well. In spite of the 3D power Doppler indices correlated with each other, VI did not correlate with gestational age whereas FI clearly did it. The power of this co-correlation among the three indices was not strong enough to make significant the correlation between VI and gestational age. Vascularization flow index is a combination of FI and VI. For this variable, it is likely that its significant correlation with gestational age could depend on its co-correlation with FI. Nevertheless because it is also a product of VI, and VI is not significantly correlated with gestational age, its correlation with gestational age was clearly less significant than that of FI. This difference between the FI and the VI in relation with gestational age should depend of the different meaning that both indices have. Flow index indicated the energy reflected from the blood corpuscles in the vessels in the explored volume, nearly the whole brain, being related with the intensity of the signal. However, further studies are needed to clarify the real ‘
To the best of our knowledge this is the first study evaluating this technique in fetuses with FGR and analyzing its potential usefulness to evaluate hemodynamic redistribution. Dubiel et al (2005) evaluated 3D power Doppler angiography by using a different technique and a different index (mean signal intensity) and suggested that hemodynamic redistribution appeared physiologically at the end of pregnancy. This finding was not compared with the results obtained with the use of the conventional 2D Doppler indices. It is known that MCA PI and peak systolic velocity decreases and increases, respectively, with gestation suggesting this phenomenon. In spite they studied a group of high-risk pregnancies, no specific group of fetuses with FGR and/or placental insufficiency was studied. Again, the use of the sphere standardized technique and several 3D indices may be the best method to evaluate and analyze the results of the 3D power Doppler studies.
We found that, on average, the three 3D power Doppler indices were increased in FGR suggesting increased cerebral blood flow in cases of FGR. The finding of a high value of VI could be interpreted as the result of a greater number of cerebral vessels detected in fetuses with this condition. In hypoxic conditions, cells downregulate their overall metabolism and increase the production and secretion of factors involved in vessel formation, such as vascular endothelial growth factor (Martin et al, 1998). Thus angiogenesis leads to an increased capillary density, which is a mechanism to maintain the oxygenation of tissues by increased tissue perfusion (LaManna et al, 1992). The relation between hypoxia, a hypoxia inducible factor, and angiogenesis has been shown in fetal sheep, rats, and mice (LaManna et al, 1992; Harik et al, 1996; Martin et al, 1998; Chávez et al, 2000). Increased capillary densities decrease the overall vascular resistance of the organ considered. All these changes could be on the bases of the changes we have found in FGR.
The proposed pathophysiology of severe FGR is that placental insufficiency leading to fetal hypoxemia (Romero et al, 2002) triggers compensatory hemodynamic changes called hemodynamic redistribution. Even though this phase can be recognized clinically by several findings including decreased PI in the MCA and decreased amniotic fluid volume, the use of 3D power Doppler has some potential advantages. Using 3D power Doppler cerebral circulation is not represented by one single artery that may reproduce what it is happening in one particular brain area but not in the whole brain. The technique, as described in the present paper, is easy to perform for any operator with minimal training, in contrast to measurements on the MCA, which requires much a skillful operator to get reliable results. Finally, and more importantly 3D power Doppler indices seem to be more sensitive than MCA measurements to detect cases with abnormal cerebral circulation suggesting hemodynamic redistribution. In cases of FGR with placental insufficiency, at diagnosis, the proportion of fetuses with hemodynamic redistribution is about 20% to 25% although this proportion increases rapidly in the coming weeks of follow-up (Baschat et al, 2001). We found a 20% of fetuses in this situation. However, the 3D power Doppler indices, especially the VFI index, showed a much higher proportion of cases with hemodynamic redistribution than that detected by MCA measurements (up to a 52%). So, probably there are much more cases of fetuses having hemodynamic redistribution than those detected when using MCA pulsed Doppler. Brain perfusion in growth-restricted fetuses shows clear regional variations, which change with progression of hemodynamic deterioration. It has been reported that after an initial and early increase in the frontal area, progression of fetal deterioration is rapidly associated with a pronounced decrease in frontal perfusion, together with an increase toward the basal ganglia. On average, fetuses with FGR and placental insufficiency and normal MCA PI values can show considerable increments in fractional moving blood volume in the frontal, complete mid sagittal and cerebellar regions, and a mild increase in the basal ganglia (Hernandez-Andrade et al, 2008). Although cerebral circulation can be measured regionally by using 2D power Doppler multiple measurements, this is time-consuming, technically difficult, and reproducibility is poor. From the clinical point of view, this method would complicate excessively the evaluation process of the patient with FGR to study cerebral circulation. The advantage of the 3D technique is the possibility to have several indices representing the whole cerebral circulation with just one single measurement.
Oligohydramnios is a frequent finding in cases of FGR. Several studies have shown a significant reduction of urinary output in fetuses with FGR (Wladimiroff and Campbell, 1974; Kurjak et al, 1981; Nicolaides et al, 1990) and the degree of the reduction is well correlated with the degree of fetal hypoxemia as reflected by fetal blood
We used the ‘gold standard’ definition of hemodynamic redistribution for the majority of units of Fetal Medicine, which is based only on the presence of low values of MCA PI. It is not common in current obstetric practice to measure visceral blood flow for defining this situation. Several papers were published in the past using specific measurements of visceral blood flow (more frequently from renal artery, but also others such as descendent aorta and splenic artery), but the conclusions were that these measurements complicated the scanning examination with no benefits for clinical practice as decreased visceral flow was nearly always present when increased cerebral blood flow was present (Arbeille et al, 1994; Stigter et al, 2001). In addition all these measurements were technically more difficult and less reliable.
Previous reports (Weiner et al, 1994; Mari and Deter, 1992; Dubiel et al, 2002) have documented that MCA blood velocity may return to normal values in the terminal stage even in the presence of severely increased resistance to blood flow in the fetoplacental circulation. It has been said that this normalization of the brain-sparing effect in the terminal cases may also reduce the clinical usefulness of the conventional 2D method. The decrease of the MCA PI is progressive in the first stage of the disease and reaches a nadir at least 2 weeks before the onset of abnormal fetal heart rate patterns. A few hours before fetal death, there is a loss of cerebral vasodilatation, despite the persistence of high resistances in peripheral vessels (Man and Wasserstrum, 1991; Rizzo et al, 1994). These terminal changes are consistent with data obtained in animal models (Richardson et al, 1989). With progressive deterioration of fetal conditions, this protective mechanism is overwhelmed by the fall of cardiac output. Concomitantly the peak velocity during atrial contraction in the ductus venosus decreases and pulsations in the umbilical vein occur (Rizzo and Arduini, 1991; Rizzo et al, 1994; Arduini et al, 1993; Baschat et al, 2001), reflecting the fall of cardiac output. As a result, the terminal cases that show normal MCA cases are nearly always characterized by systemic cardiovascular failure having abnormal systemic central venous Doppler measurements, specifically in the ductus venous and also abnormal fetal heart rate patterns. This situation usually happens at the end stage of the evolution of fetuses with intrauterine growth restriction (Baschat et al, 2001). There could be also a regional variation in the hemodynamic redistribution phenomenon in the final stages of this condition. It has been suggested that the sparing of the frontal lobes is prolonged compared with the temporal and posterior parts of the brain as measurements of the anterior cerebral artery showed abnormal measurements whereas MCA Doppler indices were normal in these terminal cases (Dubiel et al, 2002). In our study there was only one case of perinatal mortality showing normal MCA Doppler measurements. In this particular case, the 3D indices were abnormal suggesting that hemodynamic redistribution persisted in some parts of the brain others than the region perfused by the MCA and this was detected by the 3D method. Nevertheless, only one case in this situation is not enough to reach conclusions on this particular issue. In any case, what this new technique introduces is a new method to easily detect hemodynamic redistribution at cerebral level, even in cases that the conventional Doppler measurements failed to identify, but it has limitations to detect fetuses at high risk of an adverse perinatal outcome in cases with absence of this phenomenon.
Moreover, the study of cerebral circulation in FGR and placental insufficiency is just one part of the evaluation of these fetuses. The absence of cerebral vasodilatation should be interpreted in the context of the rest of the data obtained from the clinical assessment and the rest of the Doppler study.
There are some potential criticisms to our study and about the use of 3D power Doppler technique. The first is obviously the cost of the equipment. This should be balanced in each institution against the potential benefits of the application of this technique in this or other health areas. Our method can also be criticized for using the automated volume acquisition provided by the equipment's software. In fact, the use of a sphere does not represent accurately total brain volume. We assumed we left a part of the cerebral circulation out of our measurements (mainly venous circulation in the posterior fossa). We did this way to set a rapid and easy method to make the measurements to be really useful in clinical practice. However, if needed, the VOCAL facility allows the use of manual mode by the operator, so a complete brain volume can be drawn and analyzed.
There are also some other limitations of the present study. Although the number of cases was good enough to show statistically significant differences between the normal and the FGR groups, further studies using a greater number of cases are needed to reach definitive conclusions about the clinical usefulness of this new method. Particularly in terms of prediction of perinatal mortality, with only three cases of death in the present study, conclusions should be interpreted carefully before leading to clinical consequences in clinical practice. Also, further studies are needed to clarify the evolution of the 3D indices as the fetal condition worsens.
The results of the present study suggest that 3D vascular indices can detect more cases of hemodynamic redistribution by showing the brain-sparing phenomenon. This has been described to precede fetal deterioration. The present study provides evidence that this is an adaptive process that may already exist in conditions of suboptimal fetal growth and normal MCA measurements. So, this new technique provides an alternative method that may alert about deterioration in fetal condition earlier than the conventional the MCA PI method. This finding may change the clinical management in these pregnancies.
Although having limitations, a new technique to evaluate the mechanisms involved in the response of fetal brain to acute and chronic hypoxia and hypotension is clearly worthy of further investigation, as it may provide clues to improved clinical strategies for management of cerebrovascular risk in the small-for-gestational-age infant. In this sense, Doppler methods, near-infrared spectroscopy, and functional magnetic resonance imaging bring new opportunities to better understand these mechanisms. Although the latter two are promising tools but until now less practical for routine use, Doppler measurements may offer opportunities to measure more easily cerebral circulation. The 3D technique may offer a new perspective for this method.
In conclusion, fetal cerebral 3D power Doppler indices can be easily and reliably used during pregnancy and may be more sensitive than MCA measurements to detect fetuses at risk of hypoxia and, therefore brain injury, but further studies are needed to set up the clinical value of this new technology.
Footnotes
There is not conflict of interest in any sense regarding this study.