
Abstract
We analyzed cortical microvascular parameters using intraoperative ICG (Indocyaninegreen)-Videoangiography in 13 patients with Moyamoya disease, and carried out correlative studies by comparing them with clinical parameters obtained by digital subtraction angiography, physical examination, and regional cerebral blood flow studies. Patients with reduced cerebrovascular reserve capacity were characterized by increased microvascular surface area (MVSA). In addition, MVSA correlated positively with arterial microvascular transit time. Asymptomatic patients were characterized by increased arterial microvascular transit time. We show that patients with a higher arteriogenic potential to alter cortical microvasculature are characterized by a more favorable hemodynamic situation and reduced clinical symptoms.
Keywords
Introduction
Moyamoya disease (MMD) represents a rare cerebrovascular disease characterized by progressive steno-occlusive lesions of the basal cerebral arteries leading to severe hemodynamic impairment paralleled by the development of collateral vessels (‘Moyamoya vessels’) at the base of the brain (Handa and Handa, 1972). Cortical vasculature has an important role in regulating cerebral hemodynamics and cerebral blood flow (Baumbach and Heistad, 1985). With the introduction of intraoperative Indocyaninegreen (ICG)-Videoangiography visualization and investigation of cortical vasculature has become possible and using this technique the anatomic parameter, microvascular surface area (MVSA), and the hemodynamic parameter, arterial microvascular transit time (AMVTT), have been introduced (Czabanka et al, 2008). Significantly increased MVSA accompanied by increased AMVTT have been shown to potentially represent a MMD-specific, arteriogenic compensation mechanism for hemodynamic impairment (Czabanka et al, 2008). However, the clinical significance of this observation remains unknown. It was the aim of our study to investigate the clinical implications of microvascular parameters (MVSA, AMVTT, microvascular density (MD), and diameter) in patients with MMD.
Materials and methods
Patient Population
A number of 13 patients (9 women and 4 men; average age 42 ± 10 years) experiencing MMD were included in our study. Moyamoya disease was diagnosed according to diagnostic criteria using digital subtraction angiography (Suzuki and Takaku, 1969). All patients received combined cerebral revascularization using standard extraintracranial arterial bypass surgery (direct superficial temporal artery-middle cerebral artery anastomosis) in combination with encephalomyosynangiosis.
Preoperatively, MMD patients underwent conventional catheter digital subtraction angiography. Angiographic stages of MMD were diagnosed and classified according to Suzuki and Takaku (1969). Functional rCBF (regional cerebral blood flow) studies consisted of the measurement of rCBF under rest and after the application of acetazolamide (15 mg/kg per body weight) using stable Xenon-computerized tomography technology (DDP Inc., Houston, TX, USA). Cerebrovascular reserve capacity (CVRC) was calculated as described elsewhere in detail (Horn et al, 2001). To obtain cerebral blood flow values for the region analyzed using ICG-Videoangiography, regions of interest (ROIs) of Xenon-CT were located in the medial cerebral artery territory.
Indocyaninegreen-Videoangiography
Indocyaninegreen-Videoangiography (Indocynine Green: Pulsion Medical Systems AG, Munich, Germany) was performed according to surgical implications. Placement of a millimeter scale grid on the cerebral surface guaranteed dimensional accuracy during postoperative analysis. During application of the fluorescent marker, blood pressure monitoring was recorded to exclude hemodynamic alterations that potentially interfered with cerebral perfusion during ICG injection.
Analysis of Cortical Microvascularization
For the analysis of cortical vascularization, we categorized cortical microvascularization according to functional ICG-angiographic aspects as previously described (Czabanka et al, 2008). In short, the early filling arteries (A1) and their direct branches (A2), and the last draining veins (V1) and their direct branches (V2) were referred to as cortical macrovasculature. All vessels appearing between A2 and V2 vessels were regarded as cortical microvasculature.
Microvascular parameters were quantified postoperatively using a computer-assisted analysis system (Caplmage, Zeintl Software Engineering, Heidelberg, Germany). For quantification of cortical microvasculature, we analyzed three suitable ROIs per cerebral hemisphere. Regions of interest, which were marked digitally using the analysis software, were characterized as an area of 25 to 100 mm2 surface without A1, A2, V1, and V2 vessels within this area. Quantification of MD was performed by calculating the length of all microvessels per analyzed ROI (Vajkoczy et al, 1998). For this purpose, microvessels were marked using the analysis system Caplmage, and the length of all marked microvessels was evaluated digitally and related to the area of the analyzed ROI. This relation was defined as MD. Furthermore, microvascular diameter (D) was analyzed by marking the diameter of the microvessel, which was automatically quantified using the image analysis software. Accordingly, MVSA per analyzed ROI was calculated on the basis of the following formula: MVSA = π × D/2 × MD (Czabanka et al, 2008).
Microhemodynamic analysis was performed postoperatively as previously described using IC-CALC 1.1 software (Pulsion Medical Systems AG, Munich, Germany) (Czabanka et al, 2008). IC-CALC 1.1 allows the analysis of fluorescence intensity in different compartments during ICG-Videoangiography. By comparing fluorescence intensity in the arterial (A2 vessel) and capillary compartments, the time difference between both fluorescent peaks can be calculated, which is defined as the time that the fluorescent dye requires to pass the cortical microvasculature in the arterial compartment (AMVTT) (Czabanka et al, 2008).
Statistical Analysis
For correlation testing, Pearson's correlation and Spearman's rank correlation testing were applied. Student's t-test was used to compare MVSA, AMVTT, and CVRC in symptomatic and asymptomatic patients. Differences were considered statistically significant for P < 0.05. All values are given as mean ± s.d.
Results
Patient Population and Clinical Parameters
The mean age of the Moyamoya patient population was 42 ± 10 years. Analysis of rCBF studies using predefined ROIs that correlated with the region analyzed by ICG-Videoangiography showed the following results: the mean basal CBF was 52 ± 17 mL/100g per min and the mean stimulated CBF was 55 ± 20 mL/100g per min. Calculated CVRC was 4 ± 25%. The mean systolic blood pressure measured during the application of ICG-Videoangiography in MMD patients was 134 ± 16 mmHg, and the mean diastolic blood pressure was 69 ± 10 mm Hg. A detailed description of patient population is summarized in Table 1.
Summary of patient population included in our study
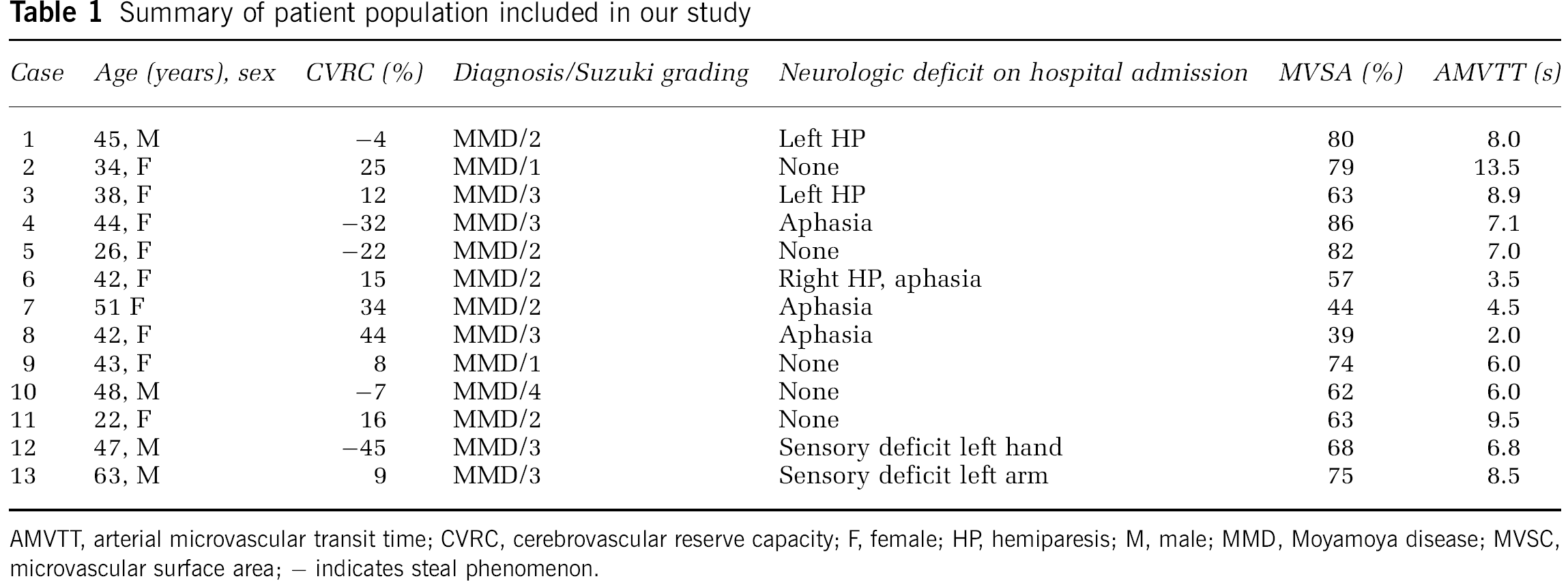
AMVTT, arterial microvascular transit time; CVRC, cerebrovascular reserve capacity; F, female; HP, hemiparesis; M, male; MMD, Moyamoya disease; MVSC, microvascular surface area; – indicates steal phenomenon.
All patients showed a history of recurrent transient ischemic attacks, and 8 of 13 patients presented with a manifest neurologic deficit specific for the analyzed hemisphere on admission to the hospital. For our analysis, we defined the symptomatic patient as a patient presenting with a manifest neurologic deficit (e.g., motor deficit, sensory deficit, aphasia) on hospital admission. The asymptomatic patient was defined as a patient presenting without a manifest neurologic deficit on hospital admission. The history of the patient was not included in our definition, as we wanted to focus on the effect of cortical microvasculature on the current neurologic situation, thereby excluding other factors, such as physical exercise or blood pressure dysregulation, which may lead to transient ischemic attacks in MMD patients.
Cortical Microvasculature
Anatomic analysis of ICG-Videoangiography showed MVSA to be 67 ± 14% (Table 1). Microhemodynamic analysis confirmed an AMVTT of 7 ± 2 secs in our patient population (Table 1). Correlative analysis showed a negative correlation between MVSA and CVRC (r = −0.636; Figure 1A). In comparison with angiographic stages, there was no significant correlation (Figure 1B).
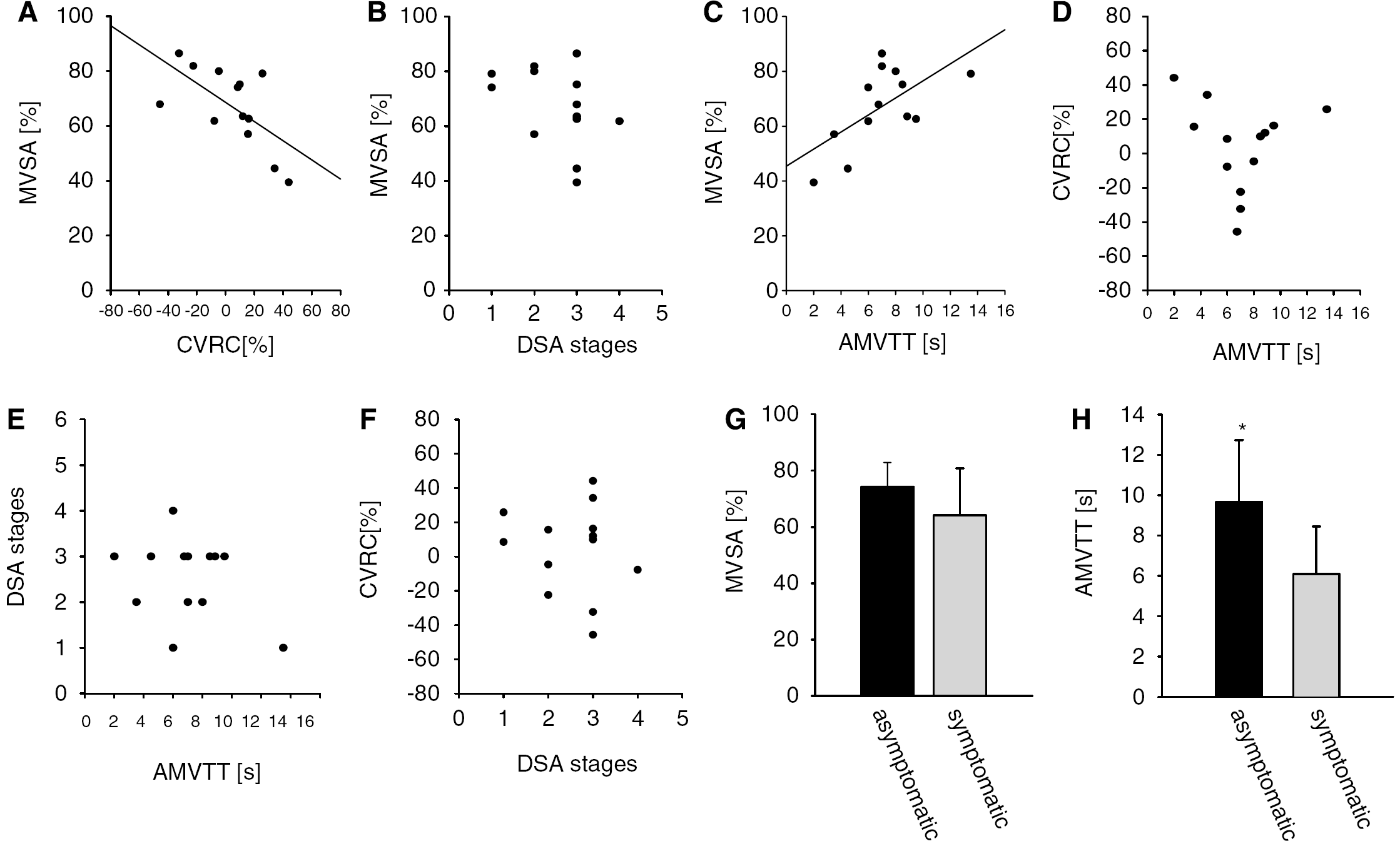
Graphical illustrations of correlative studies. (
Arterial microvascular transit time showed a positive correlation with MVSA (r = 0.630; P=0.021, Figure 1C) without a significant correlation between CVRC (Figure 1D) and angiographic stages (Figure 1E). Interestingly, CVRC did not show a correlation with angiographic stages (Figure 1F).
Patients with manifest neurologic deficits on hospital admission did not show any significant differences of CVRC in the analyzed cortical area (asymptomatic patients: 7 ± 20% versus symptomatic patients: 3 ± 29%). Asymptomatic patients showed a trend toward increased MVSA (asymptomatic patients: 74 ± 8% versus symptomatic patients: 63 ± 15%, P < 0.260, Figure 1G) and they were characterized by significantly prolonged AMVTT (asymptomatic: 10 ± 3 secs versus symptomatic: 6 ± 2 secs; P < 0.05, Figure 1H). Microvascular density also showed a trend toward an increase in asymptomatic patients compared with that in symptomatic patients (asymptomatic: 19 ± 0.8 cm/cm2 versus symptomatic: 17 ± 2 cm/cm2), whereas microvascular diameter was unaltered in both subpopulations (asymptomatic patients: 0.24 ± 0.01 mm versus symptomatic patients: 0.23 ± 0.03 cm/cm2).
Discussion
In our study, we show increased MVSA to be positively correlated with increased AMVTT in MMD patients. In addition, we show a negative correlation between MVSA and cerebrovascular reactivity. Patients who were asymptomatic on admission to the hospital showed a significantly prolonged microvascular transit time in the arterial compartment.
In contrast to patients experiencing chronic hemodynamic impairment due to atherosclerosis, MMD patients develop specific, arteriogenic compensatory mechanisms like the typical Moyamoya vessels at the base of the brain and extensive extraintracranial collaterals (Natori et al, 1997). Increased cortical microvasculature paralleled by prolonged cortical microhemodynamics has been proposed to be a potential novel arteriogenic compensatory mechanism in MMD by reducing peripheral vascular resistance (Czabanka et al, 2008).
We show that MVSA correlates negatively with CVRC. As MVSA represents a compensation mechanism for reduced cerebral blood flow, we argue that patients with a strongly reduced CVRC, and consequently a severe form of chronic ischemia depend on a higher MVSA to compensate for their blood flow deficit compared with patients with less reduced CVRC. This could explain the negative correlation between MVSA and CVRC.
In addition, we found a significant correlation between AMVTT and MVSA. Arterial microvascular transit time represents the time that the fluorescent dye Indocyaninegreen requires to pass arterial microvascularization and therefore, represents an indirect parameter reflecting cortical microhemodynamics in the arterial microvascular compartment (Czabanka et al, 2008). Arterial microvasculature has an important role in regulating cerebral perfusion as more than half of the total cerebrovascular resistance is located in the extraparenchymal vessel segments (Baumbach and Heistad, 1985). An increase in the number or in the diameter of arteriolar resistance vessels leads to an increase in microvascular cross-sectional area, and thus to decreased peripheral microvascular resistance. The observation of increased AMVTT in combination with increased MVSA suggests decreased peripheral microvascular resistance as a potential compensation mechanism for chronic hemodynamic impairment. In this regard Okada et al (1988) were able to show diminished vascular resistance between cortical arteries of the middle cerebral artery territory and the corresponding veins in MMD patients.
Arterial microvascular transit time has not been shown to correlate with CVRC in our study. To draw conclusions about cortical blood flow and its relation to cerebrovascular reactivity from transit time measurements, a stable microangioarchitecture is required. As we have shown previously, MD and cortical microvasculature are increased significantly and the microangioarchitecture is severely altered in MMD (Czabanka et al, 2008). Therefore, conclusions about the functional aspects of cerebral blood flow and cerebrovascular reactivity cannot be drawn definitely from transit time measurements. Furthermore, we have to point out that cerebral infarctions may alter cerebral blood flow. In our study, 10 of 13 patients showed border-zone infarctions in MRI, but none showed a territorial infarction. Therefore, we argue that infarction-induced alterations of cerebral blood flow did only have a minor role in our study.
When comparing MVSA and AMVTT with angiographic stages according to Suzuki, we found no correlation between those parameters. This is not a surprising finding as the angiographic classification of MMD according to Suzuki is primarily orientated on the extent of the basal steno-occlusive lesions. Hemodynamic or microvascular considerations are not a part of the Suzuki classification (Suzuki and Takaku, 1969). In this regard, Ogawa et al (1987, 1990) showed already in 1990 that the adult MMD population does not show a decline in cerebral blood flow according to the angiographic stages in contrast to the juvenile patient population.
When analyzing microvascular parameters in MMD patients with a manifest neurologic deficit on hospital admission in comparison with MMD patients without a manifest deficit, we found that patients presenting without a neurologic deficit were characterized by increased MVSA and significantly increased AMVTT. The increase in MVSA was most probably because of an increase in MD, although microvascular diameter was found to be unaltered between asymptomatic and symptomatic patients.
Therefore, we show that asymptomatic patients with an increased arteriogenic potential leading to increased MVSA are characterized by a more favorable hemodynamic situation in the arterial microvascular compartment, which underlines the potential clinical importance of cortical microvasculature as a MMD-specific compensatory mechanism.
Footnotes
The authors declare no conflict of interest.