
Abstract
Most clinical trials have focused on the presence of perfusion- and diffusion-weighted imaging (PWI–DWI) mismatch by more than 20%, and different stroke subtypes were lumped together. We hypothesized that intracranial large artery atherosclerotic stroke (IC-LAA) would show different PWI–DWI and magnetic resonance angiography (MRA)–DWI mismatch profiles, compared with other stroke subtypes. Consecutive patients underwent pretreatment multiparametric magnetic resonance imaging for the acute middle cerebral artery infarcts within 6 h of symptom onset. We assessed the difference in the DWI–PWI mismatch ratio, severity of hypoperfusion, and MRA–DWI mismatch among the stroke subtypes. Of 86 patients, 19 (22.1%) had IC-LAA; 42 (48.8%) cardioembolic stroke, 15 (17.4%) extracranial-LAA, and 10 (11.6%) had cryptogenic embolic stroke. Although the volume of the penumbra was not different among the groups, the mismatch ratio was higher (P=0.003) and the severity of hypoperfusion was lower in the IC-LAA group (P=0.001). The MRA–DWI mismatch was more prevalent in the IC-LAA group than in other groups (
Introduction
Multiparametric magnetic resonance imaging (MRI), including diffusion-weighted imaging (DWI) and perfusion-weighted imaging (PWI), has increasingly been used in clinical practice for selecting patients for recanalization therapy after stroke (Albers et al, 2006; Furlan et al, 2006; Hacke et al, 2005; Hjort et al, 2005; Kohrmann et al, 2006). Hyperintense DWI lesions can appear within 30 to 60 mins from the onset of infarction, whereas PWI defines an area of hypoperfusion. Thus, the mismatch between areas of hypoperfusion and areas of decreased diffusion on MRI have been suggested to be a penumbra zone, although many uncertainties remain (Kidwell et al, 2003).
Most clinical trials have focused on the presence of PWI—DWI mismatch by more than 20%. However, the severity of hypoperfusion and vascular status and the extent of hypoperfusion determine tissue fate. Recently, Lansberg and colleagues of the Diffusion and Perfusion Imaging Evaluation for Understanding Stroke Evolution (DEFUSE) trial group reported that the magnetic resonance angiography (MRA)–DWI mismatch model could identify patients with stroke who are likely to benefit from reperfusion therapy (Lansberg et al, 2008). In addition, few studies have looked at differences in the hypoperfusion pattern among stroke subtypes; patients with different stroke subtypes were lumped together as one group. Most recent studies on hypoperfusion have been performed in Western countries, where the prevalence of intracranial large artery atherosclerotic stroke (IC-LAA) is much lower than in Asian countries; thus, relatively little attention has been devoted to this type of stroke mechanism. Intracranial large artery atherosclerotic stroke accounts for one-quarter to one-third of all strokes in Asian patients (Kieffer et al, 1967; Liu et al, 1996; Wong et al, 1998). Although the stroke classifications used widely in clinical trials (Adams et al, 1993; Ay et al, 2005) classify IC-LAA and extracranial large artery atherosclerotic stroke (EC-LAA) together, there are accumulating evidences that these two types of stroke differ in terms of ethnicity, risk factors, natural history, mechanism, and long-term recurrence (Inzitari et al, 1990; Shin et al, 2005; Uehara et al, 2005; Kang et al, 2003; Wong et al, 2002).
Our hypothesis was that IC-LAA would show different PWI–DWI and MRA–DWI mismatch profiles, compared with the other stroke subtypes.
Materials and methods
Patient Selection
Our analysis was performed on data collected in a prospective registry of patients who were eligible for recanalization therapy for acute infarct of the middle cerebral artery (MCA), and who were evaluated with diffusion-perfusion MRI. This study analyzed consecutive patients encountered at a University Medical Center from June 2005 to July 2008. Inclusion criteria for this study were: (1) presentation within 6 h of symptom onset; (2) performance of pretreatment MRI, including DWI, PWI, and MRA; (3) acute ischemic lesions within the MCA distribution on DWI or perfusion defects within the MCA territory on PWI; and (d) a NIHSS (National Institute of Health Stroke Scale) score of ≥ 4 points at the time of pretreatment MRI.
In this study, we included atherosclerotic, cardioembolic (CE), and cryptogenic embolic stroke. Patients with small arterial occlusive stroke (
Patients Grouping
Stroke subtypes were determined according to the SSSTOAST (Stop Stroke Study Trial of Org 10172 in Acute Stroke Treatment) classification (Ay et al, 2005), with the following modifications: patients with atherosclerotic stroke were divided into IC-LAA and EC-LAA. Intracranial large artery atherosclerotic stroke was diagnosed when the initial angiography showed symptomatic atherosclerotic intracranial arterial stenosis of ≥ 50% or occlusion, and when neither a cardiac nor an extracranial arterial embolic source could be identified. The large intracranial arterial system included the intracranial portion of the internal carotid artery (ICA) and the M1 portion of the MCA. If the M2 portion of the MCA showed stenosis or occlusion in isolation, the patient was included as IC-LAA with one of the three additional findings, namely concomitant stenotic lesions on the contralateral M1 portion of the MCA or the intracranial portion of the ICA, or the intracranial portion of the vertebral artery or the basilar artery. Extracranial large artery atherosclerotic stroke was diagnosed if there was symptomatic extracranial arterial stenosis of ≥ 50% or occlusion without evidence of CE. Cryptogenic embolic stroke was diagnosed when there was an angiographic evidence of an abrupt cutoff, consistent with a blood clot, within otherwise angiographically normal-looking intracranial arteries, or imaging evidence of the complete recanalization of an earlier occluded artery, or the presence of multiple acute infarctions that had occurred closely in time, without a detectable abnormality in the relevant vessels. Stroke subtype and phenotype were diagnosed by consensus of two stroke neurologists (O.Y.B. and G.M.K.).
Magnetic Resonance Imaging Methods and Image Analysis
Magnetic resonance imaging was performed using a 3.0T unit (Achieva, Philips Medical Systems, Best, The Netherlands). The typical stroke MRI protocol consisted of DWI, PWI, T2 × gradient-echo imaging, gadolinium-enhanced T1-weighted imaging, and vascular images (three-dimensional time-of-flight MRA and contrast-enhanced MRA, including extracranial ICA and vertebral artery). The DWI parameters were as follows: TR (repetition time), 3,000 msecs; TE (echo time), 46 msecs; matrix, 128 × 128; 3 directions; FOV (field of view), 24 cm; section thickness, 5 mm; and intersection gap, 2 mm. Diffusion-weighted imaging was obtained with
Magnetic resonance imaging volume measurements were performed by one of authors (K.H.K.), blinded to the clinical information. For each patient, DWI and PWI lesion volumes were outlined automatically with subsequent manual corrections, and the volumes were calculated using a computer-assisted volumetric analysis program (Medical Image Processing, Analysis and Visualization, version 2.1, CIT, NIH). The mismatch ratio was defined as the ratio of PWI lesion volume of
The MRA rating and MRA–DWI mismatch was defined according to the prespecified MRA–DWI mismatch criteria (Lansberg et al, 2008). For the intracranial ICA and M1 segment of the MCA, 1= normal; 2 = reduced flow; and 3 = occlusion. For the M2 segment of the MCA, 1 = normal and 2 = abnormal. The MRA–DWI mismatch was defined as an MRA score of 3 and a DWI lesion volume < 25 mL or an MRA score of 2 and a DWI lesion volume < 15 mL. The MRA was rated independently by two stroke neurologists (S.J.K. and J.M.S.) who were only informed of the symptomatic hemisphere of the patient. The third opinion (by RJ.) was obtained in cases of disagreement.
Conventional Angiographic Study
Some of the patients underwent comprehensive cerebral angiography, including injection of both ICAs and the dominant vertebral artery, with assessment through the late venous phase. The angiographic collateral grade was evaluated using the ASITN/SIR Collateral Flow Grading System on pretreatment angiography (Higashida et al, 2003). This angiographic scale assigns patients to grade 0 (no visible collateral to the ischemic site), grade 1 (slow collaterals to the periphery of the ischemic site with persistence of some of the defect), grade 2 (rapid collaterals to the periphery of ischemic site with persistence of some of the defect and to only a portion of the ischemic territory), grade 3 (collaterals with slow but complete angiographic blood flow of the ischemic bed by the late venous phase), and grade 4 (complete and rapid collateral blood flow to the vascular bed in the entire ischemic territory by retrograde perfusion). In this study, scores of 0 and 1 were designated as poor collateral flow; grades 2 and 3, as intermediate; and grade 4, as excellent. The collateral grade was rated independently by two stroke neurologists (S.J.K. and J.M.S.) who were only informed of the symptomatic hemisphere of the patient. The third opinion (RJ.) was obtained in cases of disagreement.
Statistical Analysis
The differences in the clinical, laboratory, and radiologic characteristics among stroke subtypes were evaluated using one-way ANOVA (analysis of variance) or Kruskall-Wallis test for continuous variables, Pearson's χ2 or Fisher's exact test for categorical variables. The independent
Results
Of the 98 patients who met the inclusion criteria during the study period, a total of 86 patients (50 men and 36 women; age, 66.4 ± 13.0 years) were included in this study. Twelve patients were excluded owing to the failure of post-MRI processing or selection of the wrong arterial input function. Pretreatment MRI and conventional cerebral angiography were performed at 3.2 ± 1.5 h (range, 0.9 to 7.4) and 5.6 ± 1.9h (range, 2.6 to 8.7), respectively.
Clinical and laboratory characteristics of patients, classified by stroke subtype, are presented in Table 1. Male gender and hypertension were more frequently observed in patients with EC-LAA, whereas atrial fibrillation was more prevalent in patients with CE. Hyperlipidemia was more frequent in patients with EC-LAA, but was not significantly so. The NIHSS score on admission was lower in patients with IC-LAA than in those with CE. Age, diabetes, smoking habits, coronary heart disease, stroke/transient ischemic attack (TIA) history, onset to pretreatment MRI time, and other laboratory findings did not differ among the groups.
Clinical and laboratory characteristics of patients according to the stroke subtypes
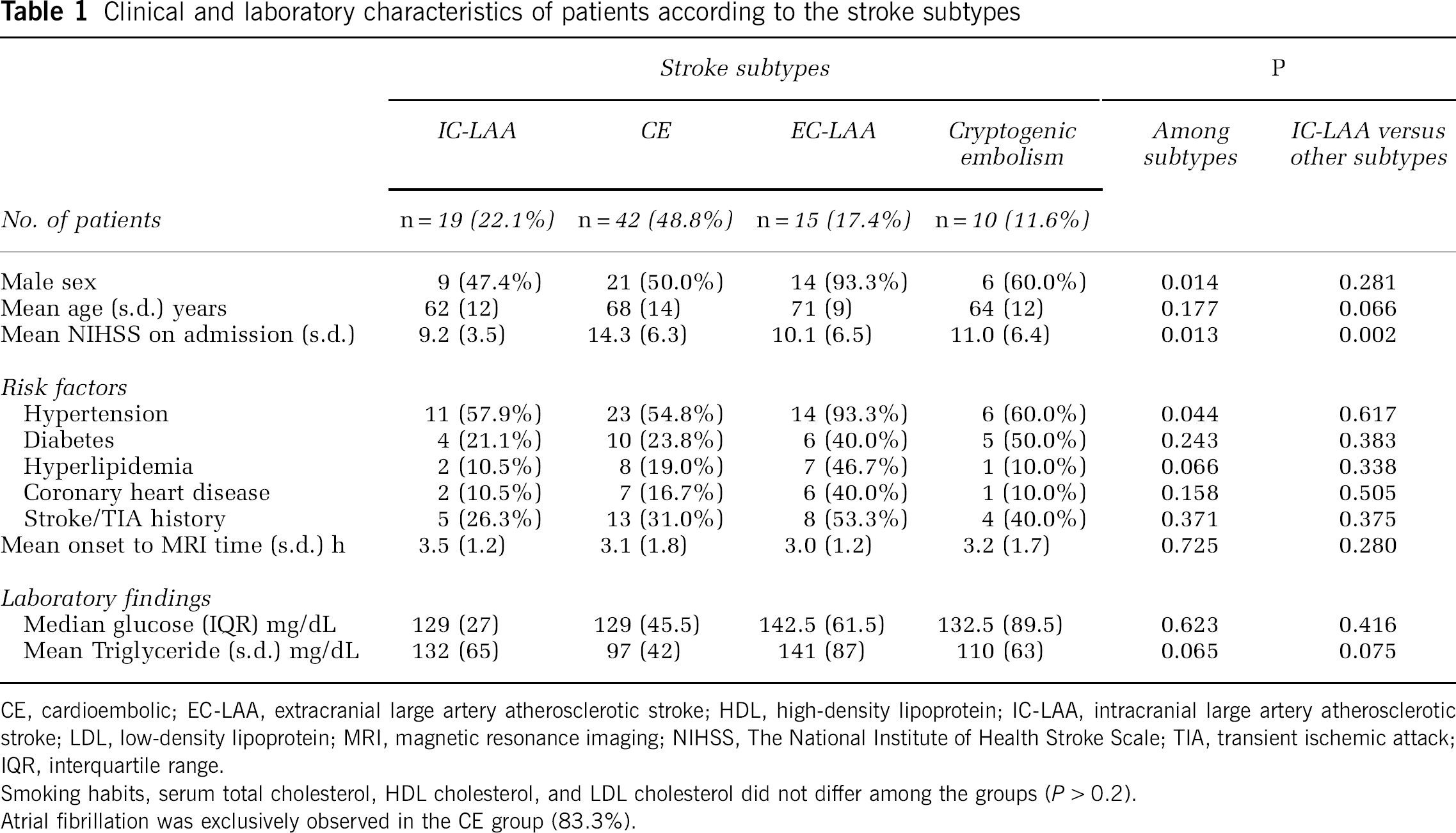
CE, cardioembolic; EC-LAA, extracranial large artery atherosclerotic stroke; HDL, high-density lipoprotein; IC-LAA, intracranial large artery atherosclerotic stroke; LDL, low-density lipoprotein; MRI, magnetic resonance imaging; NIHSS, The National Institute of Health Stroke Scale; TIA, transient ischemic attack; IQR, interquartile range.
Smoking habits, serum total cholesterol, HDL cholesterol, and LDL cholesterol did not differ among the groups (
Atrial fibrillation was exclusively observed in the CE group (83.3%).
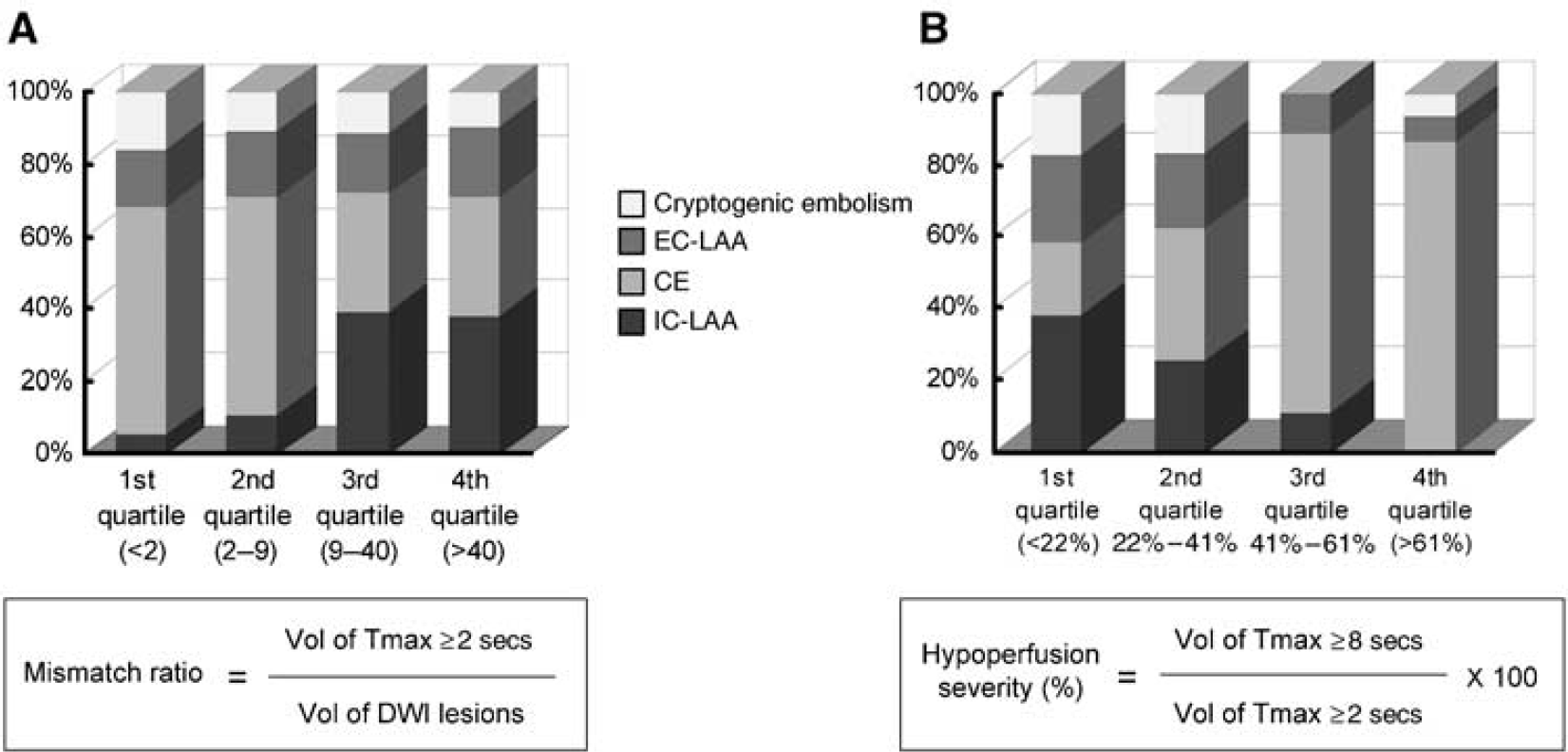
Radiologic characteristics of different stroke mechanisms are illustrated in Table 2. The volumes of initial penumbra were not different among the groups. However, the mismatch ratio and the severity of perfusion defect differed by stroke subtype (Figure 1). Compared with other stroke mechanisms, IC-LAA had a much higher mismatch ratio (
Radiologic characteristics of patients according to the stroke subtypes
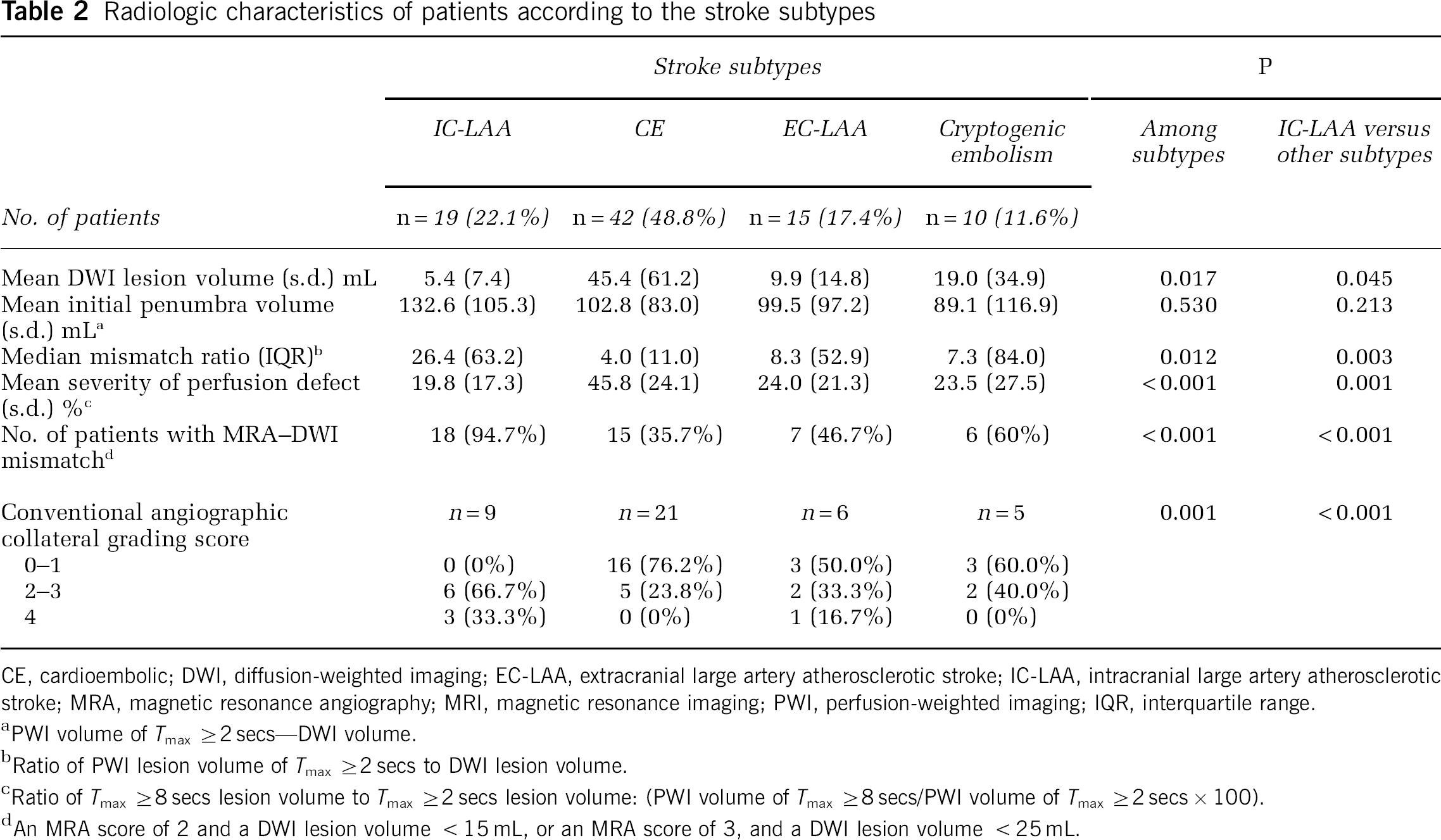
CE, cardioembolic; DWI, diffusion-weighted imaging; EC-LAA, extracranial large artery atherosclerotic stroke; IC-LAA, intracranial large artery atherosclerotic stroke; MRA, magnetic resonance angiography; MRI, magnetic resonance imaging; PWI, perfusion-weighted imaging; IQR, interquartile range.
PWI volume of
Ratio of PWI lesion volume of
Ratio of
An MRA score of 2 and a DWI lesion volume < 15 mL, or an MRA score of 3, and a DWI lesion volume < 25 mL.
(
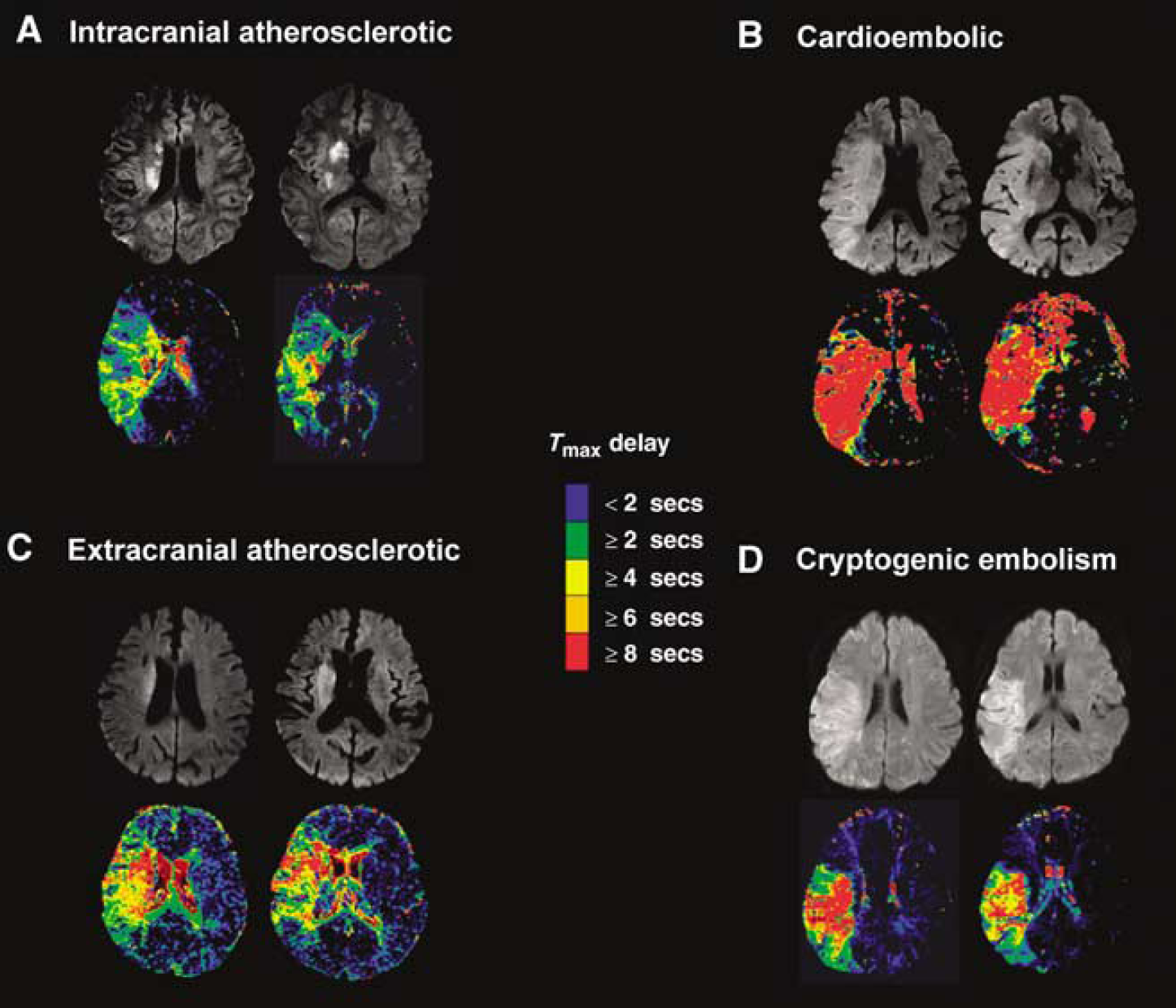
Typical examples of DWI and PWI in patients with different stroke mechanisms.
Of patients who showed total occlusion of symptomatic vessels on conventional angiography, we compared conventional angiographic collateral grading among different stroke mechanisms (
Clinical and radiologic features independently associated with IC-LAA were analyzed by multiple logistic regression (Table 3). After adjusting for covariates; model 1 (not including MRA–DWI mismatch as an explanatory variable) revealed an independent association with IC-LAA in the higher half of the mismatch ratio (OR (odds ratio), 4.84; 95% CI (95% confidence interval), 1.35 to 17.34) and lower half of the severity of perfusion defect (OR, 6.21; 95% CI, 1.14 to 33.74). On the contrary, in model 2 (including MRA–DWI mismatch as an explanatory variable) the MRA–DWI mismatch (OR, 15.81; 95% CI, 1.45 to 171.93) alone was independently associated with IC-LAA.
Logistic regression analysis: clinical and radiologic features associated with IC-LAA
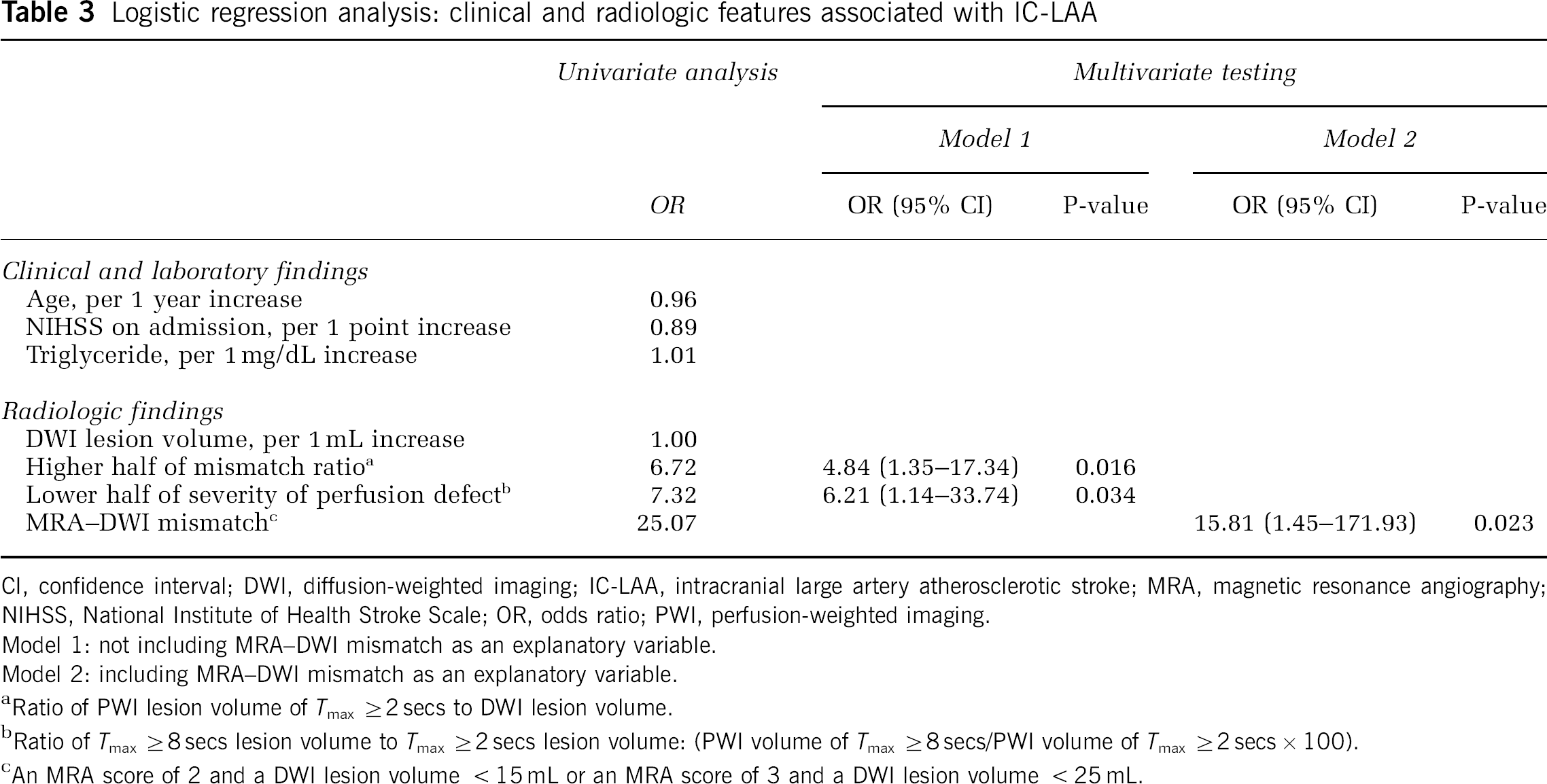
CI, confidence interval; DWI, diffusion-weighted imaging; IC-LAA, intracranial large artery atherosclerotic stroke; MRA, magnetic resonance angiography; NIHSS, National Institute of Health Stroke Scale; OR, odds ratio; PWI, perfusion-weighted imaging.
Model 1: not including MRA–DWI mismatch as an explanatory variable.
Model 2: including MRA–DWI mismatch as an explanatory variable.
Ratio of PWI lesion volume of
Ratio of
An MRA score of 2 and a DWI lesion volume < 15 mL or an MRA score of 3 and a DWI lesion volume < 25 mL.
Discussion
Intracranial large artery atherosclerotic stroke is one of the major causes of stroke in Asians and in blacks. In our study, the prevalence of patients with IC-LAA was 22.1% among Korean patients with acute ischemic stroke who were eligible for recanalization therapy. Many studies have evaluated predictors for favorable outcome after recanalization therapy for acute ischemic stroke. However, earlier studies have largely not addressed stroke mechanisms, especially IC-LAA (Albers et al, 2006; Clark et al, 1999; Davis et al, 2008; Furlan et al, 2006; Hacke et al, 1995, 1998, 2005; The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group, 1995). To our knowledge, this is the first study regarding the PWI–DWI and MRA–DWI mismatch profiles in patients with IC-LAA, compared with other stroke subtypes.
The major findings of our study were that patients with IC-LAA had PWI–DWI (larger mismatch ratio but less severe hypoperfusion) and MRA–DWI mismatch profiles, which have been reported to be associated with favorable outcomes after recanalization therapy (Albers et al, 2006; Furlan et al, 2006; Hacke et al, 2005; Hjort et al, 2005; Kohrmann et al, 2006; Lansberg et al, 2008; Bang et al, 2008). In this study, we have considered several different mismatch profiles simultaneously (using DWI, PWI, and MRA data) to characterize the penumbra zone, for the following reasons. First, the ideal PWI–DWI mismatch definition was not settled yet, and there have been growing evidences that a simple diffusion-perfusion mismatch model may not accurately identify the ischemic penumbra (Kidwell et al, 2003). Most clinical trials defined the diffusion-perfusion mismatch as PWI–DWI ratio 1.2 using
The results of our study suggest that patients with IC-LAA may show more favorable clinical outcomes after recanalization than those with other subtypes, especially CE. Further studies with data on infarct growth determined by serial MRI are needed to confirm our findings. In addition, in clinical trials of recanalization therapy for acute ischemic stroke, race and ethnicity should be considered in the analysis, because the prevalence of IC-LAA differs among Asians, blacks, and Caucasians.
The differences in PWI–DWI mismatch profiles and in MRA-DWI mismatch profile between IC-LAA and other subtypes may be related to differences in pretreatment collateral flow status; in this study, patients with IC-LAA had a good collateral grade than those with other subtypes. Collateral flow is an important indication for good treatment outcome after thrombolysis in acute stroke patients (Liebeskind, 2003). Using serial MRI data, we recently found that the pretreatment collateral grade was associated with infarct growth in patients undergoing endovascular recanalization therapy (Bang et al, 2008). The good collateral flows of IC-LAA may be explained by the speed of occlusion. In patients with CE and cryptogenic embolism, arterial occlusion occurs suddenly; hence, the time available for developing collaterals may be insufficient. Similar mechanisms may apply in EC-LAA, which are related to thromboembolism owing to plaque instability. Conversely, IC-LAA is associated with microembolism or hemodynamic instability (Wong et al, 2002). These mechanisms require a longer time for complete arterial occlusion, allowing the development of adequate collateral flow before the onset of stroke.
There are several limitations to our study. First, this was a single-center trial with a modest sample size. Multicenter trials with larger cohorts and different study populations are warranted. Second, in this study,
In conclusion, IC-LAA as stroke mechanism had a relatively larger salvageable area of less severe hypoperfusion and more frequent MRA–DWI mismatch profile. Good collateral flows of IC-LAA may explain these results. Larger, multicenter, confirmatory studies with long-term follow-up are needed to determine whether IC-LAA has different responses after recanalization therapy.
Footnotes
The authors declare no conflict of interest.