
Abstract
The aim of this study was to evaluate and compare the effects of anti-platelet agents with different modes of action (cilostazol, aspirin, and clopidogrel) on brain infarction produced by photothrombotic middle-cerebral-artery (MCA) occlusion in male, spontaneously hypertensive rats. Cerebral blood flow (CBF) was measured with laser-Doppler flowmetry in the penumbral cortex. Infarct size was evaluated 24 h after MCA occlusion. The effects of these drugs on infarct size were examined by pretreatment of rats undergoing MCA occlusion. Pretreatment with cilostazol (100 mg/kg) significantly reduced infarct size. In contrast, aspirin (10 mg/kg) and clopidogrel (3 mg/kg) failed to mitigate infarct size, regardless of their apparent inhibitory effects on platelet aggregation. Post-treatment with cilostazol also significantly attenuated the infarct size, associated with improved CBF in the penumbral region. In support of this effect, cilostazol increased nitric oxide (NO) production and prostaglandin-I2 (PGI2) release in cultured human brain microvascular endothelial cells. Cilostazol-induced NO production and PGI2 release were completely abolished by an NO synthase inhibitor and aspirin, respectively. These findings show that cilostazol reduced brain infarct size due to an improvement in penumbral CBF possibly in association with increased endothelial NO and PGI2 production.
Keywords
Introduction
Cilostazol, a selective inhibitor of phosphodiesterase-3, is an anti-platelet drug and a vasodilator (Kambayashi et al, 2003). It has been used for treatment of ischemic symptoms in patients with chronic peripheral arterial obstruction and for the secondary prevention of brain infarction (Kambayashi et al, 2003; Matsumoto, 2005). Aspirin (a cyclooxygenase inhibitor) and clopidogrel (a platelet P2Y12-receptor antagonist) are well known anti-platelet drugs and are used for patients with ischemic heart diseases and ischemic stroke worldwide (Billett, 2008; Papathanasiou et al, 2008). Recently, cilostazol has been shown to be a more effective and safer alternative to aspirin for long-term prevention of the recurrence of ischemic stroke in Chinese patients with chronic ischemic stroke (Huang et al, 2008). Furthermore, cilostazol attenuated acute brain infarction induced by middle-cerebral-artery (MCA) occlusion–reperfusion in rats (Choi et al, 2002; Lee et al, 2003), suggesting its potential to ameliorate acute ischemic stroke by minimizing evolving ischemic injury. However, the influence on the development and complications of mechanical occlusion of the MCA is different from that of cerebral ischemia induced by thrombotic occlusion as is seen with photochemically induced platelet thrombi (Watson et al, 1985, 1995). These thrombotic occlusions are more relevant to human stroke than are mechanical occlusions. Hence, the photothrombotic model is useful and reasonable to examine the effects of anti-platelet drugs on brain infarction in basic research.
In the present study, we compared the beneficial effects of three anti-platelet drugs with different modes of action (cilostazol, aspirin, and clopidogrel) on photothrombotically induced infarction in spontaneously hypertensive rats (SHRs). Another issue is whether post-ischemic treatment with cilostazol is effective in this model, since the therapeutic efficacy by post-ischemic treatment is a prerequisite for successful acute stroke treatment. Therefore, we further examined the therapeutic effects of cilostazol on acute ischemic stroke, with post-ischemic administration in rats with MCA occlusion. The effect of post-ischemic administration of cilostazol on cerebral blood flow (CBF) in acute brain ischemia is an intriguing aspect of research. Endothelial nitric oxide (NO) synthase (NOS) plays a role in improving CBF and preventing brain injury in the ischemic region (Samdani et al, 1997). Endogenous mediators such as NO and prostaglandin-I2 (PGI2) are protective against brain infarction by improving CBF (Faraci, 1992; Karasawa et al, 2003; Wainwright et al, 2007). These mediators are mainly produced by vascular endothelial cells. Thus, therapeutic agents that increase production of these vasodilating substances by endothelial cells presage their beneficial effects in cerebral infarction. Therefore, we investigated the effects of cilostazol on NO production and PGI2 release in
Materials and methods
Animals
Adult male SHRs (body weight 346 ± 33 g; over 20 weeks old; SHR/Hoshino, SLC, Japan) were used. All experimental procedures were performed in accordance with the Guidelines for Animal Care and Use of Otsuka Pharmaceutical Co. Ltd.
Ex Vivo Platelet Aggregation
Cilostazol (100 and 300 mg/kg), aspirin (1, 10, and 100 mg/kg), and clopidogrel (1, 3, and 10 mg/kg) were suspended in 2% arabic gum solution and orally administered to SHRs at 5 mL/kg. Arabic gum solution was used for the control group. Three hours after single administration of the drugs, citrated peripheral blood was collected from the vena cava under ether anesthesia. The final concentration of citrate was 0.313%. Platelet-rich plasma was obtained by centrifuging the blood at 200 ×
Effects of Anti-Platelet Drugs on Infarct Size
(1) In the pre-ischemic administration study, cilostazol (30 and 100 mg/kg) or vehicle was administered 2 h before MCA occlusion. In the post-ischemic administration study, cilostazol (30 and 100 mg/kg) or vehicle was administered 30 mins after MCA occlusion. In the pre-ischemic administration study, the time of administration was chosen because cilostazol shows maximal plasma levels at 2 to 4 h after oral administration in rats (data not shown). (2) For the comparative study of anti-platelet drugs, aspirin (10 mg/kg), clopidogrel (3 mg/kg), and 2% arabic gum were administered orally, approximately 2 h before MCA occlusion.
Photothrombotic MCA Occlusion
Male SHRs (20–24 weeks old) were anesthetized with halothane (3% for induction, 1.5%. during the surgical preparation, 0.75% after intubation, and 0.5% for maintenance) in a mixture of 70% nitrous oxide and 30% oxygen. The right femoral artery and vein were cannulated with PE50 tubing. The rats were endotracheally intubated with PE240 tubing and were mechanically ventilated at a volume of 2.5 mL/300g with a rodent ventilator (model 683; Harvard Apparatus, Holliston, MA, USA). Rats were then mounted on a stereotaxic head holder in the prone position, and a 3-cm incision was made vertically midway between the right orbit and the right external auditory canal. The temporalis muscle was separated, and a burr hole (3 mm in diameter) was made 1 mm rostral to the anterior junction of the zygoma and squamosal bone under an operating microscope, revealing the distal segment of the MCA. The burr hole was made using an electric drill (minimo; Minitor, Tokyo, Japan) with an electrodeposited diamond burr (1.8 mm in diameter). A thin bone layer was preserved to prevent injury to the brain and was carefully removed with pincers. The dura was, thereby, left intact.
Rectal and brain temperatures were monitored with a thermo probe and maintained at approximately 37.5°C and 36.5°C, respectively, using an incandescent lamp. Mean blood pressure and heart rate were measured using a polygraph (365; NEC San-ei, Tokyo, Japan) through the cannulated femoral artery. Approximately 300 μL of blood was collected from the femoral artery with a 1-mL syringe to determine blood O2, CO2 gas pressure, and pH with an auto pH/blood gas analyzer (248; Chiron, Tokyo, Japan). Blood glucose levels were measured with a blood glucose analyzer (antsense II; Bayer Medical, Tokyo, Japan). Pre-and post-values of these physiological parameters were measured 10–20 mins before and after MCA occlusion in the pre-administration studies, and, in addition, 1 h after drug administration in the cilostazol post-administration study.
A krypton laser (643-Y-A01; Melles Griot, Carlsbad, CA, USA) operating at 568 nm was used to irradiate the distal MCA at an intensity of 20 mW for 4mins. The corresponding energy at the focal plane was approximately 64 mW/mm2. An elliptical, almost-linear laser beam (linear hit, approximately 2 mm long) focused with a 30-cm focal length cylindrical lens (CKX 300; Newport Corporation, Irvine, CA, USA), was positioned with a mirror onto the distal MCA. The photosensitizing dye rose Bengal (15 mg/mL in 0.9% saline; Wako Pure Chemical Industries, Tokyo, Japan) was administered intravenously at 20 mg/kg over 90 secs starting simultaneously with 4 mins of laser irradiation.
Measurement of CBF
Cerebral blood flow was determined by laser-Doppler flowmetry in SHRs. We made one hole at the side of MCA occlusion and used a slide caliper (sr-5r; Narishige, Tokyo, Japan) that was fixed on the operating plate. CBF was measured at 1mm posterior and 1, 2, 3, and 4 mm lateral to the bregma by laser-Doppler flowmetry (alf 21n; Advance, Tokyo, Japan) following the procedure of Yao et al (2003). This multi-point measurement of CBF would reduce the risk of missing the zone of improved perfusion associated with the drug therapy. Changes in CBF were expressed as percentage change in value after MCA occlusion (% of pre-value). Pre- and post-values of CBF were measured 10mins before and after MCA occlusion, respectively, in pre-administration studies. Additionally, in a post-administration study, supplemental measurements were made at 1 and 3 h after cilostazol administration.
Infarct Volume
Twenty-four hours after MCA occlusion, rats were decapitated under ether anesthesia and the brains were rapidly removed, cooled in ice-cold saline for 10 mins, and cut into 2-mm-thick coronal sections in a cutting block. The brain slices were then stained with 2% 2,3,5-triphenyl-2H-tetrazolium chloride (TTC; Wako Pure Chemical Industries, Ltd, Tokyo, Japan) in saline solution at 37°C for 30 mins in the dark, arranged on a clear sheet, and scanned with a high-resolution scanner (gt-9500; Epson, Tokyo, Japan). Infarct volume was calculated with the trapezoidal rule using an image analyzer (win roof, Mitani Corporation, Tokyo, Japan) by one of the authors (H Ito) in a masked manner.
Evaluation of Long-Term Effect of Cilostazol
To assess the long-term effect of cilostazol in this model, we evaluated the cerebral ischemic lesion 3 days after MCA occlusion. We administered cilostazol (100 mg/kg) or vehicle solution to rat 2 h before and 1 h after MCA occlusion (day 0), twice (9:00 am and 5:00 pm) on days 1 and 2, and once (9:00 am) on day 3. TTC staining is a convenient procedure for detection and quantification of brain infarction 24 and 48 h after the onset of ischemia. At later time points, however, TTC methods underestimate the infarct volume because of reactive gliosis, macrophage infiltration, and other proliferative responses in the infarction (Liszczak et al, 1984). Therefore, to adequately examine the long-term effects of focal ischemia, infarct size was evaluated 3 days after MCA occlusion with hematoxylin–eosin (Wako Pure Chemical Industries, Tokyo, Japan). The rat brain was removed after perfusion with 4% paraformaldehyde phosphate buffer under halothane anesthesia. Then 10-μm-thick brain sections were prepared at 2-mm intervals, and were stained with hematoxylin–eosin. Infarct volume was calculated by the trapezoidal rule and expressed as the ratio of infarct to whole-brain volume. The neurological evaluation was performed on day 3 by Garcia's method with slight modification (Garcia et al, 1995).
NO Production and PGI2 Release In Vitro
Human brain microvascular endothelial cells (HBMECs; Applied Cell Biology Research Institute, Kirkland, WA, USA) were cultured in 5% CO2 at 37°C in a 100-mm culture dish in endothelial growth medium supplemented with 10% fetal bovine serum. Cells from passages 4–8 were used for all experiments.
Intracellular NO was monitored with 4-amino-5-methylamino-2′,7′-difluorofluorescein (DAF-FM) diacetate (Invitrogen, Carlsbad, CA, USA). HBMECs were seeded on glass chamber slide at a density of 5 × 105ccells/well in endothelial growth medium and incubated at 37°C for 10 mins in Dulbecco's Modified Eagle Medium containing 1 μM of DAF-FM diacetate. After loading with the NO indicator, cells were rinsed three times with endothelial growth medium and were pretreated with or without 1 mM N G-nitro-L-arginine methyl ester (L-NAME) for 30 mins, and then stimulated with vehicle (0.05% dimethyl sulfoxide) or 30 μM cilostazol for 15 mins. The glass slide chamber was placed on the stage of a confocal laser-scanning microscope (tcs-sp5; Leica Microsystems, Tokyo, Japan). Typically, four fields were chosen at random and NO fluorescence was measured using excitation (488 nm) and emission (520 nm) wavelengths.
For the PGI2 measurement, HBMECs were plated in 24-well culture plates at a density of 5 × 104 cells/well in culture media and cultured overnight. After 1 h incubation with culture media (250 μL) supplemented with test drugs at 37°C in a humidified CO2 incubator, supernatants were collected on ice and centrifuged to remove cell debris. The collected samples were stored at −80°C until measurement. PGI2 was assessed as 6-keto-prostaglandin-F1α (6-keto-PGF1α) using a commercial enzyme immunoassay kit (Cayman Chemicals, Ann Arbor, MI, USA) according to the manufacturer's instruction. Optical density was measured at 405 nm using a microplate reader (soft max; Molecular Devices, Tokyo, Japan). Results were expressed as a 6-keto-PGF1α concentration (pg/mL).
Data Analysis
In the
Results
Effects of Anti-Platelet Drugs on Platelet Aggregation
As shown in Figure 1, cilostazol at doses of 100 and 300 mg/kg did not significantly inhibit platelet aggregation induced by ADP or collagen. Clopidogrel significantly inhibited ADP- and collagen-induced platelet aggregation at 3 and 10 mg/kg, and at 10 mg/kg, respectively. Aspirin significantly attenuated collagen-induced platelet aggregation at 10 and 100 mg/kg, but did not affect ADP-induced platelet aggregation.
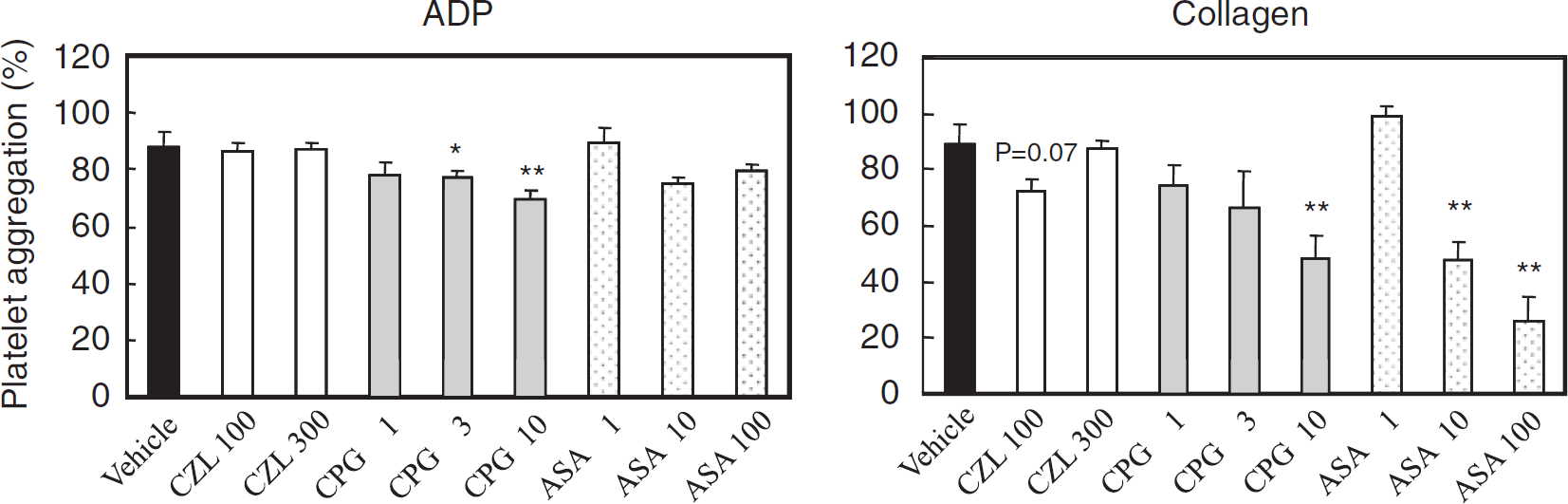
Effect of anti-platelet drugs on platelet aggregation
Physiological Variables
In the operated rats, physiological parameters were not different among the drug-treated groups and the control group, and between the pre-values (before MCA occlusion) and the post-values (after MCA occlusion), in the cilostazol pre-administration study, in the cilostazol post-administration study, and in the comparative study of anti-platelet drugs. The post-value of physiological parameters of the control group and cilostazol (100 mg/kg)-treated group in the cilostazol pre-administration study was as follows: rectal temperature, 36.2 ± 0.3°C and 36.1 ± 0.1°C; brain temperature, 36.8 ± 0.2°C and 36.5 ± 0.3°C; mean blood pressure, 209 ± 13 and 181 ± 27 mm Hg; heart rate, 298 ± 45 and 324 ± 26 beats/min; blood O2 gas pressure, 119 ± 13 and 119 ± 31 mm Hg; blood CO2 gas pressure, 46 ± 5 and 57 ± 27 mm Hg; blood pH, 7.33 ± 0.03 and 7.26 ± 0.10; and blood glucose levels, 144 ± 15 and 142 ± 29 mg/dL in the control and the cilostazol group, respectively.
Effects of Anti-Platelet Drugs on Infarct Size
In the pre-administration study, cilostazol significantly reduced the cerebral infarct area in the fourth section and the infarct volume at the higher dose (100 mg/kg) in comparison with the control group as shown in Figure 2A and 2B. Infarct volume (mm3) in the cilostazol (100 mg/kg)-treated group was significantly smaller, by 38%, than in the control group (50 ± 32 versus 81 ± 24 mm3,
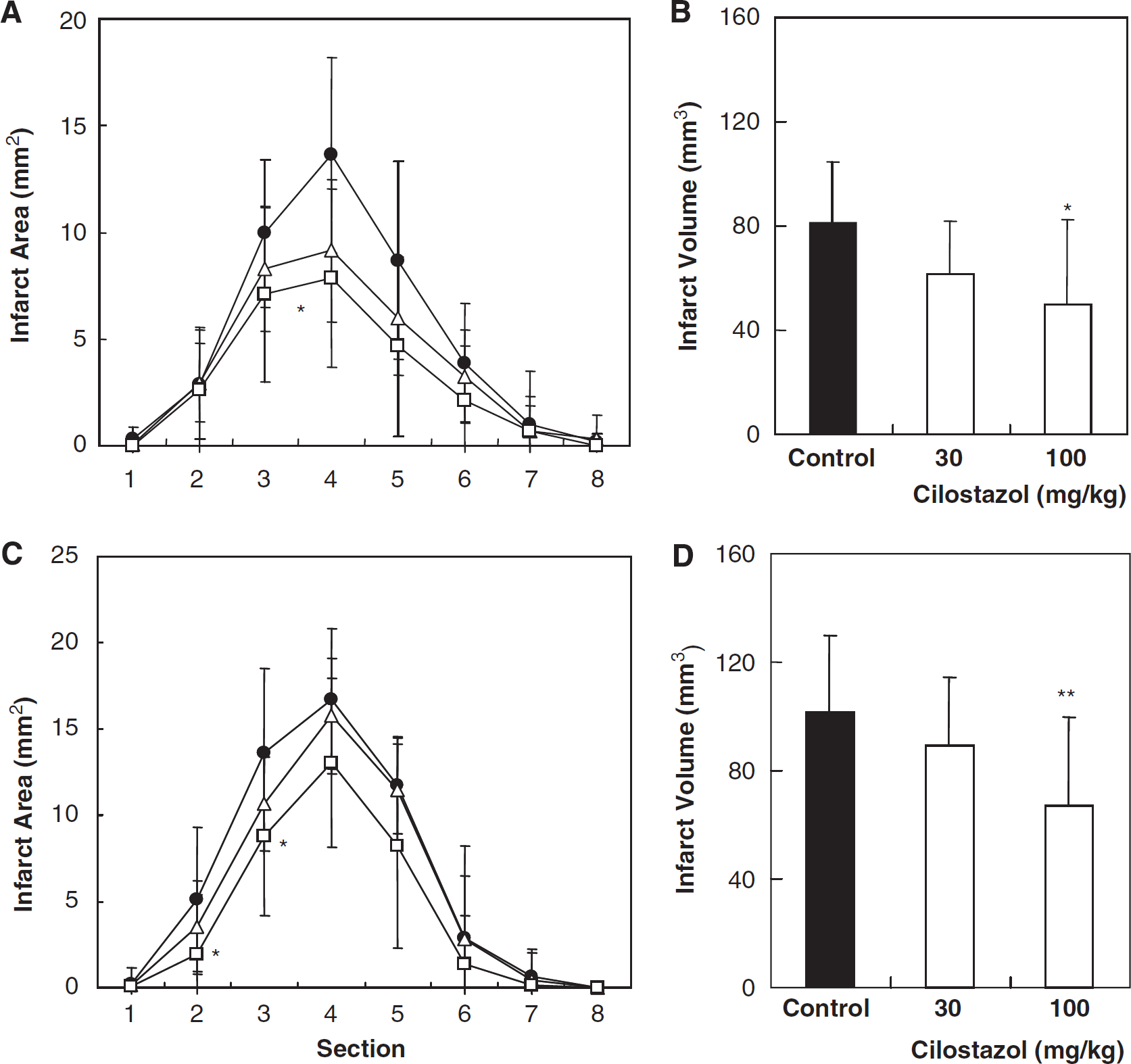
Pre- and post-administration of cilostazol-reduced infarct size. (
CBF after MCA Occlusion
Cilostazol significantly reversed the reduction in CBF after MCA occlusion at the points 1 and 2 mm lateral to the bregma (Figure 3). In the comparative study of anti-platelet drugs, clopidogrel (3 mg/kg) and aspirin (10 mg/kg) did not reduce infarct sizes (Figure 4A). The CBF in the rats treated with these two anti-platelet drugs was not different from that observed in the control group (Figure 4B). Additionally, arterial resistance was calculated by dividing femoral pressure by regional CBF. Cilostazol also significantly improved arterial resistance as compared with that in the control group at points 1 and 2 mm lateral to the bregma, by 42% and 46%, respectively (
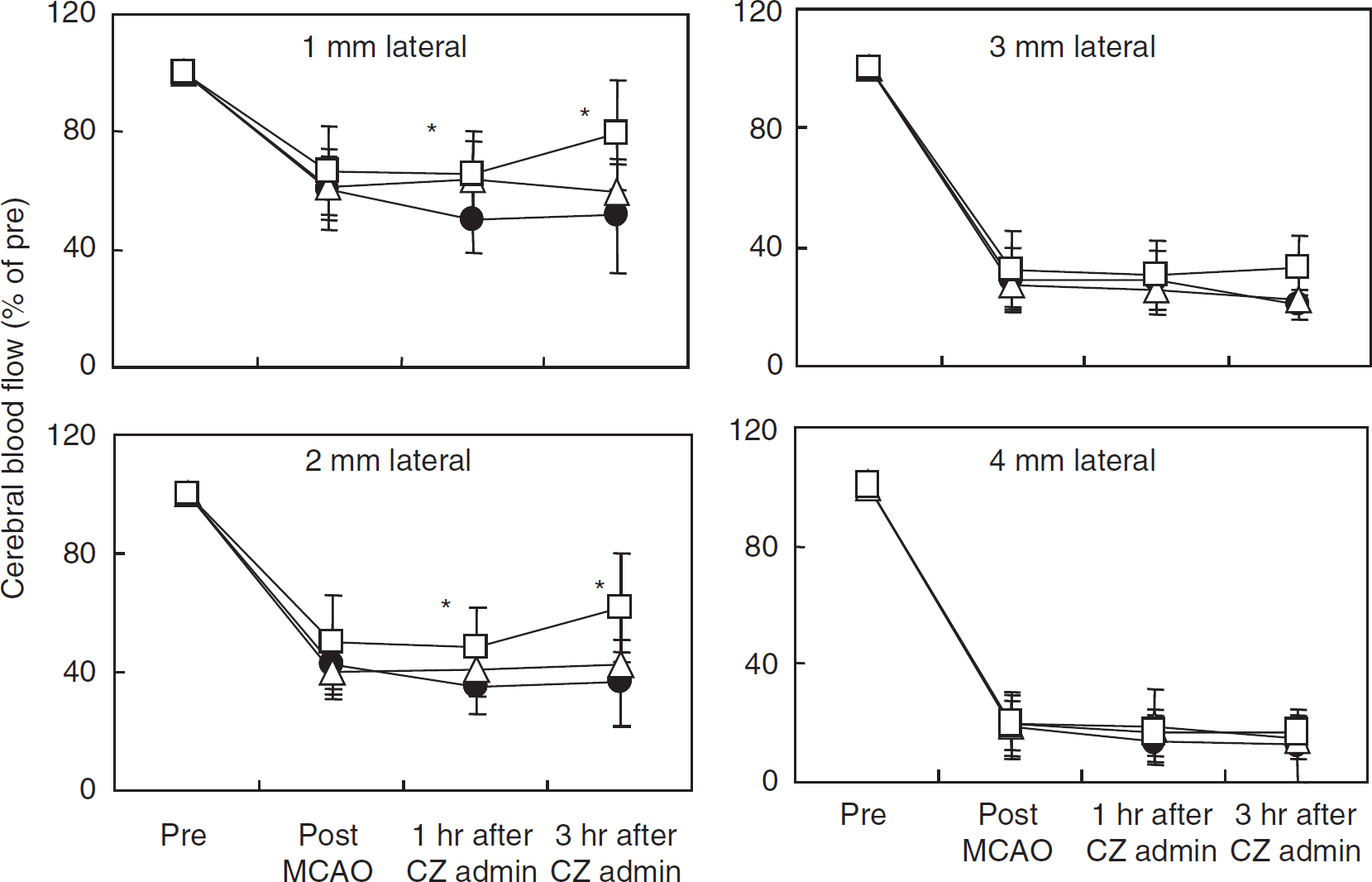
Regional CBF after MCA occlusion. Cilostazol was administered 30 mins after MCA occlusion. CBF was measured 10 mins before and after MCA occlusion, and 1 and 3 h after cilostazol administration. Cilostazol (100 mg/kg) significantly reversed the CBF reduction at points 1 mm posterior and 1 and 2 mm lateral to the bregma. Control, cilostazol (30 mg/kg), and cilostazol (100 mg/kg) are represented by closed circles, open triangles, and open squares, respectively. Data represent means ± s.d. (
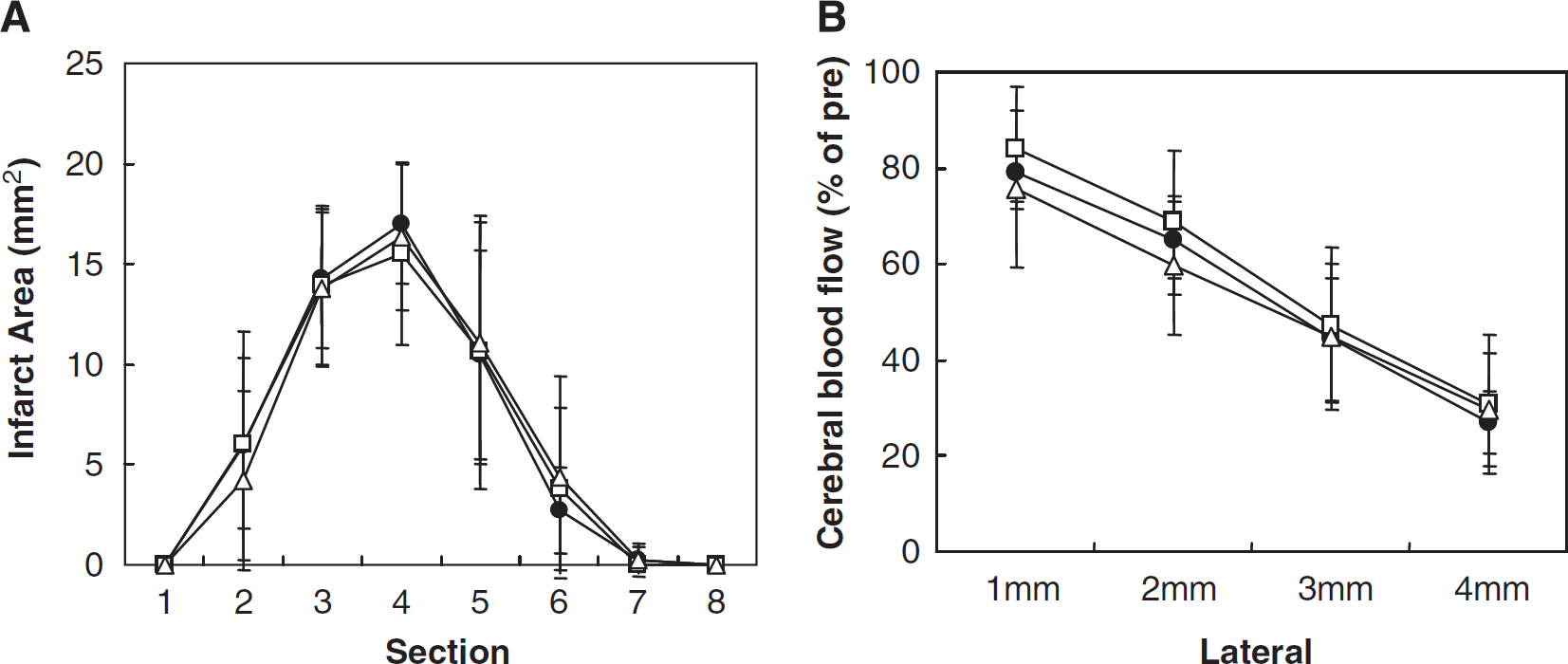
Effect of aspirin and clopidogrel on the infarct area (
Long-Term Effects of Cilostazol
Neurological score in the control and the cilostazol-treated group 3 days after MCA occlusion was 17.7 ± 0.8 and 17.7 ± 0.8 (a minimum neurological score of 3 and a maximum of 18). The neurological score remained normal even in the control group. Hence, we failed to find beneficial effects of cilostazol treatment on behavior. Infarct volume in the cilostazol-treated group 3 days after MCA occlusion was significantly smaller by, 48%, than in the control group (4.8 ± 2.2% (
Effects of Cilostazol on NO Production and PGI2 Release
Figure 5 presents representative DAF-FM images for NO production in HBMECs. Cilostazol significantly increased NO production in a concentration-dependent manner, which was decreased to control levels in the presence of an NOS inhibitor, L-NAME. As shown in Figure 6, cilostazol significantly increased PGI2 production in a concentration-dependent manner. Cilostazol-induced PGI2 production was completely inhibited by the cyclooxygenase inhibitor, aspirin.
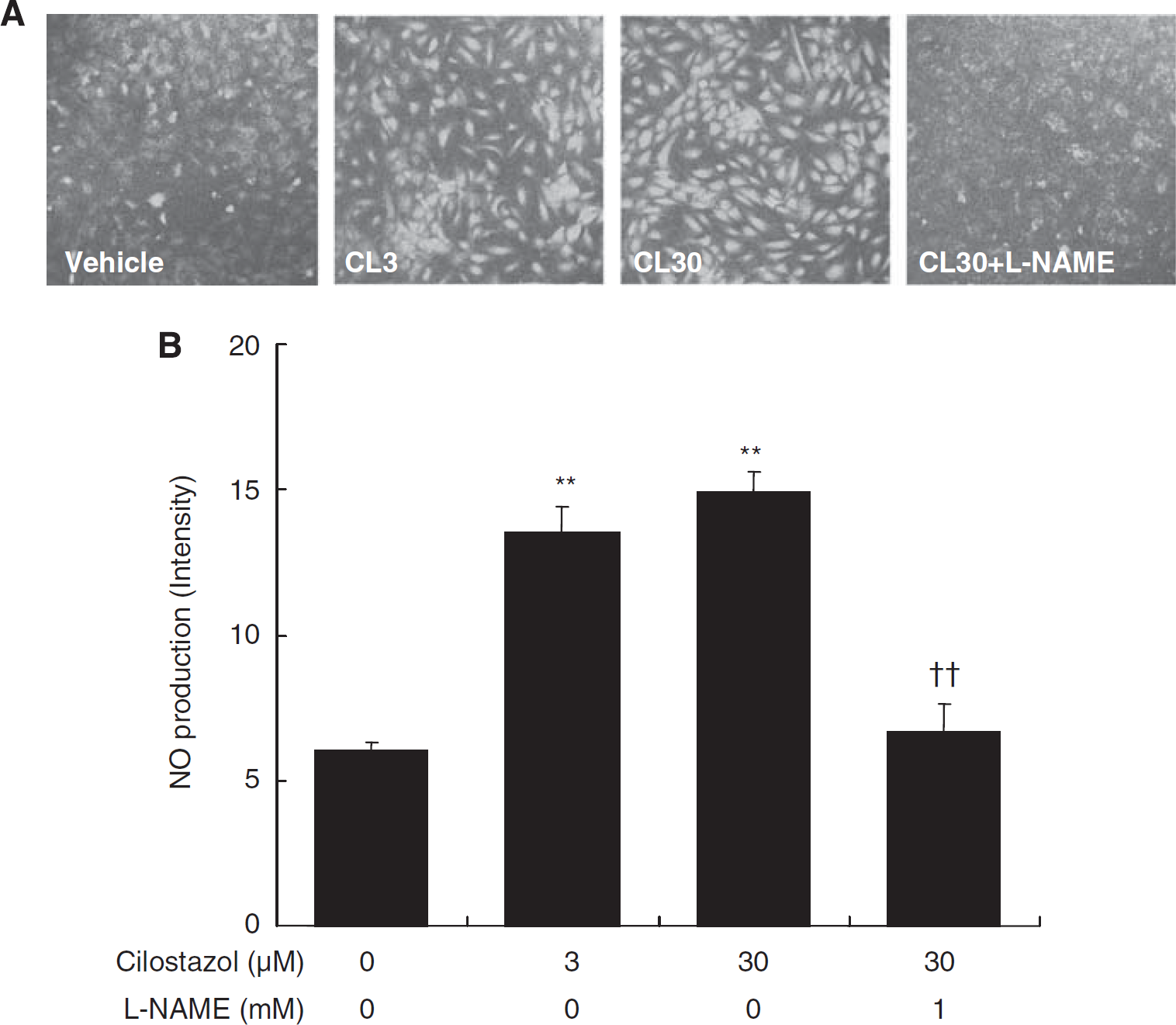
Effect of cilostazol on NO production in HBMECs. Typical fluorescence images of NO production, shown using a confocal laser-scanning microscope (
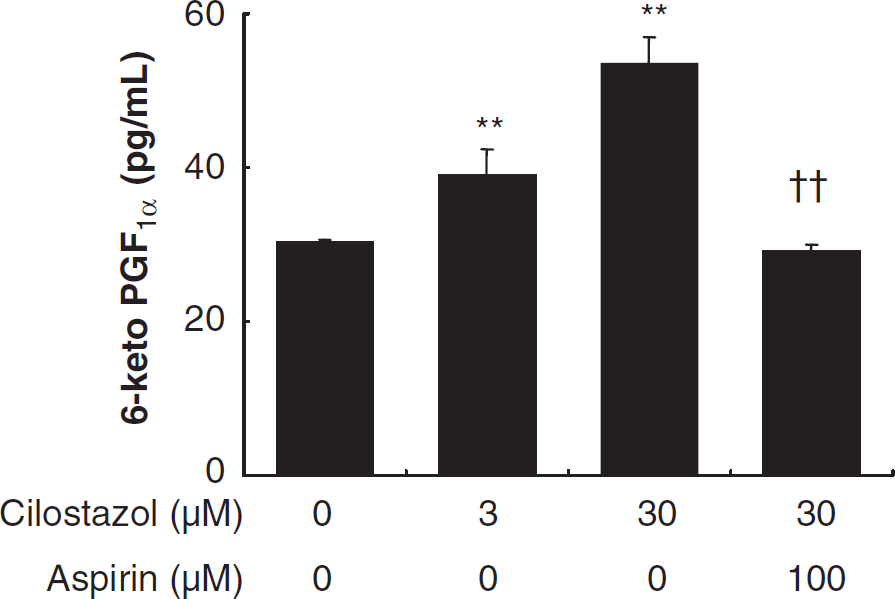
Effect of cilostazol on PGI2 release from HBMECs. Cilostazol induced PGI2 release in a concentration-dependent manner and the release was prevented by aspirin. Data represent means ± s.d. (
Discussion
The present study is the first study of cilostazol evaluation and comparative study with other anti-platelet drugs on brain infarction produced by photothrombotic MCA occlusion in SHRs. The effect of cilostazol on
The photothrombotic model of distal MCA occlusion in SHRs used in this study does not entail extensive surgery, thereby avoiding local tissue damage at the site of occlusion (Yao et al, 1996). SHRs used in this study have encompassed associated risk factors for stroke such as hypertension and aging. In addition, the average coefficient of variation of infarct volume was 21%, indicating that nine rats in each group are sufficient to detect a 30% reduction in infarct volume after treatment (Yao et al, 2003). Above all, the photothrombotic model has an advantage over mechanical MCA occlusion models in the evaluation of thrombotic stroke.
We examined the effects of three anti-platelet drugs on
We examined the effects of pre- and post-administration of cilostazol on CBF in this MCA occlusion model. Cilostazol significantly reduced the infarct sizes at 100 mg/kg, but not at 30 mg/kg, and the higher dose was associated with significant improvement in CBF in the post-administration study. With multi-point CBF measurement, we could detect the beneficial effect of cilostazol on ischemic CBF in the cortex that was perfused by collaterals (i.e., ischemic penumbra). The improvement of penumbral CBF by cilostazol may have contributed to reduction in infarct size. This improvement of penumbral CBF may be advantageous in treatment of clinical stroke.
Aspirin and clopidogrel did not reduce cerebral infarct size in the pretreatment study. This result coincided with the results of the study by Lee et al (2005) in a cerebral ischemia/reperfusion model in rats. The time needed to occlude the MCA was not prolonged by any anti-platelet drugs examined, and the MCA was consistently occluded within 4 mins of irradiation. Nevertheless, cilostazol decreased the infarct size. The efficacy of cilostazol in this model is largely attributable to mechanisms other than anti-platelet effects (i.e., improved CBF in the penumbra region). Recently, cilostazol has been shown to have pleiotropic effects other than anti-platelet and vasodilating actions. For example, cilostazol suppressed lipid peroxidation in the cerebral spinal fluid after subarachnoid hemorrhage in rat, as measured by malondialdehyde and 8-isoprostane contents (Ito et al, 2008). Cilostazol also inhibited the production of intracellular reactive oxygen species and apoptotic death in human umbilical vein endothelial cells (Kim et al, 2002). Reduction of oxidative stress by cilostazol might have contributed to protection from the brain injury that follows ischemia. Cilostazol induced NO production from endothelial NOS in human aortic endothelial cells (Hashimoto et al, 2006).
We demonstrated that cilostazol induced NO production and PGI2 release in HBMECs. These endogenous vasodilating substances are protective in cerebral ischemic models (Faraci, 1992; Karasawa et al, 2003; Wainwright et al, 2007). NO plays a dual role in cerebral ischemia. Depending on its source, NO may be toxic or protective to the brain under conditions of ischemia. The role of NO derived from L-arginine is unclear in ischemic brain tissue. Briefly, neuronal and inducible NOS play roles in nerve degeneration, while endothelial NOS plays a role in maintaining CBF and preventing neuronal injury in ischemic brain (Samdani et al, 1997). NO donors such as L-arginine increased CBF and reduced brain damage in mechanical MCA occlusion models (Morikawa et al, 1994; Zhang et al, 1994). Recently, cilostazol has increased the phosphorylation of endothelial nitric oxide synthase (eNOS) in the ischemic brain after MCA occlusion in rats (Nonaka et al, 2009). In the present study, therefore, NO production after phosphorylation of eNOS from cerebral endothelium, increased by cilostazol, might have improved CBF in the ischemic penumbra region.
The PGI2 release induced by cilostazol was prevented by aspirin treatment. PGI2 the plays roles of neuroprotector, anti-thrombotic and vasodilator (Cazevieille et al, 1993; Bath, 2004). Reduction of PGI2 is a risk factor for thromboembolic events in patients with cerebrovascular disorders (Akopov et al, 1993). Conversely, high-dose aspirin inhibits PGI2 synthesis in addition to thromboxane-A2 synthesis, and it may paradoxically enhance thrombogenesis
We examined the long-term effect of cilostazol 3 days after MCA occlusion. In this model, Prado et al (1996) demonstrated that a zone of infarction comprised the portions of dorsolateral and lateral neocortex of the ischemic hemisphere, and did not involve subcortical structures as well as our experience (Yao et al, 1996, 2003, 2009). It has generally been reported that the abnormality of behavior was hardly observed (Gonzalez and Kolb, 2003) when the ischemic region was restricted in the unilateral neocortex. Nevertheless, cilostazol treatment showed apparent long-term beneficial effects on cerebral infarction as exemplified by a 48% reduction in infarct volume at 3 days after MCA occlusion.
In conclusion, therapy with cilostazol appears to provide beneficial effects in thrombotic stroke, owing to an improvement of CBF in the ischemic penumbral zone. Cilostazol-increased NO production and PGI2 release from the brain endothelium may protect endothelial and neuronal cells after ischemic stroke, although proof for involvements of these endogenous mediators in neuroprotection needs further experiments. Therefore, we expect cilostazol to ameliorate acute cerebral ischemic injury in the clinical setting.