202. Intracranial hemorrhage in mice with acute rise in blood pressure during chronic hypertension
Y. Wakisaka1, Y. Chu1, J.D. Miller1, G.A. Rosenberg2 and D.D. Heistad1,3,4
1Internal Medicine, University of Iowa, Iowa City, Iowa; 2Neurology, University of New Mexico Health Sciences Center, Albuquerque, New Mexico; 3Pharmacology, University of Iowa; 4VA Medical Center, Iowa City, Iowa, USA
Objectives: Acute as well as chronic hypertension (HT) is a risk factor for intracranial hemorrhage (ICH). We have developed new models of spontaneous ICH with acute, superimposed on chronic, hypertension. We tested the hypotheses that increases in oxidative stress and activation of matrix metalloproteinase (MMP)-9 are associated with, and may precede, spontaneous ICH during hypertension, and that susceptibility to ICH would be increased more by angiotenin-II (AngII) than by norepinephrine (NE) because of the pro-oxidant effects of AngII.
Methods: Chronic HT was produced in C57BL/6 mice with AngII-infusion and L-NAME. One week later, acute HT was produced in some chronic HT mice by daily subcutaneous injection of AngII (chronic/acute HT-AngII group) or NE (chronic/acute HT-NE group). Superoxide was measured in brain homogenates using lucigenin-enhanced chemiluminescence. MMPs levels were estimated by gelatin zymography and by in situ zymography.
Results: Systolic blood pressure (SBP) increased to 163±3 (mean±SE) mm Hg 7 days after start of AngII-infusion and L-NAME. Injection of AngII transiently increased SBP in chronic/acute HT-AngII mice (ΔSBP: 57±4 mm Hg). Eleven of 15 chronic/acute HT-AngII mice developed neurological signs after 15±1 days. ICH was demonstrated with histological examination. Only one of 15 chronic HT mice, without acute HT, developed ICH. Superoxide was low in control mice, increased in chronic HT mice (3.8±0.2 fold versus control), increased further in chronic/acute HT-AngII mice without ICH (6.5±0.6), and was highest in chronic/acute HT-AngII mice with ICH (11.4±1.2) (each, P<0.01 versus control). NAD(P)H oxidase activity (superoxide after addition of 100 μM NADPH) increased in parallel with changes in superoxide. RT-PCR revealed that Nox4 was upregulated and SOD2, SOD3, and catalase were downregulated in chronic/acute HT-AngII mice with and without ICH. Expression of several other pro- and anti-oxidant enzymes was unchanged. Changes in MMP-9 levels (gelatin zymography) also paralleled oxidative stress, with no changes in MMP-2 levels. In situ zymography showed that activated MMPs and an oxidative stress marker were co-localized on extracellular matrix and endothelium of cerebral vessels, especially in vessels that appeared to be associated with ICH. When chronic HT mice received injections of NE, SBP increased more than chronic/acute HT-AngII mice (ΔSBP: 68±3, P<0.01), but incidence of neurological signs was less than in chronic/acute HT-AngII mice (40% versus 73%). Histological studies showed that chronic/acute HT-NE mice developed significantly fewer ICH than chronic/acute HT-AngII mice. Levels of oxidative stress and MMP-9 did not increase in chronic/acute HT-NE mice without ICH compared to those of chronic HT mice, and were significantly less than those of chronic/acute HT-AngII mice with and without ICH.
Conclusion: We have developed new models of ICH in mice with acute, superimposed on chronic, hypertension. AngII-mediated acute HT increased oxidative stress and levels of MMP-9, with increased propensity for ICH. Incidence and number of ICH were greater during AngII- than NE-induced acute HT, perhaps related to the extraordinary pro-oxidant effects of AngII. The findings suggest that acute HT induced by AngII, and less by NE, may play a critical role in spontaneous ICH during chronic HT.
346. Vascular adhesion Protein-1 (VAP-1/sSAO) is involved in intracranial hemorrhagic complications after thrombolysis in human stroke
J. Montaner1,2, M. Hernández-Guillamon1, M. Solé3, M. Parés1, E. Cuadrado1, T. Valente3, L. Garcia-Bonilla1, M. Ribó2, M. Rubiera2, C. Molina2, J. Alvarez-Sabín2, A. Rosell1 and M. Unzeta3
1Neurovascular Research Laboratory; 2Neurovascular Unit, Department of Neurology, Vall d'Hebron Hospital; 3Biochemistry and Molecular Biology, Neuroscience Institute, Autonomous University of Barcelona, Barcelona, Spain
Objectives: Vascular adhesion protein-1 (VAP-1) is a cell surface and soluble molecule that possesses semicarbazide-sensitive amine oxidase (SSAO) activity; which oxidatively deaminates primary amines (generating hydrogen peroxide, ammonia and the corresponding aldehyde) and plays a role in leukocyte transmigration through the inflamed vasculature. Leucocytes secrete proteases after tPA treatment contributing to BBB disruption. Therefore, we aimed to investigate for the first time the role of VAP-1 in hemorrhagic transformation (HT).
Methods: VAP-1/SSAO activity was determined radiochemically (pmol/min mg protein) in 141 consecutive ischemic strokes involving the middle cerebral artery territory who received t-PA. Blood samples were obtained at baseline (pretreatment), in all patients. Hemorrhagic events were classified according to computed tomography (CT) criteria petechial hemorrhagic infarctions (HI,1–2) and large parenchymal hemorrhages (PH,1–2 and remote PH). Brain CT scan was obtained at 24 to 48 h or when a neurological worsening occurred. To calculate the sensitivity and specificity for VAP-1 values to predict brain bleedings a receiver operator characteristic (ROC) curve was configured. A replication study was conducted using cases from our plasma-library of t-PA treated patients [40 PH patients matched to 40 without HT]. Finally, SSAO/VAP-1 immunostaining of brain microvascular vessels was performed in 8 deceased stroke patients (2 without HT and 6 with HT). One of the cases with HT received thrombolytic treatment 3 days before death and the other cases suffered spontaneous hemorrhagic transformations. All brain samples were obtained within the first six hours after death.
Results: HT was present in 48 (34.3%) patients 21 (15%) HI-1, 11 (7.9%) HI-2, 10 (7.1%) PH-1, 3 (2.1%) PH-2 and 3 (2.1%) PH-R. An increased baseline VAP-1 level was found among patients who later on develop a HT (P<0.001). Moreover, the highest baseline VAP-1 level was found in patients with an ulterior PH and the lowest baseline VAP-1 level in those without HT (PH: 3.41±1.07, non-HT: 2.48±0.92 and HI: 2.79±0.75; P = 0.001). For HT, VAP-1 (>2.7) was the main baseline predictor of HT appearance [OR 5.84 (2.16 to 15.80), P = 0.001] and also hyperglycemia was independently associated to HT [OR 1.03 (1.007 to 1.05), P = 0.008]. Baseline VAP-1 (>3.07) was the only predictor independently associated to PH appearance OR [8.94 (2.29 to 34.93), P = 0.002]. In the subgroup of athrothrombotic strokes a cut-off of VAP-1 = 3.12 had a 100% sensitivity and 100% specificity to identify PH. The replication study confirmed those results (data not shown). In the histological sub-study, brain samples with HT areas showed a strong SSAO/VAP-1 inmunostaining compared to the corresponding contralateral areas. SSAO/VAP-1 inmunostaining was associated with white blood cell extravasations and infiltration in those HT areas supporting our findings in the blood stream.
Conclusions: Baseline VAP-1 level predicts PH appearance after t-PA treatment. In the near future, VAP-1 determination might increase the safety profile for thrombolysis and anti-VAP-1 drugs might be combined with t-PA to prevent hemorrhagic complications.
367. MRI surrogate measures of blood-brain barrier permeability for the prediction of hemorrhagic transformation in acute ischemic stroke
A. Kassner1,2, S. Chen2, R. Thornhill1,2, W. Rammo2 and D. Mikulis3
1Physiology and Experimental Medicine, Hospital for Sick Children; 2Medical Imaging, University of Toronto; 3Medical Imaging, Toronto Western Hospital, Toronto, ON, Canada
Objectives: Therapeutic use of recombinant tissue plasminogen activators (rt-PA) in acute ischemic stroke (AIS) is currently limited to patients presenting ⩽4.5 h post-ictus, due to the increased risk of hemorrhagic transformation (HT).1 It has been shown that permeability MRI followed by tracer-kinetic modelling can be used to predict HT.2 However, recent work suggests that information relating to blood-brain barrier permeability can be more rapidly extracted from the recirculation-phase of routine ‘dynamic susceptibility contrast’ (DSC) MRI images.3–5 Our purpose was to evaluate four distinct DSC parameters in discriminating between AIS patients who will proceed to HT and those who will not.
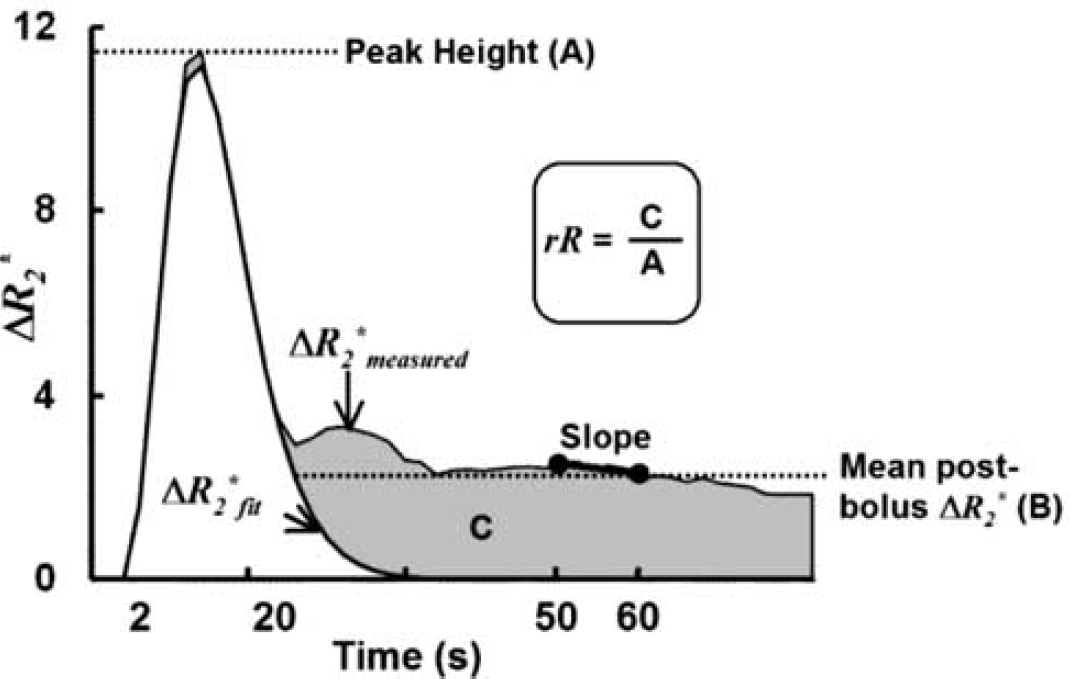
Methods: Eighteen AIS patients were examined <6 h post-ictus. All imaging was performed on a 1.5T clinical MRI system (GE Signa LX 12.0, Milwaukee, WI). DSC imaging consisted of a single-shot EPI scan with TR 1725 ms, TE 31.5 ms, FOV 240 mm, matrix size 96 × 64, flip angle 90°, slice-thickness 5 mm, 17 slices, and acquisition time 86 s. Gadodiamide was injected as a bolus (Omniscan, GE, USA) at the initiation of DSC. HT was determined by follow-up CT or MRI 24 to 72 h later. Data were analyzed offline. Two regions of interests (ROIs) were defined on diffusion-weighted MRIs, one within the infarct and another within the contralateral hemisphere and then copied to the equivalent DSC images. Mean values were recorded for each of the following four DSC parameters: relative-recirculation (‘rR’),3 Peak Height,4 %Recovery of the ΔR2* versus time curve (%Recovery = 100 × (A−B)/A)4), and Slope of the ΔR2* versus time curve between 50 to 60 s post-injection5 (Figure 1). Data were grouped based on follow-up HT-status. For each parameter, differences between ROIs as well as between HT and non-HT patients were assessed using Wilcoxon matched pairs and Mann-Whitney U tests, respectively.
Results: Eight patients proceeded to HT. While the mean rR for infarcts was significantly greater than for contralateral ROIs (0.18±0.02 versus 0.08±0.01, P<0.001), the converse was true for %Recovery (79±9 versus 91%±3%, P<0.001). The mean infarct rR for HT patients was significantly greater than for non-HT patients (0.22±0.06 versus 0.14±0.06, P<0.001), while the mean %Recovery in HT patients was significantly lower than in non-HT patients (76±6 versus 82%±11%, P<0.05). No significant differences were detected with respect to Peak Height or Slope.
Conclusions: Both rR and %Recovery can be readily extracted from a standard 90 s DSC data-set and each shows potential for delineating HT from non-HT infarcts.
429. Multiparametric MRI of pathophysiological processes involved in hermorrhagic transformation after embolic stroke in spontaneously hypertensive rats
I.A.C.W. Tiebosch, R. Zwartbol, M.J.R.J. Bouts and R.M. Dijkhuizen
Image Sciences Institute, University Medical Center Utrecht, Utrecht, The Netherlands
Objectives: Risk of hemorrhagic transformation (HT) limits thrombolytic treatment against acute ischemic stroke. Elucidation and delineation of the pathophysiological basis of HT after stroke may lead to improvement of treatment strategies. Multiparametric MRI uniquely allows serial in vivo assessment of multiple pathophysiological processes involved in HT.1 The goal of this study is to characterize MRI profiles of ischemic regions that develop HT in a clinically relevant model of embolic stroke in spontaneously hypertensive rats.
Methods: Spontaneously hypertensive rats (SHRs, n = 17) were subjected to unilateral embolic ischemic stroke2 as part of a large study on effects of combination treatment strategies. Researchers are blinded for treatment assignments. At 0–2 h, 24 h and 7 days post-stroke, tissue damage, perfusion status and blood-brain barrier (BBB) integrity were assessed with diffusion-, T2-, T2*-, perfusion- and post-contrast (Gadobutrol) T1-weighted MRI.3 After MRI at day 7, rats were sacrificed and brains were excised and sectioned. Regions with clear blood accumulation within the ischemic lesion were identified as HT areas. HT regions and non-HT areas within the lesion, as well as their contralateral counterparts, were outlined on the MR images. The temporal profiles of the T2, T2*, apparent diffusion coefficient (ADC), cerebral blood flow index (CBFi), cerebral blood volume (CBV) and contrast leakage through the BBB were measured in these regions and satistically compared by a repeated measures one-way ANOVA with post hoc Student-Newman-Keuls testing (P<0.05 was considered significant).
Results: Eleven SHRs completed the experimental protocol, of which five showed HT.
Acutely after stroke, ADC and CBFi were significantly reduced in HT and non-HT areas. Contrast-enhanced T1-weighted signal was significantly elevated in HT but not in non-HT regions.
After 24 h, ADC was still decreased in the entire ischemic lesion, while T2, T2* and contrast leakage had increased. In HT regions, T2 elevation and contrast leakage were larger than in non-HT areas. In addition, CBV and CBFi were considerably lowered in HT regions at this stage.
At day 7, when HT was identified histologically, T2* values were significantly lower in HT as compared to non-HT regions (but not as compared to contralateral). Also, contrast leakage remained strongly elevated in HT areas.
Conclusions: We found that HT after stroke in SHRs, particularly after 24 h, is associated with locally reduced perfusion, largely increased BBB leakage and substantial edema, indicative of severe ischemia. HT may be directly detected by T2* shortening,4 however in our study T2* in HT areas was considerably influenced by T2* prolongation due to edema formation. Nevertheless, HT was implied by a T2* drop between 24 h and 7 days, which was not the case for the non-HT regions. Our study confirms that multiparametric MRI allows characterization of pathophysiological processes involved in HT. Furthermore, MRI of perfusion status and BBB integrity may provide prognostic information on risk of HT after stroke.
Funding: Netherlands Heart Foundation (2005B156).
697. PJ34, a poly(ADP-ribose) polymerase inhibitor, reduced tissue plasminogen activator-induced hemorrhage after permanent cerebral ischemia in mice
M. Haddad, M. Plotkine and I. Margaill
Pharmacology of Cerebral Circulation EA2510, Paris Descartes University, Paris, France
Objectives: Tissue plasminogen activator (tPA) remains the only pharmacological treatment for acute ischemic stroke. However the increased risk of intracerebral hemorrhage after tPA largely contributes to limit its widespread use. tPA-induced hemorrhage seems to be related to the capacity of the thrombolytic to up-regulate matrix metalloproteinase-9 known to degrade the basal membrane components of blood vessels.1 Furthermore in a model of cerebral ischemia, the poly(ADP-ribose) polymerase (PARP) inhibitor 3-aminobenzamide was shown to reduce brain MMP-9 overexpression.2 In this context, we investigated whether the potent PARP inhibitor, PJ34 (N-(6-oxo-5,6-dihydrophenanthridin-2-yl)-2-(N,N-dimethylamino-acetamide), affected the rate of hemorrhage due to tPA therapy in a model of permanent cerebral ischemia.
Methods: Ischemia consisted in an intravascular occlusion of the left middle cerebral artery in male Swiss mice (30 g) anesthetized with i.p. ketamine (50 mg/kg) and xylazine hydrochloride (6 mg/kg). Mice received either recombinant tPA (rtPA, Actilyse®, 10 mg/kg, i.v. 6 h after the onset of ischemia as a 10% bolus followed by an infusion over 30 min) or a combination of rtPA with the same protocol and PJ34 (3 to 6 or 12 mg/kg, i.p. just after and 4 h after the onset of ischemia). Control ischemic animals received the vehicle of rtPA and PJ34 (saline) with the same protocol. The neurological deficit (evaluated by a grip and a string test), infarct volume and intracerebral hemorrhage (counted on twelve 20-μm-thick coronal brain slices) were assessed 48 h after ischemia.
Results: The rt-PA-treated ischemic mice showed a significant increased score of intracerebral hemorrhage compared to saline-treated ischemic mice (83±10 versus 50±8, P<0.05). PJ34 reduced rt-PA-induced aggravation of hemorrhagic score at 3 mg/kg (37±7, P<0.01) and 6 mg/kg (52±11, P<0.05). PJ34 at 3 mg/kg also significantly improved the score in the string test (P<0.05) and tended to reduce the deficit in the grip test (P = 0.07). Whatever the dosage, PJ34 had no effect on the infarct volume.
Conclusions: The present study demonstrates that PARP inhibition prevents rtPA-aggravation of both intracerebral hemorrhage and neurologic deficit. Thus PARP inhibition could be a valuable strategy to optimise tPA thrombolysis in stroke.
933. Hemorrhagic stroke associated with poor outcome after infective endocarditis
T. Ohtsuki, E. Nomura, S. Aoki, Y. Sueda, T. Kono, K. Kawase, K. Ochi, T. Ohshita, T. Nakamura, T. Kohriyama and M. Matsumoto
Department of Neurology, Hiroshima University Hospital, Hiroshima, Japan
Objectives: Infective endocarditis causes not only ischemic stroke by bacterial emboli, but also hemorrhagic stroke by inflamed arteries or aneurysms prone to rupture that often makes our decision for the requisite surgery hard. We examined if hemorrhagic stroke detected by CT was associated with poor outcome after stroke caused by infective endocarditis, as compared with pure ischemic stroke.
Patients and methods: We conducted the observational study on 22 consecutive patients (12 men, aged 23 to 82, median 57) with acute symptomatic stroke after definite or possible infective endocarditis according to the Duke University criteria from October 2005 to September 2008. Brain hemorrhage and infarction responsible for neurological signs were verified by CT and diffusion-weighed image of MRI, respectively. We evaluated modified Rankin Scale (mRS) at 3 months after stroke and divided each patient into either favorable outcome with mRS score of 0 to 1 or poor outcome of from disability to death, mRS score of 2 to 6. Best medical treatment and surgical repair of the damaged heart valves that cardiovascular doctors decided for if necessary were provided to each patient according to the Japanese Circulation Society guideline for treatment of infective endocarditis.
Results: While 2 hemorrhage and 13 infarction were noted in 15 patients of the favorable outcome group, 7 patients of the poor outcome group consisted of subarachnoid hemorrhage in 3, parenchymal hematoma on infarcts in 3 and multiple infarction in 1. Out of the poor outcome group, 4 died of recurrent intracranial bleeding. The poor consequence group had brain hemorrhage detected by CT more frequently than the favorable outcome group (P<0.01: Mann-Whitney U-test). Statistically observed between the poor outcome and favorable outcome groups were no significant differences of age, gender, presence of disturbed consciousness or hemiplegia on admission, involvement of mitral valve, attachment of 1-cm or larger vegetations to valves, isolation of staphylococcus aureus from blood, recurrence of stroke, embolization to other organs than the brain and complication of meningitis/brain and intraocular abscess. The 8 of 13 ischemic patients had cardiac valves repaired 2 to 4 weeks after stroke to lead to favorable outcome. In contrast, out of 9 hemorrhagic stroke patients 4 cancelled the expected operations, while 5 underwent open-heart surgery, one of which led to parenchymal hematoma in vain during surgery. As a result, 6 of 8 hemorrhagic stroke led to poor prognosis, while 13 out of 14 ischemic stroke got advantageous outcome. Poor outcomes were more frequent in hemorrhagic stroke than in infarction (Hazards ratio 39.0: 95% CI, 2.9 to 518).
Conclusions: Hemorrhagic stroke on CT was independently associated with poor neurological outcome after infective endocarditis, as well as the formidable complication of intracranial hemorrhage during extracorporeal circulation as described previously,1 that could make us deferring open-heart surgery after infective endocarditis.
References
1.
HackeW. NEJM2008;359:1317–29.
2.
KassnerA. AJNR2005;26:2213–17.
3.
KassnerA. JMRI2000;103–13.
4.
LupoJM. AJNR2005;26:1446–54.
5.
BangOY. Ann Neurol2007;62:170–76.
6.
Jiang. JCBFM2002;22(5):559–68.
7.
Zhang. Brain Res1997;766:83–92.
8.
Dijkhuizen. JCBFM2001;33(8):2100–04.
9.
Neumann-Haefelin. Neuroreport2001;12:309–311.
10.
Tsuji. Stroke2005;36:1954–9.
11.
Koh. Toxicology2005;214:131–9.
12.
RuttmannE. Neurological outcomes of septic cardioembolic stroke after infective endocarditis. Stroke2006;37:2094–9.