
Abstract
Our laboratory has shown in numerous experiments that the neurosteroids progesterone (PROG) and allopregnanolone (ALLO) improve molecular and functional outcomes after traumatic brain injury (TBI). As coagulopathy is an important contributor to the secondary destruction of nervous tissue, we hypothesized that PROG and ALLO administration may also have a beneficial effect on coagulation protein expression after TBI. Adult male Sprague—Dawley rats were given bilateral contusions of the medial frontal cortex followed by treatments with PROG (16 mg/kg), ALLO (8 mg/kg), or vehicle (22.5% hydroxypropyl-β-cyclodextrin). Controls received no injury or injections. Progesterone generally maintained procoagulant (thrombin, fibrinogen, and coagulation factor XIII), whereas ALLO increased anticoagulant protein expression (tissue-type plasminogen activator, tPA). In addition, PROG significantly increased the ratio of tPA bound to neuroserpin, a serine protease inhibitor that can reduce the activity of tPA. Our findings suggest that in a model of TBI, where blood loss may exacerbate injury, it may be preferable to treat patients with PROG, whereas it might be more appropriate to use ALLO as a treatment for thrombotic stroke, where a reduction in coagulation would be more beneficial.
Introduction
Over the last few years, studies from several laboratories, including ours, have shown that acute progesterone (PROG) treatments can substantially reduce the morphologic and behavioral impairments caused by both traumatic brain injury (TBI) and stroke (Shear et al, 2002; Gibson and Murphy, 2004; Goss et al, 2003; Cutler et al, 2005; O'Connor et al, 2005; Sayeed et al, 2006; Hoffman et al, 2006; Schumacher et al, 2007b). In addition to animal studies, a recent randomized, double-blind, placebo-controlled clinical trial using 3 days of intravenous PROG to treat moderately to severely brain-injured patients demonstrated both safety and efficacy compared with the patients given state-of-the-art treatment plus placebo (Wright et al, 2007). The severely injured patients given PROG had almost a 60% reduction in mortality and a significantly better functional outcome at 30 days after injury. Despite the promising outcomes shown in these studies, the specific mechanisms by which neurosteroids act to enhance neuroprotection are still not completely defined.
We have previously demonstrated that PROG and its metabolite allopregnanolone (ALLO) are potent neuroprotective agents (Djebaili et al, 2005; He et al, 2004). However, they exhibit somewhat different pharmacological properties. On one hand, ALLO does not act as a ligand at the classical PROG nuclear receptor (Rupprecht et al, 1993), the putative PROG membrane receptor (Meffre et al, 2005), or the glucocorticoid receptor (Herkert et al, 2001). On the other hand, and unlike ALLO, PROG does not directly increase GABAergic transmission (Ciriza et al, 2006). Physiologically, the divergent actions of the two neurosteroids may be attributable to the fact that the conversion of PROG to ALLO takes place primarily in the brain, and not in the serum (Schumacher et al, 2007b).
Traumatic brain injury frequently results in diffuse intravascular coagulation as a result of a massive release of tissue factor (thromboplastin) into the systemic circulation after injury (Stein and Smith, 2004). Diffuse intravascular coagulation leads to uncontrolled procoagulant activity with a rapid consumption of clotting factors, induction of fibrinolysis, and hypocoagulation, further contributing to secondary ischemic injury, inflammation, posttraumatic hemorrhaging, and poor clinical outcome (Stein et al, 2002, 2004). Some form of coagulopathy has been observed in more than 60% of severe TBIs, and in 15% to 35% of all TBIs (Stein et al, 2002). As PROG and ALLO appear to be protective in TBI, we hypothesized that they will also have effects on the expression of hemostatic proteins. There are reports that PROG may increase levels of coagulation factors in breast cancer tissue (Kato et al, 2005), arterial walls (Herkert et al, 2001), and the uterus (Schindler, 2003). In contrast, recent clinical trials using tissue-type plasminogen activator (tPA) as a thrombolytic agent in stroke patients have shown that female patients benefit more than male patients with regard to postinfarct lesion size and functional recovery (Savitz et al, 2005). As estrogen is generally higher in women and has been found to stimulate the conversion of PROG to ALLO in both serum and brain (Frye and Rhodes, 2005), it is possible that an increased ALLO to PROG ratio is responsible for this enhanced anticoagulant effect. Progesterone and ALLO may therefore have divergent effects on coagulation factor expression, which may be an important parameter in the choice of steroid treatment for different kinds of brain injury, for example, ALLO for thrombotic stroke (ALLO), but PROG for blunt or penetrating brain injuries with a significant hemorrhagic component.
Here we evaluate the effects of both PROG and ALLO on five major components of the coagulation cascade after TBI: thrombin, tPA, neuroserpin, fibrinogen, and coagulation factor XIII (cFXIII). We also examined blood-clotting times for both PROG and ALLO in our brain-injured animals. We hypothesize that, although both neurosteroids have similar effects on inflammatory and edema-inducing factors after TBI, they might differ in their effects on hemostatic protein expression and on coagulation.
Materials and methods
Animal Protocol
A total of 64 male Sprague—Dawley rats (8 to 12 weeks old) weighing 275 to 300 g were used as subjects. Twelve rats were randomly assigned to each of four treatment groups according to standard experimental procedures. Six rats from each group were used for gene expression analysis and six for protein expression assays. An additional 16 animals were used for systemic coagulation measurements. This study was conducted in a facility approved by the American Association for the Accreditation of Laboratory Animal Care in accordance with NIH guidelines. All experimental animal procedures were approved by the Emory University Institutional Animal Care and Use Committee, Protocol no. 146-2005.
Controlled Cortical Impact Model
Rats were anesthetized with 2.5% isoflurane (4 mins) before and during surgery. Body temperature was monitored and maintained by a homeothermic heating blanket system (Harvard Apparatus, Holliston, MA, USA). Pulse oximetry was used to maintain heart rate at approximately 350 beats per minute with blood oxygen saturation levels > 95%. Animals were placed in a stereotaxic frame and their heads held horizontally in place by bars inserted in the ears. A midline incision was made to expose the skull, and a 6-mm-diameter craniotomy was made along the midline, 3 mm rostral to bregma, in order to gain access to the medial frontal cortex. The cortical contusion was created to a depth 3.5 mm ventral to bregma by a pneumatically driven 5-mm-diameter steel impactor at a velocity of 2.25 m/sec and impact time of 170 ms. Sham rats underwent the same procedure but without craniotomy or impact.
Hormone Administration
Progesterone (16 mg/kg), ALLO (8 mg/kg), and vehicle (22.5% 2-hydroxypropyl-β-cyclodextrin) were administered intraperitoneally at 1 h after TBI and subcutaneously at 6 h followed by one injection every 24 h until the animals were killed and their brains removed for molecular assays. The treatment protocol was based on previous studies in our laboratory (Goss et al, 2003). Sham groups received no injury or injections. Animals were killed with a lethal dose of Nembutal at 48 h after TBI for mRNA analysis and at 72 h for protein analysis.
Reverse Transcriptase-Polymerase Chain Reaction
At 48 h after TBI, the medial frontal cortex was dissected and total RNA extracted as previously described (He et al, 2004). Invitrogen SuperScript First-Strand Synthesis System for RT-PCR (Invitrogen, Carlsbad, CA, USA; 11904-018) was used to synthesize cDNA from total RNA using random primers. This 48 h time point for mRNA analysis was chosen to determine whether changes in the protein expression profile at 72 h could be predicted by gene expression at 48 h.
Real-time PCR was performed in a 50-mUL reaction using 5 μL of the diluted first-strand cDNA template, an optimized quantity of primers, water, and 25 pL of the 2 × SYBR Green I dye PCR Master Mix (Applied Biosystems, Foster City, CA, USA). PCR reactions were performed at 50°C for 2 mins, 95°C for 10 mins, and 40 cycles of 95°C for 15 secs and 60°C for 1 min. 18S ribosomal RNA abundance was also amplified using real-time PCR to normalize for nucleic acid loading (Ambion, Austin, TX, USA). Primers were designed using Primer Express software (Applied Biosystems) and synthesized by the Microchemical Facility at Emory University. The primer sequences are as follows:
Western Blotting
Medial frontal cortex sections with cortical injury were dissected at 72 h after injury as previously described (Pettus et al, 2005) and homogenized in T-per (Pierce, Rockford, IL, USA). Resulting homogenates were centrifuged for 20 mins at 10,000g. A bicinchoninic acid protein assay (Pierce, 23225) was performed to ensure that all samples had equal amounts of protein. Samples consisting of homogenate, dH2O, and sample buffer were prepared, incubated at 90°C for 10 mins, and stored at −80°C.
A portion of 20 μL of each sample containing 30 μg protein was added to individual wells of a 12.5% acrylamide Criterion gel (BioRad, Hercules, CA, USA). Protein standard (15 μL; Bio-Rad) was loaded into the first well, and 1 μL of MagicMark XP Western Standard (Invitrogen) was loaded into the last well. The gel was run at 200 V for 1 h. Gels were rinsed in transfer buffer for 10 mins. Proteins were transferred to a polyvinylidene difluoride membrane at 100 V for 30 mins. Ponceau S was added to membranes to show protein bands. The membranes were rinsed several times with dH2O to remove excess Ponceau S. Membranes were incubated overnight at 4°C in KPL blocker (KPL, Gaithersburg, MD, USA).
Blots were incubated with a polyclonal goat or rabbit primary antibody for tPA (Santa Cruz Biotechnology, Santa Cruz, CA, USA; sc-5241), thrombin (sc-23348), neuroserpin (sc-32947), cFXIII (sc-18012), and fibrinogen (sc-18026) in KPL diluent to phosphate-buffered saline 1:20) and left overnight on a nutating mixer at 4°C. Membranes were rinsed in phosphate-buffered saline/Tween and incubated with secondary antibody donkey anti-goat IgG-HRP in KPL diluent (1:2,000) for 2 h at room temperature. Membranes were rinsed thrice in phosphate-buffered saline/Tween and then incubated in chemiluminescent substrate (Pierce) for 5 mins. Chemiluminescent bands were detected on a Kodak Image Station 440CF scanner (Rochester, NY, USA) and analyzed with the accompanying densitometric image analysis software. Band density was compared among treatment groups run on the same blots and normalized with a β-actin loading control.
Systemic Coagulation
As noted above, 16 additional rats were used for systemic coagulation parameters. The groups were identical (PROG, ALLO, vehicle, and sham;
Statistical Analysis
All results were expressed as the mean±s.e.m. Statistical significance was set at
Results
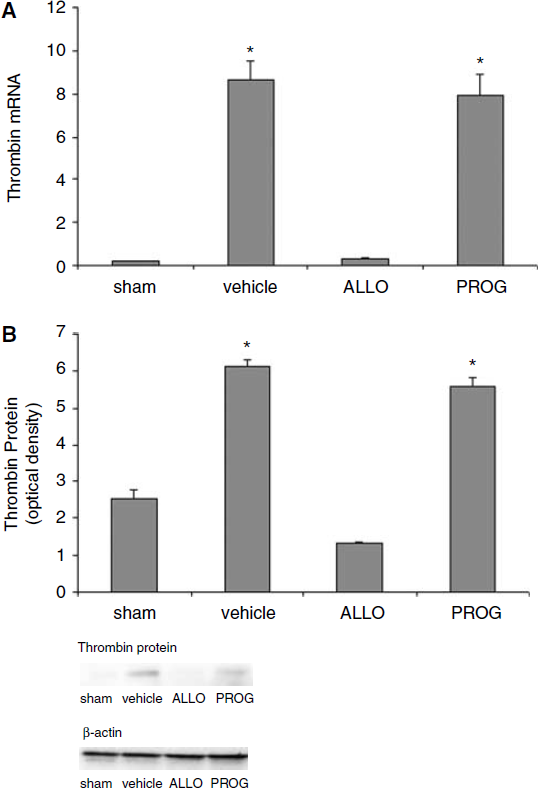
Compared with Progesterone- and Vehicle-Treated Animals, Allopregnanolone Decreases the Expression of Thrombin after Traumatic Brain Injury
Gene expression analysis using real-time PCR showed that thrombin expression was significantly different among the groups (F3,12 = 49.170;
(
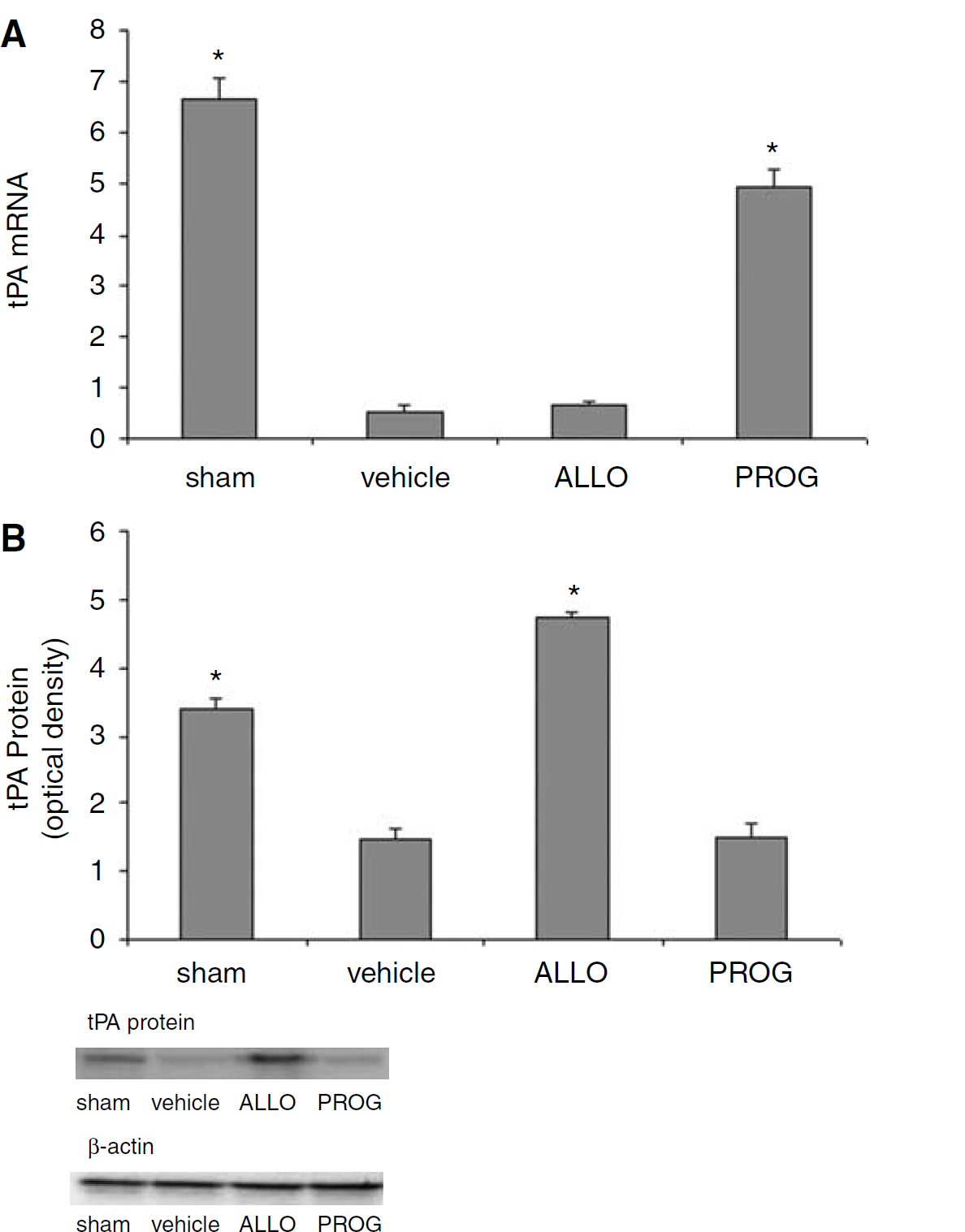
Allopregnanolone Increases the Levels of tPA Protein, but not mRNA, whereas Progesterone Increases tPA mRNA but not Protein
At 48 h after TBI, there were significant differences among the groups with respect to gene expression of tPA (F3,12 = 117.751;
(
Progesterone and Allopregnanolone Increase the Level of Neuroserpin, a tPA Inhibitor
Analyses of free neuroserpin protein levels revealed differences among the groups at 72 h after injury (F3,8 = 130.326;
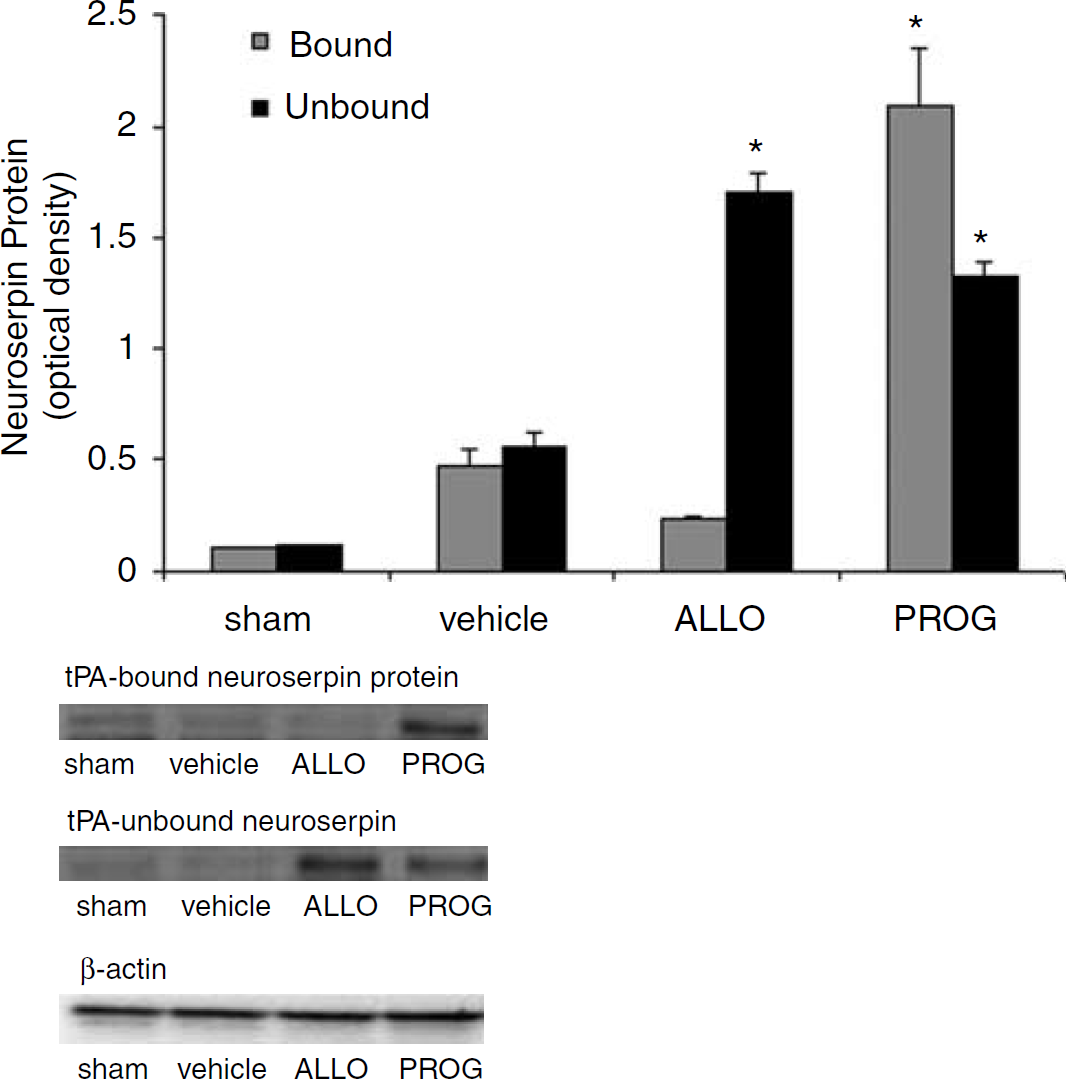
Immunoblotting of free (unbound) neuroserpin protein compared with tPA-bound neuroserpin 72 h after brain injury. Progesterone (PROG) and allopregnanolone (ALLO) significantly increased total (bound and unbound) protein expression of neuroserpin compared with vehicle (22.5% cyclodextrin) and shams. Progesterone significantly increased the level of tPA-bound neuroserpin compared with all other groups. There were no differences between vehicle and shams (*
Given that the protein component of neuroserpin is what blocks the functionality of tPA, studies were not performed to measure mRNA levels.
Allopregnanolone Reduces Fibrinogen Levels after Traumatic Brain Injury
At 72 h after TBI there were injury-induced differences in the level of fibrinogen protein fragments 93 kDa (F3,12 = 181.166;
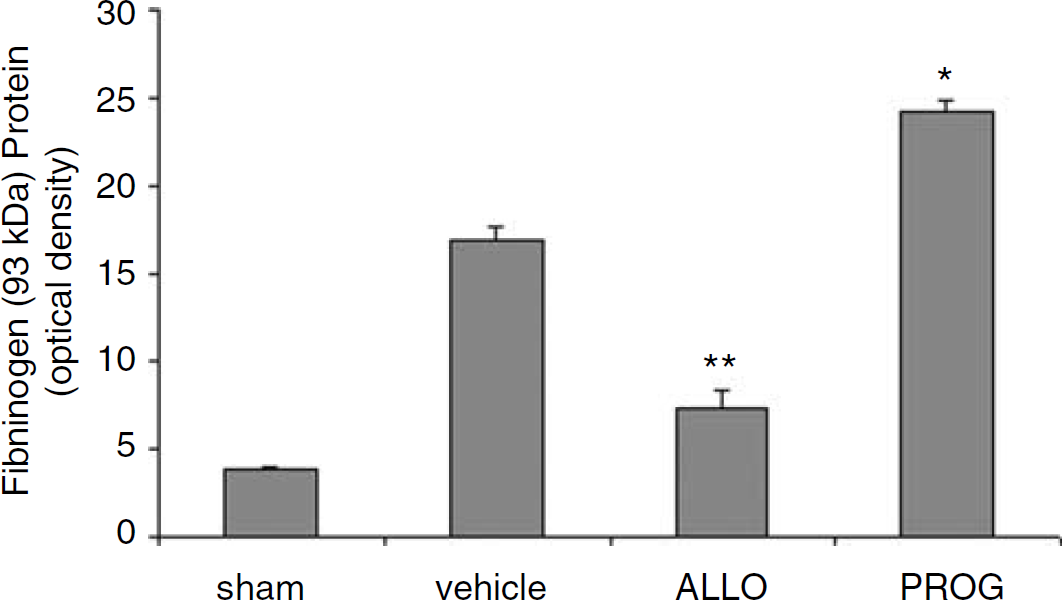
Immunoblotting of fibrinogen (93 kDa fragment) 72 h after brain injury Progesterone (PROG) treatment significantly increased fibrinogen (93 kDa fragment) protein expression compared with all other groups. Allopregnanolone (ALLO) significantly reduced the expression of fibrinogen compared with vehicle- and PROG-treated groups (*increase at
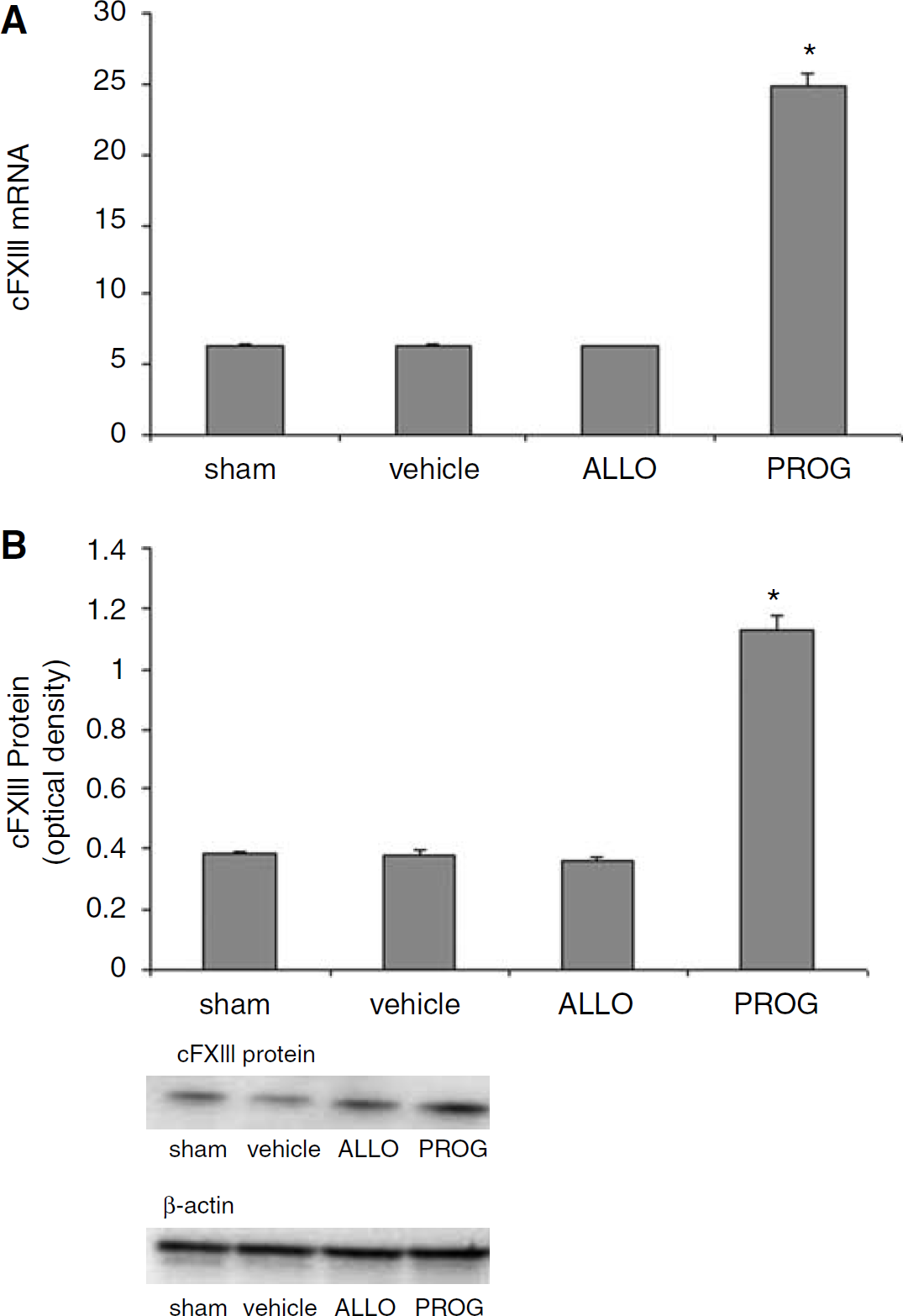
Progesterone Significantly Increases cFXIII Protein Expression
At 48 h after injury PCR analysis of cFXIII gene expression showed that there were differences among the treatment groups (F3,12 = 431.063;
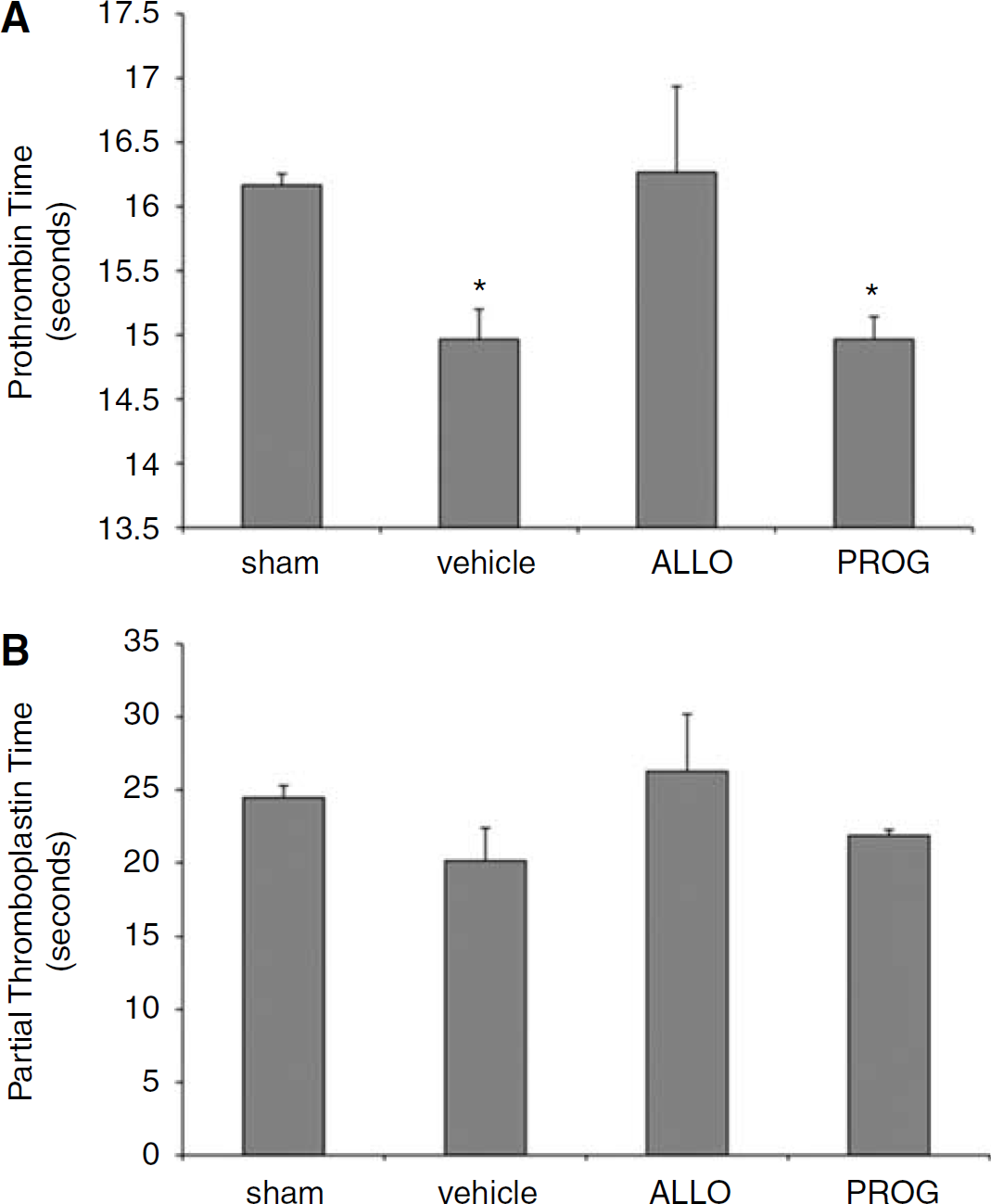
Compared with Progesterone and Vehicle-Treated Animals, Allopregnanolone Significantly Decreases Systemic Coagulation after Traumatic Brain Injury
Prothrombin time was significantly increased in animals treated with ALLO (F3,12 = 5.364,
Discussion
Both PROG and ALLO have been used as protective treatments in a variety of neurologic disease processes including TBI (Shear et al, 2002; Goss et al, 2003; He et al, 2004; Djebaili et al, 2005; Cutler et al, 2005; Hoffman et al, 2006; Schumacher et al, 2007b; Wright et al, 2007), stroke (Gibson and Murphy, 2004; Sayeed et al, 2006), epilepsy (Reddy, 2004; Herzog, 2008), and Niemann-Pick C disease (Langmade et al, 2006). Traumatic brain injury is characterized by primary mechanical injury followed by second-ary neuronal cell death caused by increased cerebral edema (Duvdevani et al, 1995), inflammation (Pettus et al, 2005), and oxidative stress (Tavazzi et al, 2005). Neurosteroids including PROG and ALLO have previously been shown to reduce both vasogenic and cytotoxic brain edema (Galani et al, 2001; O' Connor et al, 2005) while simultaneously redu-cing the molecular components of the inflammatory cascade (He et al, 2004; Pettus et al, 2005).
Cerebral hemorrhaging is a major impediment to recovery from head trauma and hemorrhagic stroke (Stein et al, 2002). As the major coagulopathy after brain injury is caused by the depletion of clotting factors, it is reasonable to assume that some increased expression of coagulation factors after TBI would be beneficial in attenuating injury. Our results indicate that PROG-treated animals show precisely this compared with vehicle-treated injured animals. In contrast, ALLO tends to reduce levels of coagulation proteins compared with vehicle. We therefore speculate that ALLO may not be as beneficial in the treatment of TBI, but may be useful when there is a general systemic hypercoagulable state, as in cases of thrombo-occlusive or ischemic stroke.
Systemic and Brain Coagulation after Traumatic Brain Injury
Our results show that PROG and ALLO differentially affect systemic hemostatic parameters such as PT and PTT after TBI, with ALLO significantly increasing PT. Although clotting time provides an indication of what might be happening in the damaged brain, these systemic clotting tests do not provide direct information about the presence of clotting factors in the area local to the injury. As there is also evidence that routine coagulation parameters (such as PT and PTT) may be inadequate in determining the extent of clinical coagulopathy (Schreiber, 2005; Stein and Smith, 2004; Stein et al, 2004), we focused on key coagulation cascade proteins measured in the penumbral area of the injury as the most reliable assessment of the hemostatic environment in the brain after TBI.
Neurosteroid Regulation of tPA after Traumatic Brain Injury
The management of hemorrhagic brain injury requires the maintenance of clotting factors and the ability to support existing clots. Among its actions in the mammalian brain, tPA destroys clots through the activation of plasmin (Sheehan and Tsirka, 2005). We suggest that hemorrhagic brain injury may benefit from lower levels of endogenous tPA, at least in the acute stage of the injury cascade. With thrombotic stroke, in contrast, a clot impedes blood flow and can enlarge the size of the resulting infarct. Given in time, tPA treatment can have some benefit for stroke management by acting as a ‘clot-buster’ (Melchor and Strickland, 2005). But the picture in the central nervous system (CNS) is not as clear-cut, and a number of studies have shown that tPA can lead to increased cell death after stroke, and inhibiting its actions by gene knockout or serine protease inhibitors, such as neuroserpin, has led to improved results (Yepes and Lawrence, 2004; Miranda and Lomas, 2006).
In this experiment, we found that although injury caused a significant reduction in tPA mRNA levels compared with shams, rats given PROG had significantly higher tPA mRNA levels than injured rats given ALLO (Figure 2A). This difference in gene expression was reversed, however, when we looked at tPA protein, in which case ALLO-treated animals showed significantly higher levels than uninjured shams and animals treated with PROG or vehicle. It is not surprising that PROG sustains tPA mRNA abundance at close to sham levels, given that the tPA gene promoter has an upstream enhancer sequence that is activated by the PROG receptor (Bulens et al, 1997). Although PROG treatment may prevent the injury-induced decline in tPA gene transcription, it does not appear to reproduce these effects at the level of protein expression in our experiments (see Figure 2B) and therefore is not likely to enhance the functional activity of tPA in the injured brain. In contrast, ALLO does increase tPA protein in the time frame we studied, and thus may exert classical anticlotting effects in the injured brain.
Neurosteroid Regulation of the tPA Inhibitor Neuroserpin after Traumatic Brain Injury: Potential Neuroprotective Effects
Neuroserpin is a serine protease inhibitor (serpin) that is released from neurons and inhibits tPA (Yepes and Lawrence, 2004; Miranda and Lomas, 2006). It has been shown to be neuroprotective in several animal models of stroke (Yepes and Lawrence, 2004). Our findings show that neuroserpin is increased by both PROG and ALLO treatment. Although both steroids increase the levels of neuroserpin, PROG increased the ratio of neuroserpin bound to tPA, whereas ALLO led to an increased level of free tPA, pushing the balance toward anticoagulation (Figure 3). As not all effects of tPA in CNS are plasmin mediated, it is possible that although free tPA is elevated in ALLO-treated animals, the simultaneously increased levels of neuroserpin may act to neutralize its neurotoxic effects. Progesterone causes even higher levels of neuroserpin, bound and unbound, indicating that the specific effects of PROG on tPA and the clotting cascade are generally procoagulatory while at the same time strongly inducing neuroserpin-mediated protection.
Neurosteroid Regulation of Coagulation after Traumatic Brain Injury
Thrombin (activated Factor II) cleaves fibrinogen to fibrin, which then crosslinks to form the clot that prevents blood loss after hemorrhagic injury (Mosesson, 1992). In the current study, treatment with PROG had no effect on thrombin compared with vehicle, in terms of both gene expression and protein levels. The observed increase in thrombin as a result of injury is expected, because in addition to its key role in hemostasis, thrombin is important for the recovery process in CNS, where it is neuroprotective in some injury models (Striggow et al, 2000).
Progesterone had effects on other coagulant proteins that contribute to its effectiveness in reducing damage after TBI. We observed an increase in the 93-kDa fibrin fragment, which is characteristic of the fibrin D monomer, formed by the cleavage of fibrinogen by plasmin (Williams et al, 1981). Although fibrinogen cleavage by thrombin leads to fragments that are able to crosslink and make clots, the presence of the D monomer interferes with clot formation (Williams et al, 1981). In this context, the significant increase of the D monomer without the detection of the full-length protein or D-dimer (the plasmin breakdown product of crosslinked fibrin clots) suggests that there is increased fibrinogen expression but also increased proteolytic activity, leading to potentially reduced clotting. At 72 h, this may be beneficial in cases of TBI, as it may reduce the potential for the formation of intravascular microthrombosis (Stein et al, 2004).
Progesterone also significantly increased levels of cFXIII, which is a key component in stabilizing fibrin. In the absence of D-dimer breakdown products, elevated cFXIII levels suggest an increased potential for coagulation rather than increased coagulation itself. This may be especially important in human polytrauma patients, the most severely injured of whom are hypocoagulable and at risk for the lethal triad of acidosis, hypothermia, and coagulopathy in the 72-h postinjury period (Schreiber, 2005). cFXIII has also been shown to be neuroprotective in CNS (Monsonego et al, 1998).
Allopregnanolone reduced the protein expression of thrombin compared with shams and the vehicle-injured group. As the same reduction is observed at the mRNA level, this anticoagulant activity appears to be regulated at the gene level. Although decreased fibrin D monomer in ALLO-treated animals may indicate reduced plasmin activity, in light of the tPA results above, it more likely indicates a reduction in fibrinogen. Along with increased levels of cFXIII induced by PROG but not ALLO, these data collectively suggest that it may be reasonable to select differentially between the hormone and its metabolite when it comes to treating traumatic versus thrombotic injury to the brain. Although the effects of PROG seem to be more complicated, ALLO appears to have a relatively straightforward anticoagulant effect. This is consistent with our PT and PTT data on systemic coagulation.
Our previous studies have shown that neurosteroids reduce brain edema, inflammation, and oxidative stress (Galani et al, 2001; Djebaili et al, 2005; Pettus et al, 2005). The findings presented here show that after TBI, coagulation mechanisms at both the gene and protein level are not the same for PROG and ALLO. Although our experiments in laboratory rats may not yet translate directly to patients, we can speculate that PROG may be better for treatment of TBI, where bleeding may not be completely stopped during the first hours or days after the insult. We also suggest that the administration of ALLO might be a more appropriate treatment for cases of thrombotic stroke, where there is already a systemic tendency toward increased coagulation and further clotting can cause additional damage. Although PROG converts to ALLO in the brain, the extent to which this reaction occurs before PROG itself can act at various sites in the damaged brain is not known. There is also evidence suggesting that ALLO metabolism is bidirectional and that it can revert to PROG in CNS, suggesting a number of interactive mechanisms that were not studied in this experiment and are not well characterized in the literature on the neuroprotective effects of these hormones (Schumacher et al, 2007a). We hope that by further clarifying the actions of neurosteroids on the coagulation cascade and clotting time, as well as on the enhanced expression of trophic repair factors in the damaged brain, we can improve the design of safe and effective clinical trials for the treatment of brain injury in both stroke and mechanical trauma. An important concept to take away is that neurosteroids do not appear to have simple linear actions
Footnotes
Acknowledgements
We thank Chheng-Orn Evans and Dr Nelson Oyesiku for their contributions to our gene expression data. We also thank the people in the Microchemical Facility at Emory University for assistance in generating the primers used in our real-time PCR experiments. Furthermore, we thank Leslie McCann and Kate I Ross for their assistance and patience in editing this article.
DGS and SWH have applied for patent protection for progesterone in the treatment of central nervous system injury and as such may benefit financially as a result of the outcomes of this research or work reported in this publication.