
Abstract
After complete cerebral ischemia, the postischemic blood flow response to functional activation is severely attenuated for several hours. However, little is known about the spatial and temporal extent of the blood flow response in the acute postischemic period after incomplete cerebral ischemia. To investigate the relative cerebral blood flow (rCBF) response in the somatosensory cortex of rat to controlled vibrissae stimulation after transient incomplete ischemia (15-min bilateral common carotid artery occlusion + hypotension), we employed laser speckle imaging combined with statistical parametric mapping. We found that the ischemic insult had a significant impact on the baseline blood flow (
Keywords
Introduction
There has been considerable interest in the ability of the cerebrovasculature to respond to functional stimulation after a period of transient cerebral ischemia (Schmitz et al, 1997, 1998; Ueki et al, 1988; Ances et al, 2000; Dijkhuizen et al, 2003), which may provide a window into the eventual fate of the tissue. Better characterization of these responses after ischemia could also be important for interpreting studies of functional reorganization after ischemic injury. After cardiac arrest, during which cerebral blood flow (CBF) is reduced to zero, magnetic resonance (MR)-based perfusion imaging shows a lack of hemodynamic response to electrical forepaw stimulation 1 h after resuscitation, and only a minimal response after 3 h (Schmitz et al, 1998). During the first 24 h of reperfusion, MR-based signals of functional recovery return, with the perfusion-weighted response to stimulation recovering more slowly than does the blood oxygen level-dependent measurement. If both vertebral and carotid arteries are occluded for 30 mins, also producing negligible blood flow in the somatosensory cortex, the tissue loses its ability to respond to electrical forepaw stimulation even after 3 h of recirculation (Ueki et al, 1988). There are significant differences, however, between complete ischemia (no blood flow) and severe incomplete ischemia (CBF less than 10% of normal) (Benzi et al, 1978; Dietrich et al, 1987; Steen et al, 1979). During incomplete ischemia, such as temporary middle cerebral artery occlusion, hemodynamic response in the somatosensory cortex to electrical stimulation of the contralateral forepaw is significantly attenuated 1 day after the occlusion and is not normalized until approximately 2 weeks (Dijkhuizen et al, 2003). There is no information, however, concerning the ability of the cerebrovasculature to respond to functional stimulation very acutely after incomplete ischemia, and, in particular, whether the spatial extent of the activation is altered by the ischemic insult.
Laser speckle imaging (LSI; Briers, 2001; Dunn et al, 2001) provides two-dimensional blood flow maps with high spatial and temporal resolution. The LSI technique shares the same basic physical picture with the laser-Doppler perfusion technique: scattered laser light with different pathlength produces a random interference pattern known as speckle, whose fluctuations contain information about motions of particles in the underlying medium. A variety of methods (Briers, 2001) use this effect for tissue studies, including laser-Doppler flowmetry (Bonner and Nossal, 1990) and diffuse correlation spectroscopy (Boas and Yodh, 1997). Recently, LSI has been widely used to measure CBF during functional stimulation and physiologic perturbation in rodent and cat cortex (Dunn et al, 2001; Durduran et al, 2004; Weber et al, 2004; Ayata et al, 2004; Shin et al, 2006; Strong et al, 2006).
We used LSI to investigate the near-surface activation flow coupling after electrical somatosensory stimulation of forepaw and hindpaw in rat (Durduran et al, 2004). Using high-resolution temporal (5 Hz) and spatial sampling (32 μm), the effects of stimulus amplitude and duration were investigated. Basic functional mapping was shown by separating the activation after forepaw and hindpaw stimulation, and correlation coefficient images were used to characterize the spatial extent of the activation. However, the regions of interest (ROIs) were determined from the rescaled correlation coefficient images by setting an arbitrary threshold or by using a full-width at half-maximum approach (Durduran et al, 2004; Weber et al, 2004; Dunn et al, 2005). This makes it difficult to compare the activation areas under different physiologic conditions, such as after cerebral ischemia, as the maximum may also be a variable. Conversely, statistical parametric mapping (SPM), which is widely used in the functional MRI community (Friston et al, 1995; Worsley and Friston, 1995), enables statistical comparison and interpretation of activation under various physiologic conditions. To this end, a modified general linear model (GLM) (Worsley and Friston, 1995) was employed to construct robust statistical parametric maps for spatially extended processes in the presence of temporal autocorrelation. We used the SPM approach with LSI data to examine the relative cerebral blood flow (rCBF) response in the somatosensory cortex of rat to controlled vibrissae stimulation after temporary incomplete ischemia. We found that the activation area and temporal response to stimulation were altered acutely after severe incomplete cerebral ischemia, whereas the maximum CBF response to functional stimulation was preserved.
Materials and methods
Surgical Preparation
Animal procedures were in accordance with the guidelines established by the National Institutes of Health and were approved by the Institutional Animal Care and Use Committee at the University of Pennsylvania. Studies were undertaken in 10 male Sprague—Dawley rats (
Transient forebrain ischemia was produced by bilateral carotid arterial occlusion (2VO) with controlled hypotension (Nordström and Siesjö, 1978; Smith et al, 1984). Loose snares were placed around both carotid arteries and mean arterial blood pressure was lowered to 45 to 50 mm Hg by slowly withdrawing blood from the femoral arterial catheter into a heparinized syringe. The snares were then tightened and the mean arterial blood pressure was maintained at this level for 15 mins, at which time the snares were removed and the withdrawn blood was returned to the animal over a period of 5 mins.
A group of control rats were prepared similar to the animals with transient forebrain ischemia, except that the carotid artery snares were not tightened and blood was not withdrawn from the arterial catheter (
Stimulus Presentation and Experiment Protocol
The experiment protocol consisted of 20 secs of image acquisition. After a 5-sec data collection (no stimulus) procedure, the vibrissae were stimulated for 3 secs; data were taken poststimulus for 12 secs. Stimulation consisted of mechanical stroking of the left vibrissa (B1–3, C1–3, and D1–3) with a solenoid driven in the rostral—caudal direction at 5 Hz. This protocol was repeated 10 times with 40 secs of no data acquisition (or stimulation) between runs. Thus, the vibrissae were stimulated for only 3 secs/min. Vibrissae stimulations (and LSI data acquisitions) were performed before ischemia and at 20 mins, 30 mins, 1 h, 2 h, and 3 h after reperfusion. Animals were killed after the 3 h measurement with an overdose of a barbiturate (150 mg/kg) and the brain removed from the skull. The cortices were carefully removed from the remainder of the brain, flattened between two silicone-coated glass slides separated by 4 mm spacers, and frozen in isopentane cooled to −30°C. The right cortex was mounted in a cryostat (Bright Instrument Company Ltd, Huntingdon, England) and, after temperature equilibration, was sectioned tangential to the cortical surface. Sequential sections were stained for cytochrome oxidase, as described previously (Sohn et al, 1999). Images from the cytochrome oxidase staining, which map the walls of the vibrissae barrels, were coregistered with the LSI images using a warping technique described by Bookstein (1989).
Laser Speckle Imaging
The basics of the LSI technique have been described in detail earlier (Goodman, 1985; Briers, 2001; Dunn et al, 2001; Bandyopadhyay et al, 2005). Briefly, when coherent laser light is shone on a turbid medium, such as biologic tissue, photons traveling from different scattering paths form random speckle patterns on the surface of the medium, which can be captured by a CCD (charge-coupled device) camera. The intensity of each speckle fluctuates if the scattering particles are in motion inside the tissue. Within a given exposure time, speckle visibility of the region with faster particle movements is lower than the region with slower particle movements, because of stronger blurring of the speckle patterns. The speckle visibility at each position can be quantified as speckle contrast (

where
The LSI device and scanning procedure used in this study have been described in detail earlier (Durduran et al, 2004). A collimated diode laser (Hitachi, HL 785 1G, 785 nm, 50 mW; Thorlabs, Newton, NJ, USA) was used to illuminate the cerebral cortex through the thinned window on the skull at 30 to 40° from vertical. A 60 mm lens (AF Micro-Nikkor 60 mm f/2.8D; Nikon, NY, USA) was used for the imaging and the aperture was adjusted to match the speckle size to the CCD pixel dimensions (6.45 μm × 6.45 μm) (Dunn et al, 2001; Durduran et al, 2004). Thus, β was assumed to be unity in the following calculations. Images were recorded at 5 Hz with a cooled CCD camera (Retiga 1350EX, QImaging, Surrey, BC, Canada) using commercial imaging software (StreamPix, NorPix, Montreal, QC, Canada). Both the camera and the mechanical stimulator were externally triggered for the coregistration of stimulation and data acquisition.
Equation (1) was used to extract 1/τc from the speckle contrast on each pixel as the index for CBF values. We have noticed that 1/τc is not zero when tissue perfusion is zero (post mortem), an observation also made by other laboratories (Ayata et al, 2004; Strong et al, 2006). This so-called ‘biological zero’ mainly corresponds to the random motion of scatterers in the tissue and is extensively discussed in the laser-Doppler literature (Kernick et al, 1999). In a separate group of animals without ischemic insults (
To reduce the data to be processed to a manageable size, the images were smoothed using a bi-cubic interpolation method by 5 times 5, thereby reducing the spatial resolution to 32.25 μm. Relative changes in CBF because of vibrissal stimulation (rCBF) were obtained by dividing each image by the average baseline image obtained during the 5 secs before the start of the stimulus. The data collected during the repeat stimulations were collapsed by aligning time points and calculating the mean of the images. Changes in blood flow during the ischemic and reperfusion periods were calculated by dividing each image by the average of images obtained before the onset of ischemia.
Data Analysis
A modified GLM (Worsley and Friston, 1995) was employed to estimate the spatial extent of the activation using a free software package VoxBo (http://www.voxbo.org). Basically, the GLM treats a series of measurement data

where the columns of the design matrix (
In our study, the rCBF images from individual animals were spatially smoothed with a 5 times 5 pixel spatial Gaussian filter before they were imported into Voxbo. Covariates of interest represent the contrast of activity at each second after the onset of stimulation (up to 7 secs), and covariates of no interest were defined as the intercept of each trial. Statistical parametric maps (
To investigate the spatio-temporal response simultaneously, an ROI was defined independently at each time point (before and after the ischemic insult) for each animal as all pixels with
Results from the ischemic and control groups were expressed as mean ± s.e.m. Significant differences between pre- and postischemia were determined with one-way repeated measures ANOVA. When significant differences were found, the Tukey test was used to find at which time point these differences occurred.
Results
Physiologic Variables
The blood gases in the ischemic animals were all within the normal range (PaCO2: 42.7 ± 1.8 mm Hg; PaO2: 109 ± 4 mm Hg; pH: 7.39 ± 0.02) and were not significantly different during the ischemic and reperfusion periods. The mean arterial blood pressure was 118 ± 3 mm Hg before the generation of hypotension and was reduced to 47.6 ± 1.2 mm Hg during the bleeding phase. After release of the ligatures around the carotid arteries and reinfusion of the shed blood, blood pressure increased to 122 ± 3 mm Hg (Figure 1). The blood gases (PaCO2: 37.7 ± 1.1 mm Hg; PaO2: 118 ± 7 mm Hg; pH: 7.43 ± 0.02) and blood pressures (117 ± 4 mm Hg) in the control group were very similar to the ischemic animals and did not differ significantly during the course of the study.
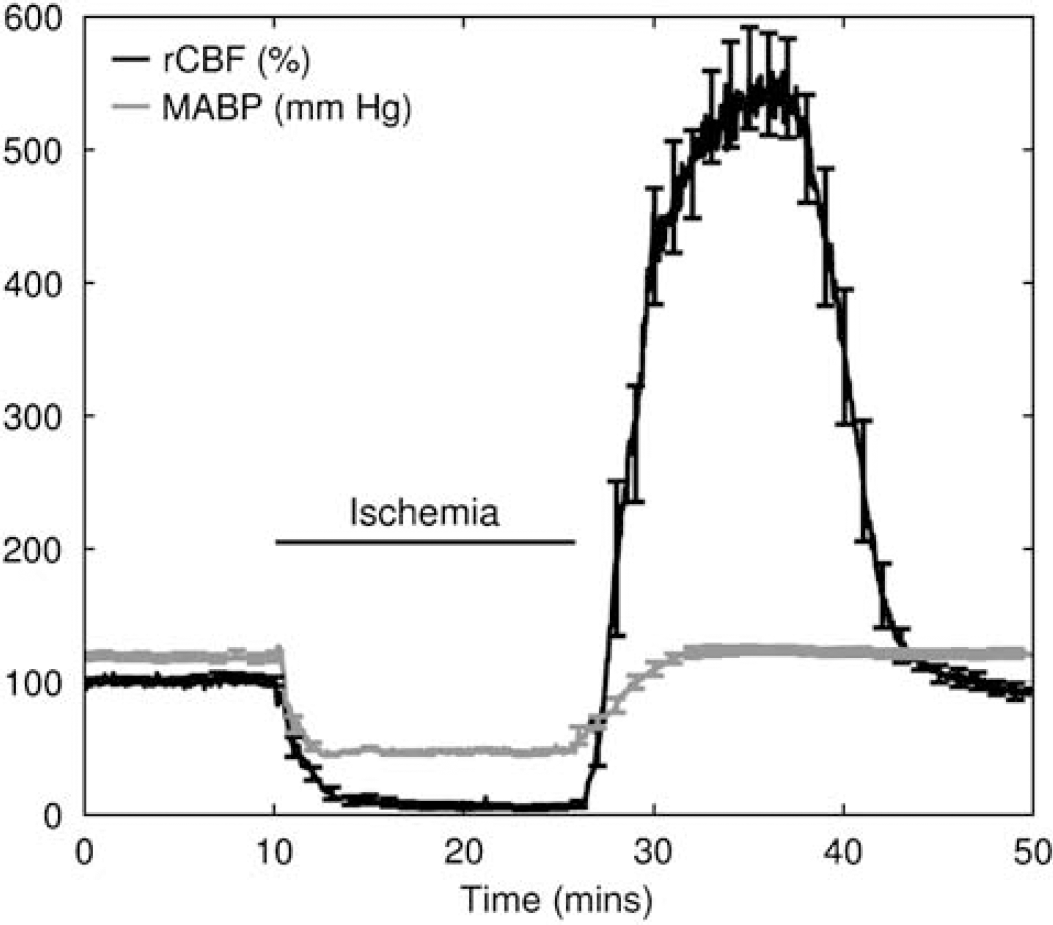
Average relative cerebral blood flow (rCBF) and mean arterial blood pressure (MABP) measured during incomplete ischemia (
Cerebral Blood Flow During Ischemia
When the carotid arteries were ligated and the arterial blood pressure decreased, rCBF in the middle cerebral artery territory decreased rapidly to 6.6% ± 1.8% (
Baseline Cerebral Blood Flow Variations because of Severe Incomplete Ischemia
The ischemic insult was found to have a significant effect on the baseline CBF (ANOVA,
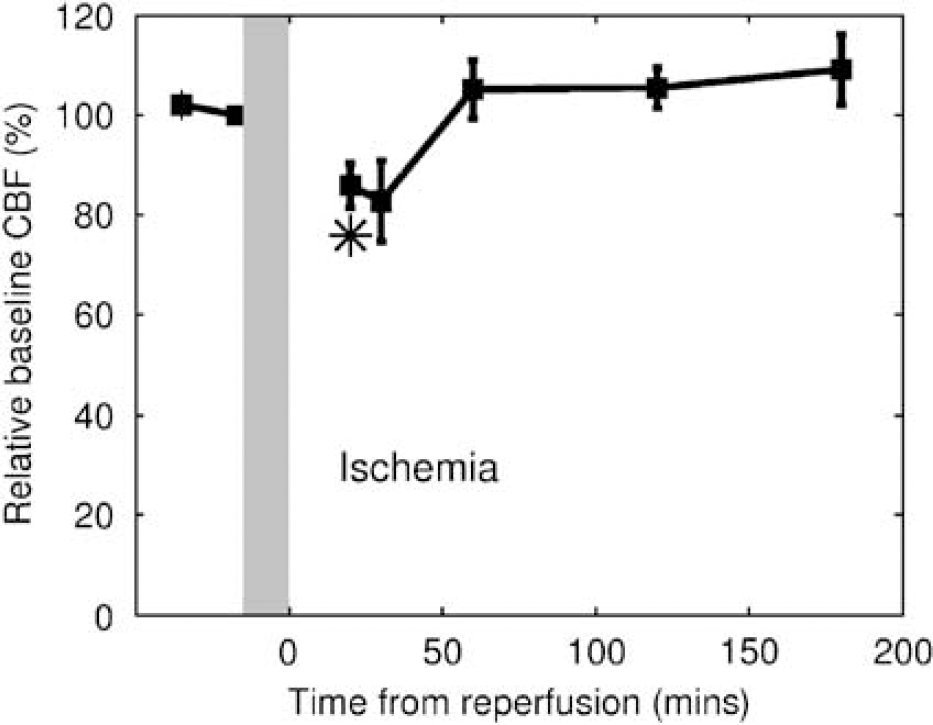
Baseline cerebral blood flow (CBF) changes before and after ischemic insults. Symbols indicate significant difference from preischemic values (
Functional Responses After Ischemic Insult
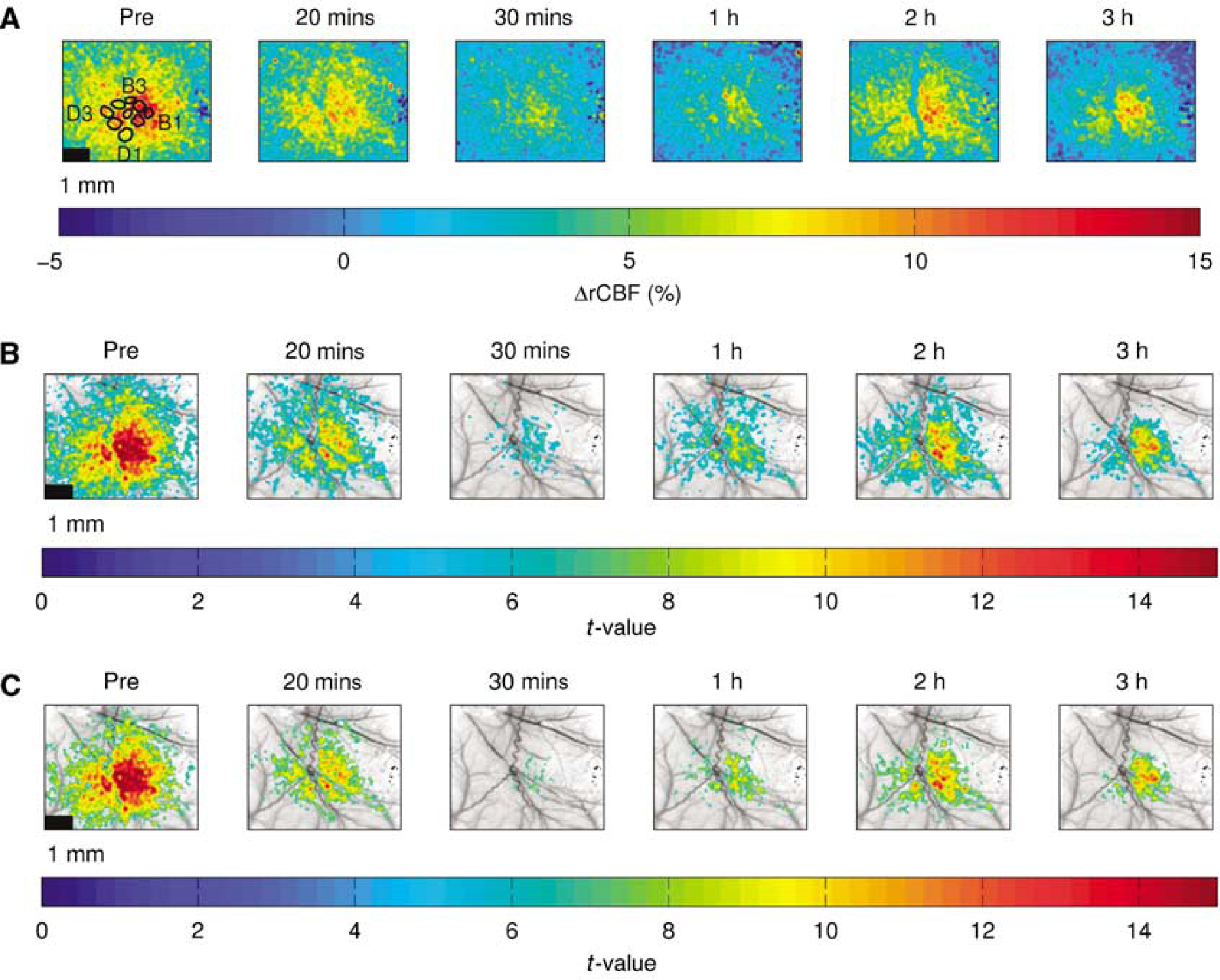
Images from a representative animal showing functional activations before and after ischemic insult. (
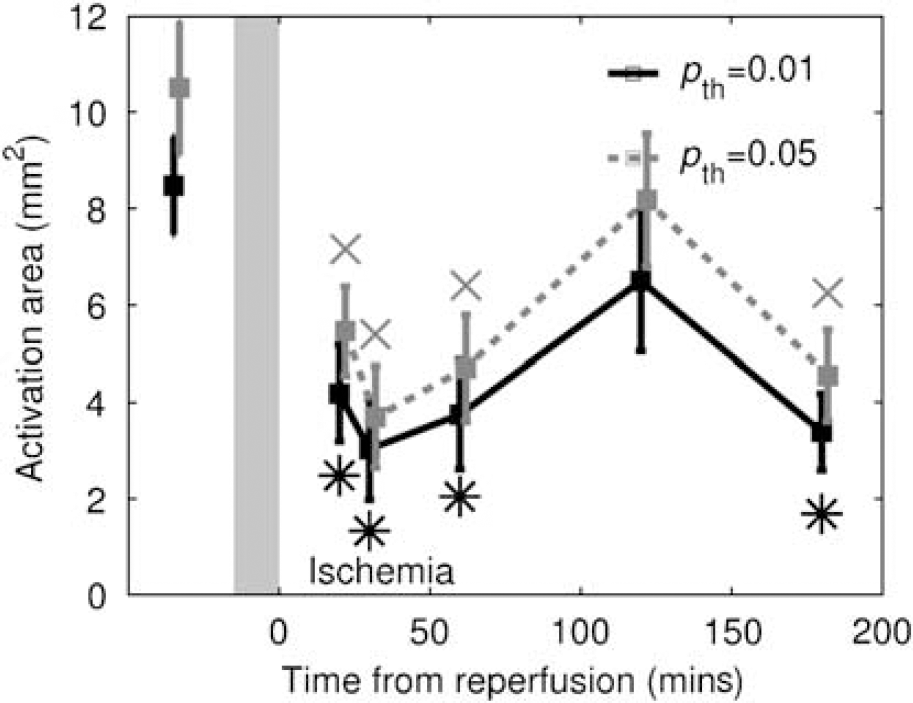
Activation area before and after ischemic insult (
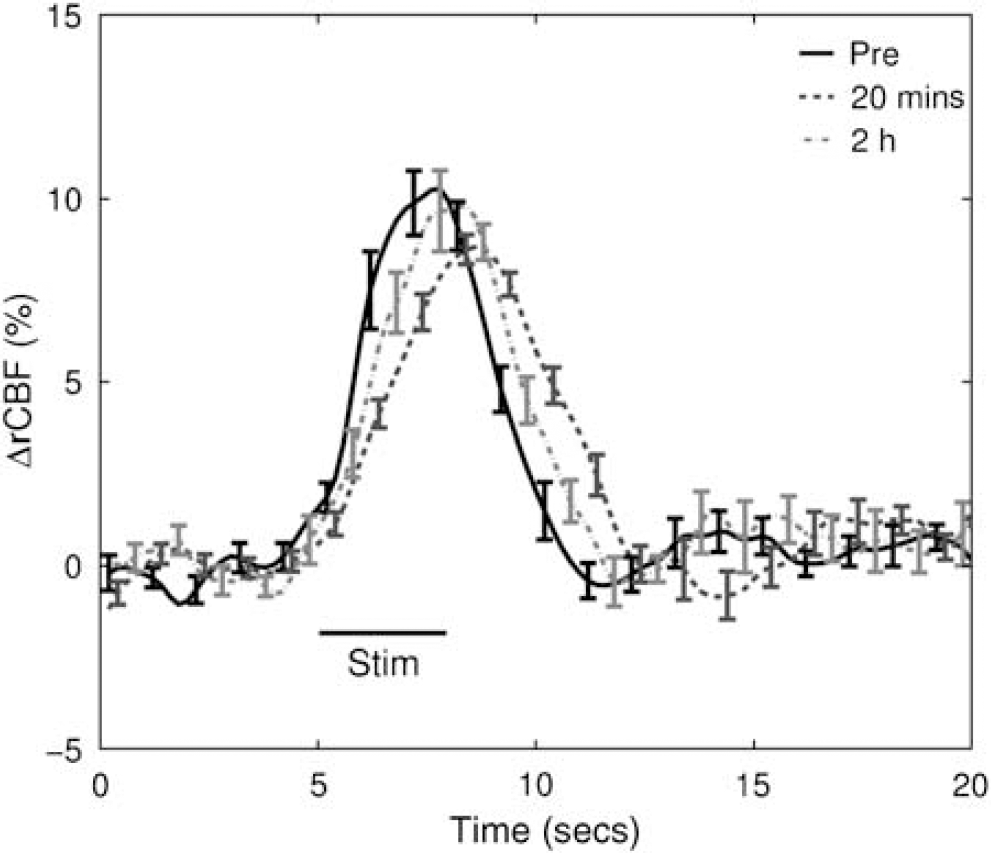
Average ΔrCBF curves in response to stimulation before and after ischemic insult from all animals (
(
In the control group, the activation area was 7.3 ± 0.9 mm2, which neither changed significantly during the course of the various scans (
Discussion
The phenomenon of hypoperfusion and postischemic hyperperfusion has been investigated extensively after severe incomplete ischemia in rat (Kagstrom et al, 1983; Inamura et al, 1988; Dirnagl et al, 1993). Cerebral blood flow measured in the cortex was found to be less than 10% of the preischemic level after 10 to 15 mins of incomplete ischemia (Kagstrom et al, 1983; Inamura et al, 1988; Dirnagl et al, 1993), which is in agreement with our observations. After 5 mins reperfusion, a 250% to 300% hyperemia was usually seen (Kagstrom et al, 1983; Dirnagl et al, 1993), which is lower than the peak value observed 9 to 10 mins after the end of the ischemia in our study (538% ± 35%). These differences might be related to differences in anesthesia or duration of ischemia between the studies. Dunn et al (2001) have validated laser speckle against laser Doppler in rat brains over a wide range of rCBF values (from 0% to 250% of baseline). However, to our knowledge, no validation study has been reported at a higher perfusion level. It is possible that laser speckle overestimates blood flow during reperfusion in the current study. Further studies are needed to validate the accuracy of laser speckle technique at high perfusion levels.
It is believed that functional impairment/recovery after stroke depends on the duration and severity of cerebral ischemia. Schmitz et al (1998) have shown in rats with 10 mins of cardiac arrest that blood oxygen level-dependent measurement and perfusion responses to forepaw stimulation were impaired 1 h after the cardiac arrest. Blood oxygen level-dependent measurement eventually recovered at 1 day, but at that time, perfusion only recovered to about 50%. In the same animal model, Schmitz et al (1997) also showed, using laser Doppler and autoradiography, that blood flow response to forepaw stimulation was completely suppressed at 45 mins. In some but not all animals, a weak response could be observed by 1.5 h, followed by a gradual improvement of 50% to 60% of control within 3 days. Using functional MRI, Shen et al (2005) showed that with permanent focal ischemia (middle cerebral artery occlusion), CBF response to the forepaw stimulation in the primary somatosensory cortices was lost, although CO2 reactivity of the vasculature was intact. After transient (15 mins) ischemia, blood flow response to the forepaw stimulation was normalized by 30 mins and remained unaltered throughout the 24 h of monitoring. It should be noted, however, that this model does not produce permanent damage.
These prior studies investigated the impairment/recovery of amplitude in response to functional challenges (CO2, electrical forepaw stimulations, and so on). However, less is known about the spatial and temporal recovery of the brain with transient ischemia in response to functional challenges, because of the limited spatial and temporal resolution of most imaging techniques (MRI and PET). In the current study, we exploited the superior spatial and temporal resolution of LSI to address this question. We also used the SPM approach to analyze our laser speckle data, which enabled the comparison of brain activation under different physiologic conditions. The time period (2 to 5 secs into stimulation) used for contrasting was chosen to cover the peak activations. We also tried contrasting different time periods (i.e., 1 to 5 secs, 2 to 6 secs into stimulation) with baseline. Similar trends were observed for the changes in activation area, maximum ΔrCBF, and time to maximum ΔrCBF. In GLM analyses, the hemodynamic response function can also be modeled in a variety of ways to examine significant changes between conditions (Woolrich et al, 2004), and it would also be possible to test complex models with various contrasts and covariates, including covariates for ischemic states, so as to generate maps showing regions of significant change at different states. These approaches will be explored in future laser speckle studies.
In SPM, variations of resting rCBF within 5 secs before stimulation were taken into account for the statistical analysis. Pixels within ROIs defined by a statistical threshold (e.g.,
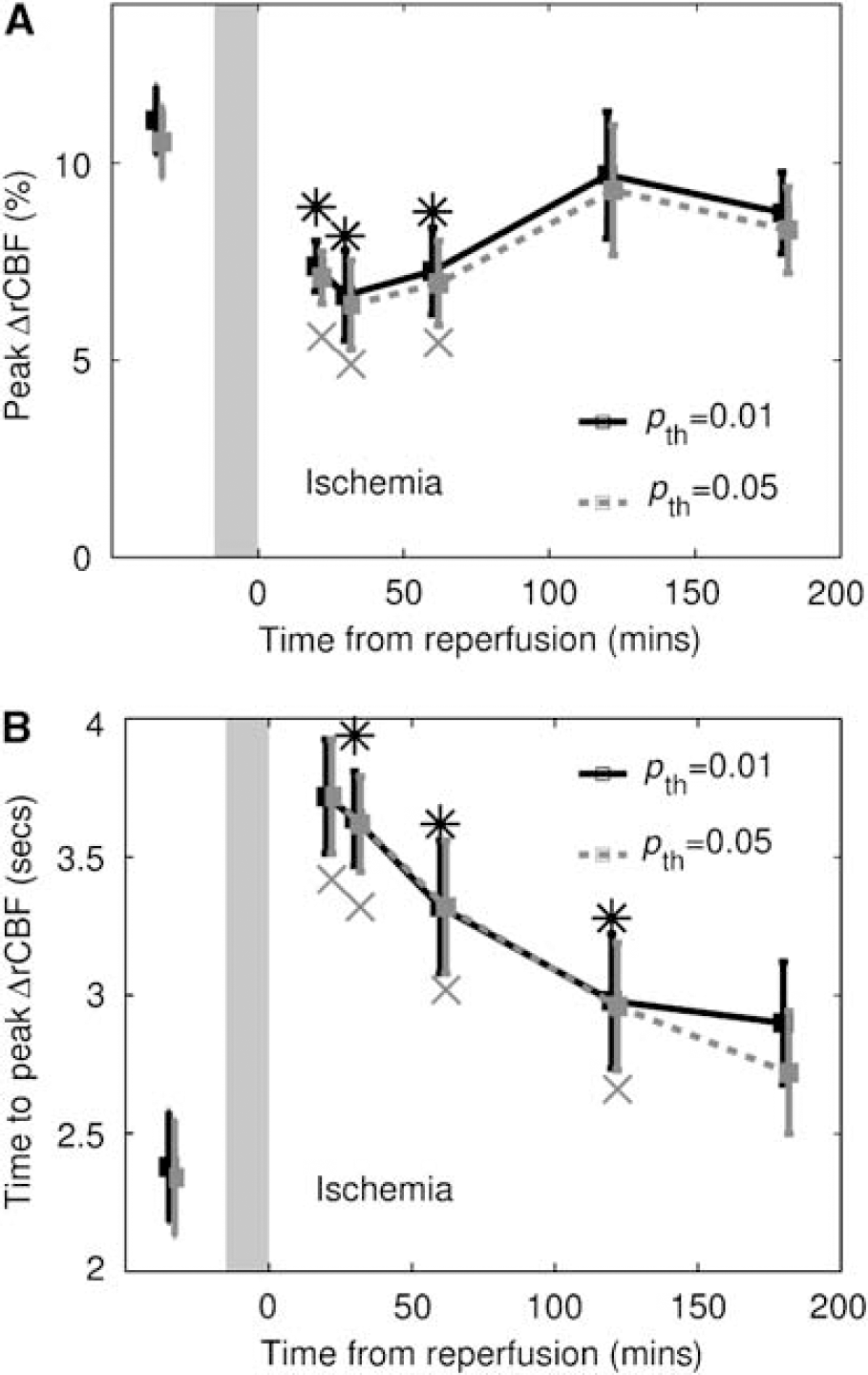
We have employed a variable ROI before and after ischemia for the analysis of ΔrCBF response to vibrissae stimulation. Another approach is to use a fixed ROI determined by SPM before the ischemic insult for analysis at all the time points. In this case, peak ΔrCBF showed a significant decrease after ischemia and subsequently recovered (Figure 7A), although the time to peak ΔrCBF (Figure 7B) followed a trend similar to that observed in Figure 6B. The difference in peak ΔrCBF before and after ischemia was less significant when a variable ROI was used (Figure 6A). Note, however, that the peak ΔrCBF response in Figure 7A followed the same trend as the activation area changes with a variable ROI (Figure 4). The different peak ΔrCBF response between a fixed ROI and a variable ROI is probably because of the inclusion of pixels that are less activated after ischemia. The approach of using a fixed ROI, therefore, cannot separate the ischemia influence on the temporal and spatial response of ΔrCBF.
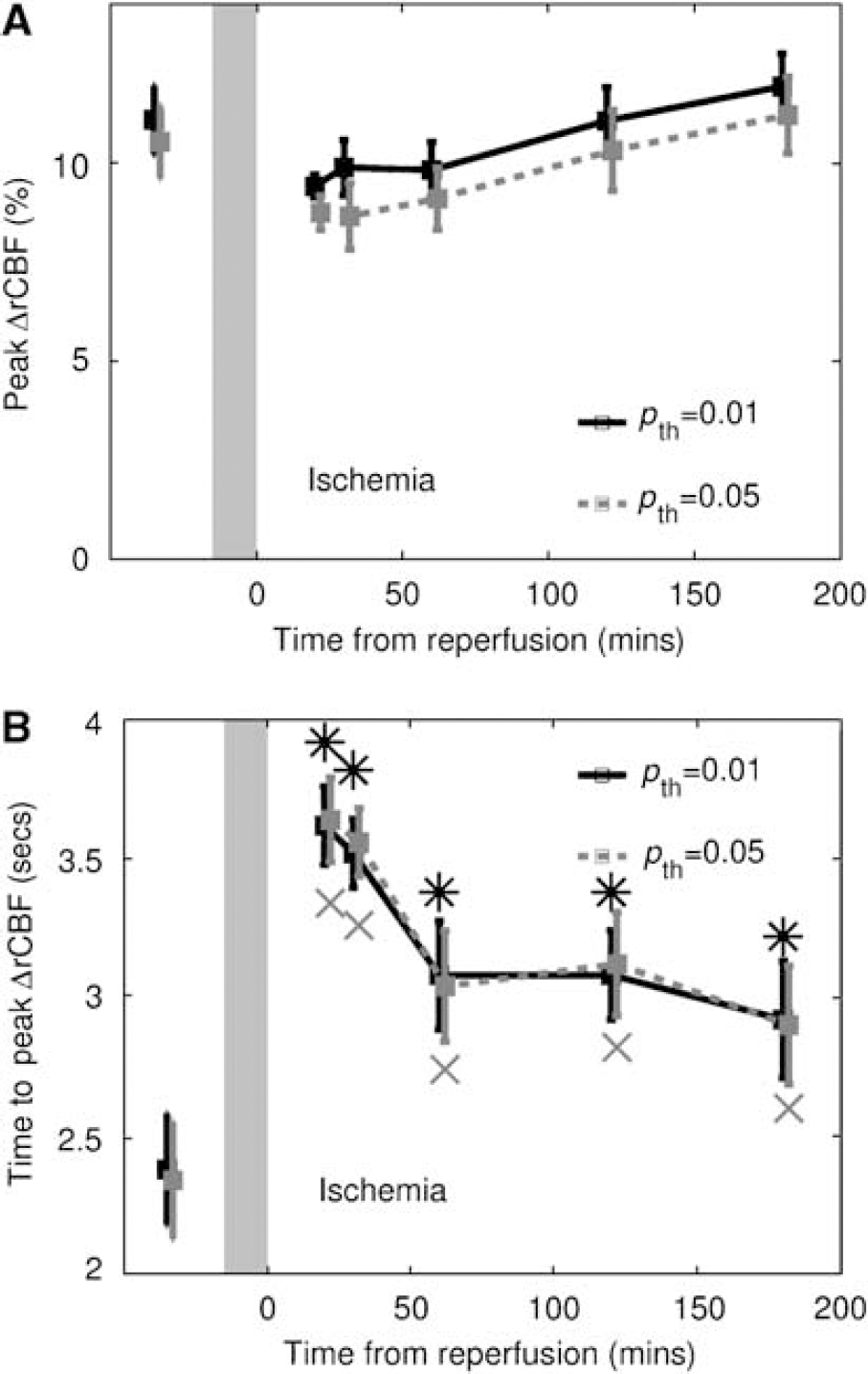
Peak ΔrCBF (
In a nonischemic rat, the spatial extent of hemodynamic changes (oxy, deoxy, and total hemoglobin concentrations and CBF) in response to whisker stimulation is usually larger than the size of the whisker barrels (Devor et al, 2003; Weber et al, 2004; Dunn et al, 2005). In the current study, the activation area observed before ischemia agrees well with the literature, considering that the distance between adjacent whisker barrels is about 400 to 500 μm (Masino et al, 1993), and the CBF response is less localized compared with hemoglobin changes (Dunn et al, 2003) and oxidative metabolism (Weber et al, 2004). One of our principle findings is that the activation area in response to functional stimulation is significantly reduced after the ischemic insult. However, baseline blood flow was found to recover 1 h after the reperfusion, and we observed a sign of recovery in the activation area at the 2 h time point. This phenomenon was quite robust and was consistent among all animals, which may suggest the existence of a window for functional recovery. It should be noted that the principal parameter of measurement in this study was blood flow (obtained with speckle contrast) and that alterations in the hemodynamic response may not be necessarily because of alterations in the ability of the vasculature to respond. There is evidence that evoked responses may be altered early after cerebral ischemia (Schmitz et al, 1997), raising the possibility that the observed changes may not be solely because of changes in activation flow coupling. In a recent study (Burnett et al, 2005), however, CBF measured with laser Doppler was found correlated with the amplitude of the somatosensory evoked potentials during ischemia, suggesting that CBF reflects neural function. Further studies correlating CBF and neural function would be needed to determine the basis for the observed hemodynamic changes.
Another major effect of the ischemic insult was the variations in the temporal profile of rCBF in response to stimulation. Before ischemia, rCBF started increasing about 1 sec after the onset of the stimulation and took 2.4 ± 0.2 secs to peak, in line with the previously observed hemodynamic changes during both forepaw (Ances et al, 2001; Durduran et al, 2004; Dunn et al, 2005) and whisker (Jones et al, 2001; Dunn et al, 2003, 2005; Weber et al, 2004) stimulations in the rat. Note that the temporal profile of the rCBF response was averaged over the whole activation area, with the maximum ΔrCBF response reflecting an average change of the activated region. The peak response of 11.1% ± 0.9% from the nine-whisker stimulation is thus comparable with the results from single-whisker stimulations (Dunn et al, 2003, 2005; Weber et al, 2004), although less than what was seen in layer IV of the cortex using autoradiography (Greenberg et al, 1999). After the ischemic insult, significant delay of the time to peak ΔrCBF was observed and this delay gradually returned toward normal (Figure 6B). It is interesting to note that the peak ΔrCBF was not significantly influenced by the ischemic insult. To the extent that CBF changes reflect underlying neural metabolism, this may suggest that in the early stages of reperfusion, the somatosensory cortex ‘worked as hard as’ before ischemia, but the vasculature responded more slowly to the stimulation. We previously observed a prolonged time to peak after unilateral carotid occlusion and attributed the delay to the use of a circuitous recruitment of collateral supply (Ances et al, 2000). However, in the present study, the carotids were reopened, suggesting that the observed delay may represent an alteration in activation flow coupling after the ischemic insult.
Conclusions
We have incorporated the SPM method into LSI to investigate functional spatial and temporal responses of CBF after temporary incomplete cerebral ischemia in the rat. Modified GLM and SPM offer robust statistical parametric maps and enable the comparison of activation under various physiologic conditions. Our results show that the ischemic insult significantly alters CBF, the area of activation, and the temporal response to stimulation. The magnitude of the CBF response to functional stimulation, however, was preserved in the early hours after transient incomplete ischemic insult.
Footnotes
Acknowledgements
The authors thank Meeri N Kim for useful discussions.