
Abstract
Vasospasm is a major cause of morbidity and mortality after aneurysmal subarachnoid hemorrhage (aSAH). Studies have shown a link between single-nucleotide polymorphisms (SNPs) in the endothelial nitric oxide synthase (eNOS) gene and the incidence of coronary spasm and aneurysms. Alterations in the eNOS T-786 SNP may lead to an increased risk of post-aSAH cerebral vasospasm. In this prospective clinical study, 77 aSAH patients provided genetic material and were followed for the occurrence of vasospasm. In multivariate logistic regression analysis, genotype was the only factor predictive of vasospasm. The odds ratio (OR) for symptomatic vasospasm in patients with one T allele was 3.3 (95% confidence interval (CI): 1.1 to 10.0,
Keywords
Introduction
The estimated annual rate of aneurysmal subarachnoid hemorrhage (aSAH) among European and North American populations ranges from 6 to 8 per 100,000 population (Broderick et al, 1993; Linn et al, 1996). Approximately 30% of survivors remain dependent, and only 30% to 45% return to previous or comparable jobs (Ropper and Zervas, 1984). Following aSAH, a major cause of morbidity and mortality is delayed ischemic neurologic deterioration secondary to cerebral vasospasm (Bendok et al, 1998). Symptomatic vasospasm occurs in 15% to 65% of patients, is detectable in 30% to 70% of patients by angiography, and results in infarction in 10% to 45% of patients (Kassell et al, 1985; Lanzino et al, 1999; Song et al, 2006; Vajkoczy et al, 2005; Wurm et al, 2004).
In vessel endothelium, nitric oxide (NO) is continuously generated from the endothelial nitric oxide synthase (eNOS) gene to maintain basal vascular tone (Quyyumi et al, 1995). Aneurysmal SAH results in alterations in eNOS gene expression and disruption of the balanced regulation of cerebral vascular tone (Khurana et al, 2002; Weir and MacDonald, 1993). Studies have found abnormal cerebrospinal fluid NO levels in humans after aSAH (Sadamitsu et al, 2001; Woszczyk et al, 2003). Furthermore, in dogs and
We hypothesize that the eNOS T-786 single-nucleotide polymorphisms (SNPs) are associated with the incidence of post-aSAH cerebral vasospasm. Presence of this allele may allow clinicians to identify high-risk individuals and tailor intensive care management in a patient-specific manner. In this context, the principal aims of our prospective clinical study were to (1) determine if there was an association between the presence of such polymorphisms and the presence of post-aSAH vasospasm; (2) determine if differences in such polymorphisms had an effect on the incidence of cerebral infarction secondary to vasospasm.
Materials and methods
Patient Population
Patients presenting to our institution from January 2004 to December 2006 with nontraumatic, computed-tomography (CT)-confirmed SAH were prospectively approached for enrollment into this IRB-approved study. Patients were eligible if they presented within 2 days of SAH. After obtaining an informed consent, a buccal swab was used to collect cheek cells for DNA analysis. All patients provided samples within 3 days of SAH onset. Patients later found to have non-aneurysmal SAH were excluded from the study.
Management Protocol
A standardized management protocol was used in the management of all aSAH patients including immediate aneurysm repair whenever feasible. Decisions regarding treatment modality were made by combined teams of open-neurovascular and endovascular surgeons. Vasospasm prophylaxis consisted of nimodipine administration and the active maintenance of central venous pressure greater than 5 mm Hg. Postoperatively, patients developing symptomatic vasospasm were treated with induced hypertension and hypervolemia (central pressure ≥8 mm Hg). Elevation of intracranial pressure above 20 mm Hg was treated aggressively with mannitol and/or hypertonic saline.
Study Outcomes
Patient demographic information, medical/surgical history, and clinical course were obtained at the time of enrollment from family members or by review of medical records. Patients were prospectively followed for adverse events until hospital discharge. All outcomes were compiled blinded to the knowledge of a patient's genotype.
Symptomatic vasospasm was defined as any change in mental status of greater than 2 points in the Glasgow Coma Scale or any new neurologic deficit that could not be explained by other etiology (Pickard et al, 1989). Patients suspected of clinical vasospasm underwent physical examination, imaging, and laboratory investigation to rule out other possible causes. Other potential causes of clinical deterioration, such as hydrocephalus, rebleeding, cerebral edema, retraction injury, ventriculitis, metabolic derangements, and seizures were rigorously excluded. Clinical deterioration from symptomatic vasospasm, thought to be consistent with vasospasm, were treated with HHHT (hypertensive, hypervolemic, and hemodilutional therapy) to maintain a hematocrit of approximately 30, systolic blood pressure >160 mm Hg, and central venous pressure of >8. When clinical evidence of vasospasm persisted for more than 2 h despite HHHT, cerebral angiography was used to document vasospasm. Additionally, poor-grade and sedated patients received CT or MR (magnetic resonance) perfusion on day 4 to 8 to assess for vasospasm. Patients with vasospasm on CT or MR perfusion then received angiography. On angiography, patients were considered to have vasospasm if there was arterial narrowing compared with normal vessel diameter (mild<30%, moderate 30% to 60%, severe>60%). Patients with moderate or severe angiographic vasospasm were treated with intraarterial administration of vasodilators and balloon angioplasty when indicated. Cerebral infarction because of vasospasm was defined as any new lucency on CT- or diffusion-weighted-imaging-positive signal on MRI in the appropriate vascular territory after exclusion of other potential causes.
Genetic Analysis
All genetic analyses were performed by laboratory personnel blinded to patient identities. Genomic DNA was extracted from buccal swabs using MasterAmp Extraction kits (Epicentre, Madison, WI, USA) and approximately 50 ng DNA was amplified in 10 μL reactions with primers 5′-GCATGCACTCTGGCCTGAAGT-3′ and 5′-CAGGAAGCTGCCTTCCAGTGC-3′ (500 nmol/L each), 0.25 μL JumpStart RED AccuTaq DNA polymerase (Sigma-Aldrich, St Louis, MO, USA), 1 × AccuTaq reaction buffer, and 500 μmol/L dNTPs. Polymerase chain reaction cycles consisted of denaturation at 94°C for 30 secs, annealing for 30 secs (touchdown from 65°C for first 10 cycles to 57°C for last 20 cycles), and extension at 72°C for 90 secs. After a final 5 mins extension, PCR products were treated with ExoSapIT kits (USB, Cleveland, OH, USA), bidirectional sequencing was performed with the same primers on 20 to 40 ng of PCR products using BigDye Termination v3.1 Cycle Sequencing kits (ABI, Foster City, CA, USA), and sequencing products were analyzed on an ABI 3730xl capillary instrument. Sequence traces were aligned and SNPs determined using SeqMan software (DNAStar, Madison, WI, USA).
Statistical Analysis
Data are presented as mean±s.d. for continuous variables, and as frequency for categorical variables. Statistical analyses were carried out using unpaired Student's
Results
Cohort Characteristics
Seventy-seven patients with SAH and confirmed aneurysms by angiography provided consent and genetic material for this study. The eNOS T-786 SNP was sequenced in all patients. Genotypes were in accordance with the Hardy—Weinberg equilibrium (
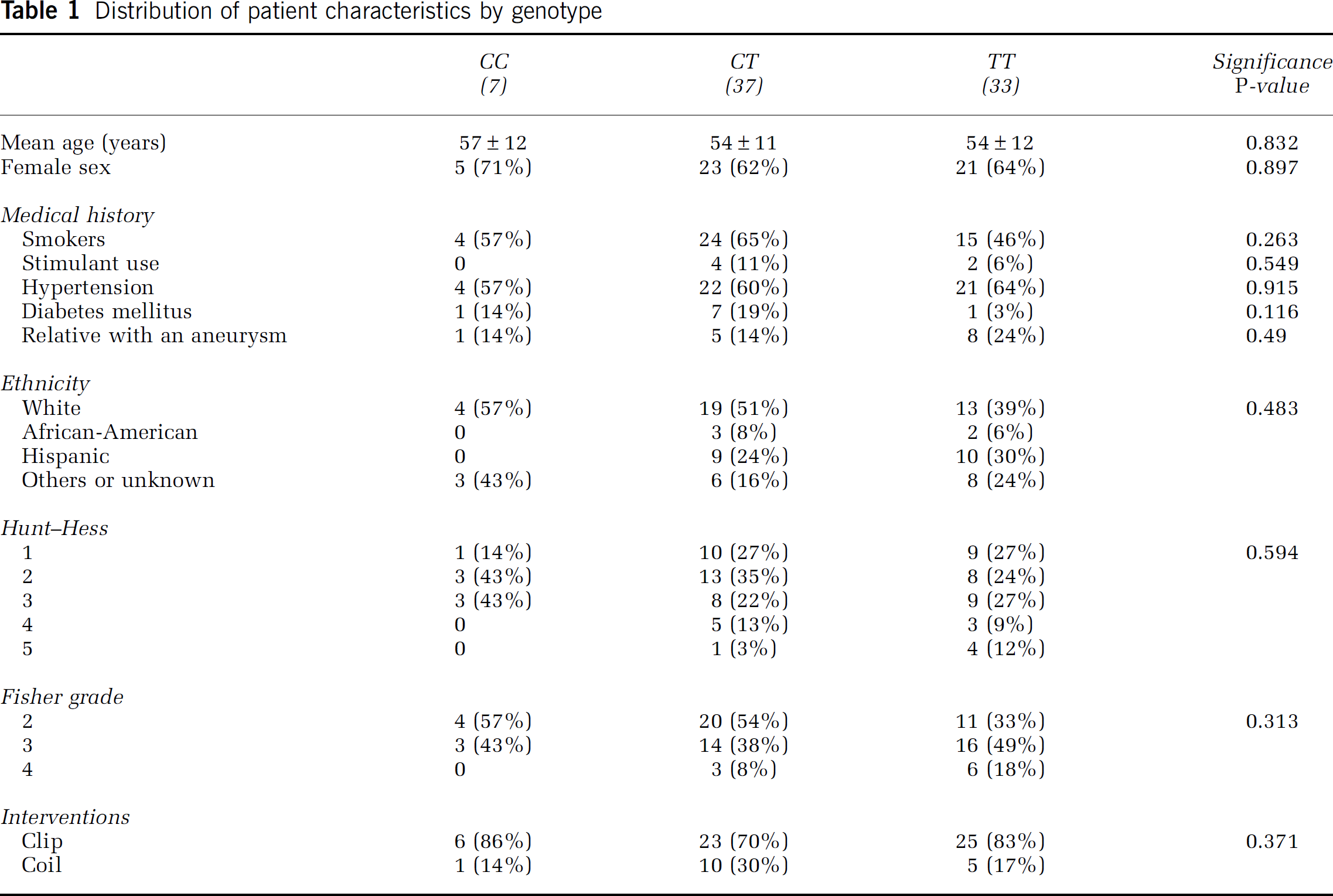
Distribution of patient characteristics by genotype
Cerebral Vasospasm
In total, 43% of patients had either symptomatic or angiographic vasospasm. Thirty percent of patients had symptomatic vasospasm, 38% had angiographic vasospasm, and 35% had vasospasm necessitating endovascular treatment. Twenty percent of patients had an infarction after aneurysm rupture and 10% had an infarction secondary to vasospasm.
There was a significant increase in symptomatic or angiographic vasospasm in patients with the TT genotype (61%) versus the CT (35%) or CC genotype (0%,
Outcome according to genotype
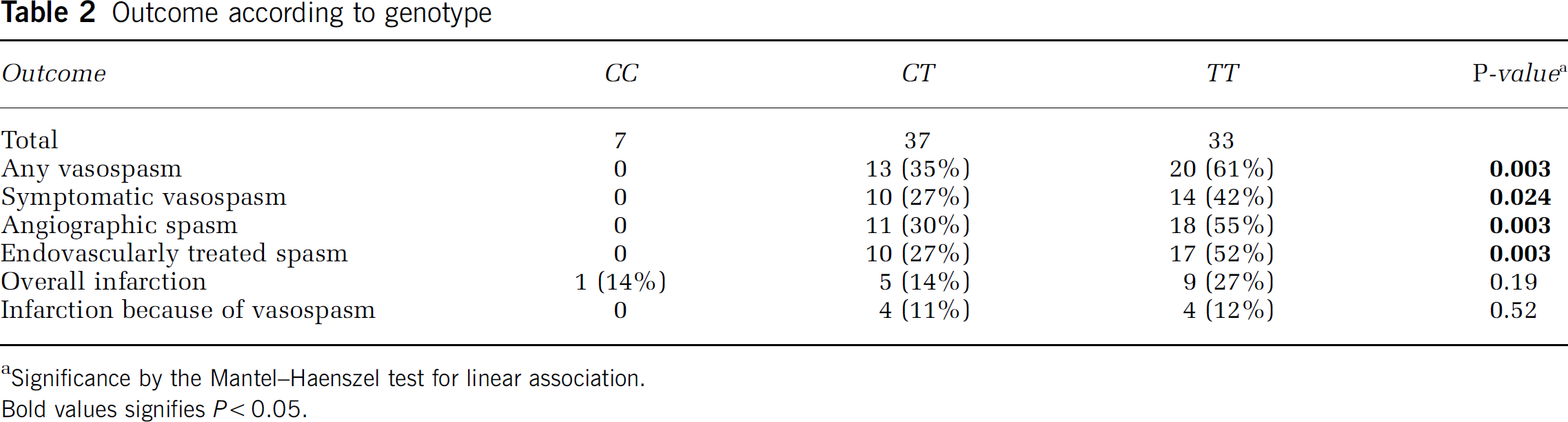
Significance by the Mantel—Haenszel test for linear association.
Bold values signifies
In multivariate logistic regression analysis, genotype was the only significant predictor of vasospasm (see Table 3). The T allele was a significant predictor of vasospasm (OR 3.4, 95% CI: 1.3 to 9.0,
Multivariable logistic regression analysis of genotype as a predictor of vasospasm
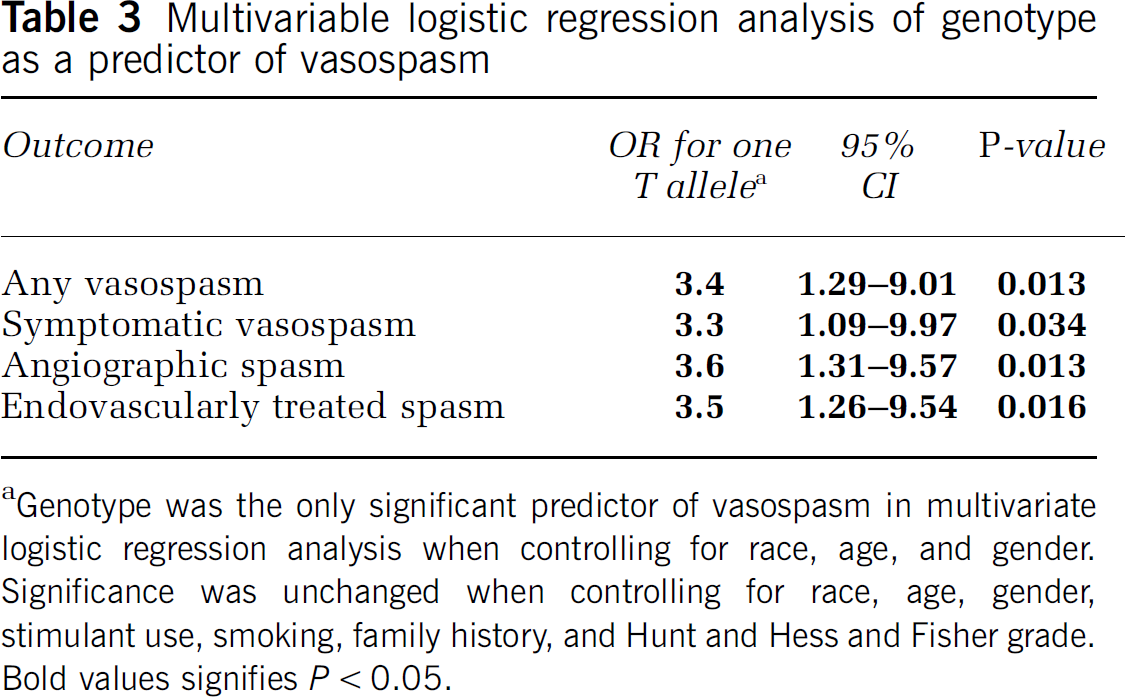
Genotype was the only significant predictor of vasospasm in multivariate logistic regression analysis when controlling for race, age, and gender. Significance was unchanged when controlling for race, age, gender, stimulant use, smoking, family history, and Hunt and Hess and Fisher grade.
Bold values signifies
Infarction
There was no significant difference in infarction in patients according to genotype. Fourteen percent of patients with CC and 14% of patients with CT had infarction versus 27% of TT patients (
Discussion
Numerous studies have attempted to determine prognostic indicators of vasospasm, as identification of high-risk individuals may allow post-aSAH management to be tailored in a patient-specific manner. History of smoking, preexisting hypertension, and hypovolemia have all been linked with vasospasm (Lasner et al, 1997; Rabinstein, 2006). Although experts have argued over the role of age, the strongest known predictive factor for vasospasm is the amount of blood on CT (Fisher grade), which often correlates with the severity of the vasospasm (Davis et al, 1980; Fox and Ko, 1978). Differences in the incidence of vasospasm and outcomes in patients with similar Fisher grade, and a genetic association with aneurysm formation, have led to the theory that genetic polymorphisms encoding vascular regulatory proteins may result in variable levels of vascular spasticity in response to aSAH.
It is likely that the onset of aSAH is multifactorial in nature and dependent on genetic characteristics and clinical variables associated with aneurysm rupture. The eNOS T-786 SNP has received much attention because of its location within the promoter region of the NO gene (Nakayama et al, 1999). In this study, Fisher grade and genotype were the only significant predictors of vasospasm in univariate analysis. In multivariable analysis, genotype was the only independent predictor of vasospasm when accounting for race, age, gender, stimulant use, smoking, family history of aneurysm, and the Hunt and Hess and Fisher grades. Patients with a T allele had 3.3 times higher odds of developing symptomatic vasospasm and patients with the TT genotype were 10.9 times more likely. Patients with the T allele had an OR of 3.5 of necessitating treatment for vasospasm and patients with the TT genotype had an OR of 12.0; thus, the T allele is not only a predictive marker of vasospasm, but a risk factor for severe vasospasm requiring endovascular therapy.
When stratified according to genotype, there was no significant difference in the incidence of infarction because of vasospasm. Twelve percent of patients with the TT and 11% of patients with the CT genotype had infarction because of vasospasm versus 0% in patients with the CC genotype. Although this difference was not statistically significant, our study was not powered to detect differences in infarction. This may also be because of a large number of clinical and genetic factors that link vasospasm with infarction in a vascular territory. This may also be because we treat vasospasm aggresively with the intent to avoid the development of infarction.
In this study, all polymorphisms were in Hardy—Weinberg equilibrium. Minor allele frequencies were not significantly different from those in previous studies (Akagawa et al, 2005; Khurana et al, 2004; Krex et al, 2006; Krischek et al, 2006; Song et al, 2006), and there was no significant difference in racial groups according to genotype. These results are consistent with more recent studies in larger populations (Rossi et al, 2006). Earlier, smaller studies hypothesized that the CC genotype was because of new mutations as the incidence of CC was 0.9% (
Our results contrast to a previous study examining genetic polymorphisms of eNOS T-786 SNP and cerebral vasospasm. This may be because of inadequate power, and/or differences in ethnicity, incidence of alleles, and prevalence of vasospasm. In one study of 28 Fisher grade III aSAH patients, it was found that patients with vasospasm had a nonsignificant increased risk of having the C allele (OR 7.1, 95% CI: 0.88 to 57.5) (Khurana et al, 2004). These results may have been because of underpowering or because of the fact that only one of these patients had the CC genotype. In a study of vasospasm, after aSAH in 133 Korean patients, the eNOS T-786C polymorphism did not confer any increased risk of symptomatic vasospasm, but the CT genotype was associated with worse outcome (Song et al, 2006). These differences may again be accounted for by the variance in racial characteristics; 0% of Korean patients had the CC genotype. They also may be accounted for by the low rate of symptomatic vasospasm (12.8%) seen in this Korean population as compared with previously published studies (20% to 65%) (Kassell et al, 1985; Lanzino et al, 1999; Song et al, 2006; Vajkoczy et al, 2005).
Although NO plays a role in vasospasm after aSAH, the precise pathophysiology remains unclear. Studies have proposed that this process may be because of increased (Ignarro, 1990; Pluta et al, 1996) or decreased NO levels (Dumont et al, 2003; Moncada et al, 1991). Studies have reported decreased levels of NO in animals after experimental aSAH (Kasuya et al, 1995); other studies in humans with aSAH found an initial decrease in NO followed by an increase in NO between 2 and 8 days (Woszczyk et al, 2003).
It is unclear as to how different allelic combinations of the eNOS T-786 SNP lead to pathologic processes. Different allelic combinations have been associated with coronary spasm (CC) (Nakayama et al, 1999), aneurysm size (CT) (Akagawa et al, 2005), and outcomes after coronary spasm (CT) (Nishijima et al, 2007), cerebral vasospasm (CT) (Song et al, 2006), and cardiovascular mortality (TT) (Rossi et al, 2006). The role of eNOS expression in aSAH is controversial (Pluta et al, 1996; Kasuya et al, 1995; Hino et al, 1996; Park et al, 2001; McGirt et al, 2002). Pathogenesis because of alterations in polymorphisms may occur through a variety of mechanisms including decreased promoter activity leading to decreased NO or increased promoter activity leading to increased NO. Increased NO may lead to oxidative stress (Yung et al, 2006), intimal hyperplasia (Hingorani et al, 1999; Kuhlencordt et al, 2001), systemic hypertension (Kuhlencordt et al, 2001), vascular smooth muscle proliferation (Dumont et al, 2003; Moncada et al, 1991), increased platelet aggregation, and proinflammatory adhesion (Dumont et al, 2003; Moncada et al, 1991). These mechanisms of dysfunction may lead to alterations in smooth muscle proliferation, vessel dilation, and inflammation seen in the pathogenesis of vasospasm after aSAH (Dumont et al, 2003; Khurana et al, 2004; Moncada et al, 1991).
In one study, the eNOS promoter was isolated from patients with coronary spasm and after being subjected to hypoxic conditions for 24 h, it was found that genes with the C allele had decreased promoter activity (Nakayama et al, 1999). In this study of Asian patients, only 3 of 335 patients had the CC genotype, which differs significantly from other studies of white patients where the CC genotype comprised 19% of 1,096 patients (Rossi et al, 2006). In this larger study by Rossi
Further studies of eNOS, the promoter, and polymorphisms are needed to develop therapeutic agents that target the NO cascade. Preliminary studies have begun to look at invasive techniques to administer exogenous NO (Afshar et al, 1995; Wolf et al, 1998) or
Future studies should focus on the link between vasospasm, eNOS 786 polymorphisms, the eNOS promoter, and the amount of NO produced from the time of aSAH to the end of the vasospasm window (day 14). The role of the eNOS promoter and the corresponding levels of NO after aSAH throughout the window of vasospasm also need to be elucidated. These results should be correlated with long-term outcomes as it is unclear as to whether decreased incidence of vasospasm will result in improved functional outcome. The results of this study should be confirmed in larger racially diverse subgroups.
Conclusion
In conclusion, patients with a T allele have a significantly increased risk of developing severe vasospasm. This may help clinicians predict and identify high-risk patients. Furthermore, genetic analysis may allow clinicians to optimize early treatment for patients at risk for vasospasm and infarction, and improve patient outcomes.
Footnotes
Acknowledgements
We thank Lina Bruno for helping in bringing this project together. RMS was supported in part by an Alpha Omega Alpha Carolyn L Kuckein Student Research Fellowship.
The authors state no conflict of interest. The authors have no personal or institutional financial interest in drugs or materials in relation to this paper.