
Abstract
We report on the case of a 28-y-old man with both legs and left arm trapped for nearly 6 h after falling and subsequently being trapped by a boulder during a hike in the wilderness. Extrication required equipment designed for urban environments and was operated by an unconventional team of rescue professionals. The patient experienced multiple right lower-extremity orthopedic injuries, acute kidney injury secondary to rhabdomyolysis, and bilateral segmental pulmonary emboli. In this article, we detail the extrication and review the treatment guidelines for crush injuries that focus on aggressive fluid resuscitation prior to and during extrication and medication administration only if hyperkalemia presents. Wilderness rescuers should plan for the use of unconventional rescue equipment in austere prolonged rescue scenarios.
Introduction
Limb entrapment and crush syndrome in the backcountry are rare events. We report on an incident where collaboration between ground search and rescue, air search and rescue, and urban technical rescue resulted in the successful rescue of a hiker with 3 extremities trapped by a boulder. Injuries included fractures, soft-tissue injuries, and bilateral pulmonary emboli. The current recommendations for the treatment of crush syndrome, described as prolonged compression causing muscle necrosis and hyperkalemia, are discussed.
Case Report
In mid-October at approximately 0900, 2 men aged 28 y were hiking around Lake Viviane, a remote backcountry plateau in Washington State. Halfway through the 19-mile route, at an elevation of 2100 m, the patient fell while traversing an off-trail area with loose rocks. A boulder became dislodged and fell on the patient, trapping his bilateral lower extremities at the thighs and his left forearm. His hiking partner attempted to free the patient for 15 min before ascending to a ridgeline. He activated 911 30 min after the incident, and search and rescue (SAR) resources were subsequently dispatched. Due to the long ground approach, the local SAR unit immediately requested a neighboring county’s helicopter rescue team (HRT), which arrived at 1249 after a 68-mile flight. The HRT paramedic and rescue technician found the patient in a narrow V-shaped chimney approximately 5 feet wide at its widest, which opened over a 200’ cliff. A pyramid-shaped boulder of approximately 4’×4’×4’ was at the opening of the chimney, pinning the patient’s lower legs between the boulder and the ground and his left forearm between the boulder and the surrounding rock wall (Figures 1 and 2). The boulder was estimated to weigh 4000 lbs and was held in place by a 6-inch-diameter pine tree.
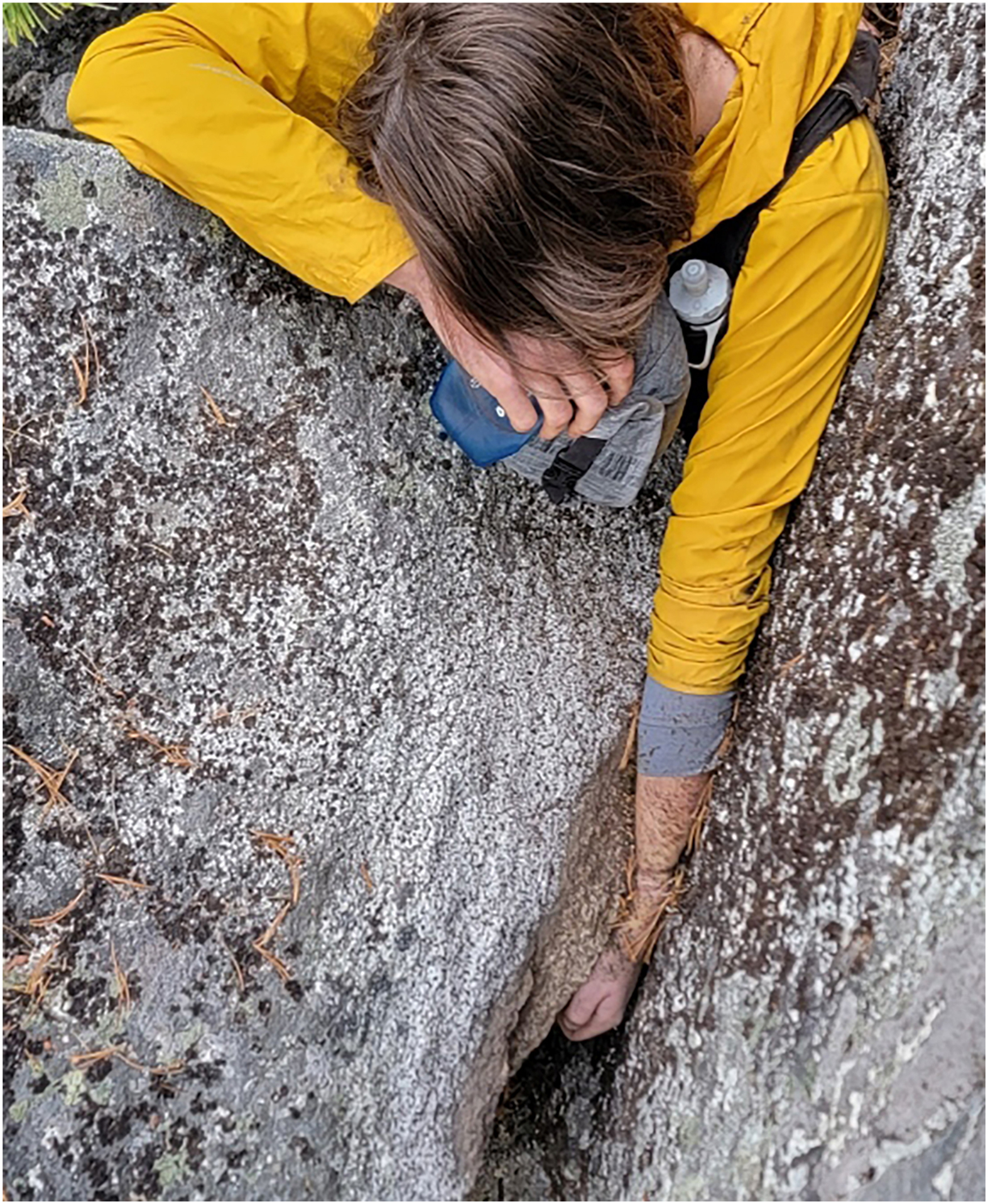
Initial view of the patient, with the left arm trapped by the boulder.

The patient’s legs prior to boulder displacement.
After attaching a rigging system to a nearby tree, the patient and rescuers were secured, and the patient was evaluated in detail. He reported severe pain in his right knee, was unable to move his right foot, and had sensation and movement in the left toes. He complained of significant pain in his left forearm, with distal sensation and limited purposeful motion. He had vomited several times prior to Emergency Medical Services’ arrival. He denied loss of consciousness and other complaints. Amputation was considered as a last-resort option; however, the position of the boulder at the upper thighs would have significantly complicated the procedure.
Physical examination revealed an alert and oriented patient with cool extremities dressed in a light jacket and running shorts. His left arm was trapped between the boulder and rock, with obvious soft-tissue damage as well as intact movement and sensation but decreased capillary refill. The medic was unable to visualize the legs. As more personnel arrived, they rappelled down the other side of the boulder to examine the lower leg. The right extremity demonstrated a 6-inch avulsion and crush injuries to the right knee and calf with moderate bleeding. The left extremity demonstrated a deformity of the distal right femur and proximal tibia/fibula. The left leg was normal in appearance. Initial vital signs were blood pressure of 68/52 mm Hg, heart rate of 130 beats/min, respiratory rate of 30 breaths/min, and oxygen saturation (SpO2) in the low 80s despite oxygen via a nonrebreather mask at 15 L/min. Lung sounds were noted to be clear in all fields.
An 18G IV line was started in the right upper extremity, and a 500-mL 0.9% saline bolus was administered for a goal systolic blood pressure of 90 mm Hg. Pain was controlled with 100 micrograms of IV fentanyl, and 4 mg of ondansetron were given for nausea. During extrication, 50 mg of ketamine was administered via slow IV push. Due to limited supplies, saline infusions were supplemented with oral hydration.
During the resuscitation and evaluation by the HRT team, the helicopter flew to a landing zone and retrieved a structural fire department technical rescue team with rescue equipment. The team was flown to the scene and lowered, along with equipment, via hoist. After an orientation and safety assessment, the team was tied into the rigging system. A high-pressure airbag was placed over a multilevel square of 4×4 wooden blocks (cribbing) and inflated to displace the boulder and free the left arm at 1429 (Figure 3). After movement of the boulder, vital signs were blood pressure of 118/76 mm Hg, heart rate of 119 beats/min, respiratory rate of 28 breaths/min, and persistently low SpO2. The left arm was splinted with a malleable splint, and no new additional injuries were noted on examination.

A view of the boulder with a high-pressure airbag (right) used to displace the boulder medially.
A second 18G IV line was started in the left arm proximal to the injury. Sodium bicarbonate, albuterol, and the remaining three 1000-mL bags of saline were prepared for extrication of the legs. A rescuer rappelled down to the base of the boulder to monitor the legs as the boulder was moved. A second airbag was placed over the cribbing to displace the boulder upward and free the legs. Immediately prior to displacement of the boulder, 50 mEq of sodium bicarbonate and 100 mg of ketamine were administered. By this time, the patient had received 3000 mL of saline. During the lifting, the boulder suddenly shifted. Operations were halted and reassessed. The patient reported that he could move his left leg, but the right leg remained trapped (Figure 4). Inflation of the airbag continued, and the patient was freed at 1448, nearly 6 h after the initial injury.

An overview of the scene. The medic (orange) and patient (yellow) can be seen on the right.
Brisk bleeding was noted from the right lower extremity. Bleeding was controlled with a combination of wound packing with hemostatic gauze, a pressure dressing, and a right thigh tourniquet. The patient was noted to be tachypneic and hypotensive. An additional 500-mL bolus of saline was administered. A pelvic binder was applied due to the mechanism of the injury, the legs were splinted, and the patient was placed in a vacuum mattress. He was wrapped in a space blanket, and small hot packs were applied before being placed in a Bauman bag for transport.
High winds delayed the originally planned hoist extraction. After a favorable shift in winds, the patient was lifted into the helicopter via hoist. The patient was flown 22 miles to a nearby level III trauma center, and care was transferred at 1708 (Figure 5).

An overview of the terrain and the rigging system used to lift the patient into position for the hoist operation into the helicopter.
Evaluation at the trauma center revealed an open right tibial plateau fracture (Schatzer type 1), right fibular head and neck fractures, an open right lateral femoral condyle fracture, and bilateral segmental and subsegmental pulmonary emboli. Initial laboratory results were significant for a venous lactic acid level of 10.7 mmol/L, hemoglobin level of 11.8 g/dL, creatine kinase (CK) level of 2263 units/L, and creatinine level of 1.32 mg/dL. The patient was resuscitated with additional crystalloids. He was taken emergently to the operating theater by a combined orthopedic, trauma, and vascular surgery team for a 4-compartment fasciotomy of the right leg, right knee arthrotomy, wound irrigation and debridement, and vascular evaluation. The pulmonary emboli were treated with a heparin drip, which was transitioned to therapeutic enoxaparin on hospital day (HD) 3. The patient was stabilized and transferred during the afternoon of the next day to a tertiary care center for skin grafting and reconstructive surgery. The laboratory results at time of transfer were significant only for an unmeasurably high CK level (>4100 units/L), and urine output was >100 mL/h. At the tertiary care facility, he underwent successful open reduction and percutaneous fixation of his fractures on HD 3. He was taken back to the operating theater for further debridement and wound vacuum placement on HD 6 and then split-thickness skin graft placement to cover a 20×10-cm2 tissue defect of the right leg on HD 10. He was discharged home on HD 11 to continue outpatient rehabilitation for the orthopedic injuries and a right foot drop secondary to a deep fibular nerve injury.
Discussion
Crush injuries requiring technical rescue are a common occurrence in urban and suburban environments, especially in natural disasters such as earthquakes, where the incidence ranges from 2 to 15% of all injuries. 1 Due to this prevalence, many urban and suburban regions of the United States have teams that specialize in the technical rescue of patients trapped in building collapses, trenches, or vehicles. Prehospital treatment in the nonwilderness setting is usually truncated due to short transport times and proximity to a hospital.
The risk of crush syndrome increases after 1 h of entrapment and becomes very likely after 4 to 6 h of entrapment. Sequelae of compartment syndrome include hyperkalemia, acidosis, and compartment syndrome, whose symptoms include pain with passive range of motion, paresthesias, and loss of pulse as a late sign. Treatment emphasizes early recognition and treatment of compartment syndrome, rhabdomyolysis, hyperkalemia, and associated orthopedic and vascular trauma. 1
Older guidelines, such as the ones used during this rescue, emphasized hyperkalemia pretreatment to include sodium bicarbonate infusion, insulin if available, and albuterol in addition to copious fluids. Current literature now centers on aggressive fluid resuscitation and treatment of hyperkalemia, if it presents, rather than prophylactic treatment. The European Renal Association and International Society of Nephrology recommend a fluid administration rate of 1000 mL/h of crystalloids for 2 h and then 500 mL/h before and during extrication for a goal of 3000 to 6000 mL/d of crystalloids, with a goal urine output of ≥50 mL/h. Important to note is that in anuric patients, crystalloid volume should be limited to 500 to 1000 mL/d with replacement of fluid losses as per the above guidelines. 2 The US Department of Defense Joint Trauma System’s Clinical Practice Guidelines (JTSCPG) also emphasize early and aggressive fluid resuscitation. The JTSCPG recommends a 2000-mL isotonic crystalloid bolus prior to extrication and a 1000-mL/h maintenance rate for a goal urine output of 100 to 200 mL/h. If IV or intraosseous access cannot be obtained, the JTSCPG recommends oral intake of an electrolyte solution or a 500-mL/h rectal infusion of an electrolyte. For patients trapped for >2 h and those in whom fluid resuscitation cannot be initiated immediately, the JTSCPG recommends that 2 side-by-side tourniquets be applied immediately prior to extrication. 3
Pulmonary emboli within the first 24 h after a traumatic injury have been documented in the trauma surgical literature. A study of 35,424 trauma patients demonstrated a pulmonary embolism rate of 0.27%. Of them, 37% were diagnosed between the first and fourth days of hospitalization. 4 One previous case of crush syndrome–associated pulmonary embolism was described in a man who fell asleep in a cross-legged position for 10 h. 5 In this case, the risk from the traumatic injury was compounded by the prolonged immobility and compression of 3 of 4 limbs. Rescuers should be alert to the possibility of pulmonary embolism and aggressively investigate tachycardia and hypoxia combined with prolonged stasis that is unexplained by other causes. Total tourniquet time was 140 min. Given the presentation of hypoxia prior to tourniquet application, it is unlikely that the tourniquet contributed to deep venous thrombosis formation.
As more people venture into the backcountry, the rate of fall injuries in the wilderness has increased. Nonclimbers have a higher rate of severe head and facial injuries than climbers, with soft-tissue injuries occurring in 57% of all fall patients. The average time from injury to hospital arrival was 4 h. 6
Injuries caused by boulders and shifting rocks are rare but do occur. The vast majority of these involve falling rocks and do not result in entrapment; however, there are case reports of boulder entrapments in both Utah and Italy, 7 including the well-documented self-rescue of Aron Ralston. In these situations, the decision between extrication and amputation must be weighed against time, location, and practicality. To date, however, there has not been a documented case of patient extrication in the wilderness using urban technical rescue equipment such as high-pressure air-lifting bags and wooden cribbing. Integration of these devices into a mountain rescue scenario requires extreme adaptability, mental flexibility, and problem solving between different groups of responders that traditionally do not train together. Agencies should consider conducting joint training between these groups using a variety of tools and procedures to enhance interoperability.
Footnotes
Acknowledgements
Author Contributions: All authors contributed to the data collection, writing, editing, and approval of this manuscript.
Financial/Material Support: None.
Disclosures: None.