
Abstract
Objective
To investigate the incidence and causative agent of the recurrent outbreaks of acute gastrointestinal illness (AGI) among different rafting groups on the Colorado River in the Grand Canyon National Park during the 2012 summer season.
Methods
Confidential illness reports were completed by all individuals with symptoms of AGI, and samples of fecal matter and vomitus, surface swabs of rafting equipment, and environmental swabs at stops along the hiking corridor were collected and tested for the presence of norovirus using reverse transcription–quantitative polymerase chain reaction (RT-qPCR).
Results
During the active outbreak period between May 9 and July 9, 2012, 97 rafters (1.4%) from 10 trips (2.9% of all trips) declared AGI symptoms. AGI incidence within the 10 infected trips varied from 6% to 88%. Outbreaks occurred in 3 distinct temporal clusters that involved 2 different genogroups of norovirus. All available toilet fecal samples (5 samples) were positive for norovirus RNA: 1 with genogroup I (GI) and 4 with GII. The vomitus sample tested positive for GI. None of the fomite samples from rafting equipment or from the hiking corridors were confirmed for norovirus.
Conclusions
The results suggest that norovirus may have been introduced by ill or asymptomatic individuals actively shedding the virus in their vomitus or feces, and spread within, or between, river trips by different modes of transmission. This study reinforces the importance of appropriate guidance and practice regarding norovirus prevention and the necessity of postoutbreak containment in relatively isolated groups of individuals.
Introduction
Noroviruses (NoVs) are single-stranded RNA, nonenveloped viruses that are the leading cause of nonbacterial acute gastrointestinal illness (AGI) worldwide. The Centers for Disease Control and Prevention (CDC) estimate that 21 million cases of AGI are caused annually by NoV in the United States, which includes 70,000 hospitalizations and 800 deaths. 1 Noroviruses belong to the family Caliciviridae and are divided into at least 5 genogroups, of which genogroup I (GI), GII, and GIV infect humans. 2 Norovirus strains belonging to genogroup II, genotype 4 (GII.4) are currently the most prevalent strains that cause illness in humans. 1 The major clinical symptoms of NoV infection are nonbloody diarrhea, vomiting, and stomach pain. Severe dehydration as a result of the diarrhea and vomiting is the most serious complication of NoV illness, particularly in the remote wilderness environment where limited treatment measures are available. Low-grade fever, nausea, and stomach cramping may also be present. The symptoms start after an average incubation period of 24 to 48 hours and usually last 12 to 72 hours. 3 Kaplan et al 4 proposed clinical criteria for the identification of NoV-associated outbreaks of nonbacterial gastroenteritis in a medical or public health setting, which was subsequently demonstrated with 99% specificity as a diagnostic tool. 5
The National Park Service Colorado River Management Plan permits more than 24,000 people annually to raft the 225-mile stretch of the Colorado River that flows through the Grand Canyon. The rafters leave Lee’s Ferry (mile 0) in various vessels including oar boats, paddle boats, dories, or motorboats and travel to the destination, Diamond Creek (mile 225), which takes approximately 14 days for oar trips and 7 days for motorboat trips. The trips stop at beaches along the river so rafters may hike during the day and camp each night. Portable toilets are provided for all rafting trips because open defecation is not permitted, and all fecal waste must be removed from the vessels at the end of the rafting trip. Because of the duration of the trips, river water is used as a source of drinking and cooking water after filtration and disinfection.
Between 1994 and 2005, there were 6 years when investigations into AGI outbreaks among river rafters were conducted (1994, 1998, 2002, 2003, 2004, and 2005), 4 of which were confirmed to be caused by NoV by testing stool samples with polymerase chain reaction (PCR).6,7 Again, in 2010, NoV outbreaks occurred and affected 63 people on 10 river trips. Fecal samples from 3 of these trips tested positive for GII. That internal report concluded no definitive source of the infections but proposed that the virus was most likely imported into the trips and spread within and between river trips. The objective of the current study was to follow up the 2003 to 2004 data and was initiated because of a large recurrence of reported AGI outbreaks in the 2012 season.
Methods
Illness Reports
During the summer 2012 active outbreak period, all AGI symptomatic individuals (self-identified or identified by the guides) completed confidential illness report forms after each river trip (100% completion rate). Individuals within each rafting trip remain in close proximity with one another as they travel down the river; therefore, anyone vomiting or experiencing 1 to 2 days of diarrhea would easily be identifiable by fellow passengers and by the guides. A trip was identified as affected if there was at least one rafter who completed a form. The forms documented signs and symptoms, date and location of illness onset, and date of recovery (if occurred). Only ill individuals completed reports. The reports were then immediately sent to the National Park Service who then contacted the Coconino County Health District in Flagstaff, AZ. An investigation report at the county was then initiated, and researchers contacted the river companies and private trips to postpone the cleanup of gear and river toilets. The researchers were then dispatched into the canyon to collect illness reports as well as available fecal, vomitus, or fomite samples. No asymptomatic guides or passengers completed illness reports.
Fecal and Fomite Testing
All of the rafting groups were required to use portable toilets (airtight containers) to collect solid waste throughout each river trip. Personnel from the Coconino County Health District collected samples from the portable toilets and the rafting equipment the day after the trips had returned from the river. No samples were collected from asymptomatic trips returning from the Grand Canyon. A sample of vomitus was also obtained from an individual from Trip 4 who declared AGI symptoms, kept on ice during the trip, and then delivered to the Coconino County Health District.
Surface swabs of frequently touched fomites were collected in mid-July using prepackaged, sterile, moistened swabs, which were then placed in airtight vials for transportation. These locations included the Bright Angel Trail that leads from the South Rim to Phantom Ranch located at the bottom of the canyon, and then back up to the rim via the South Kaibab Trail. These samples were taken from toilet surfaces, restroom door knobs, and water faucet handles at the 1½ Mile House, 3 Mile House, Indian Gardens, Pipe Creek, Phantom Ranch, Boat Beach, South Kaibab Toilets, Cedar Point, and South Kaibab Trailhead in the Grand Canyon National Park. All samples were transported on ice.
Fecal Sample Preparation, Viral Rna Extraction, and Reverse Transcription
The fecal samples were prepared as described previously.
9
Briefly, 1 g (wet weight) of fecal sample was suspended in 9 mL of sterile phosphate-buffered saline solution and centrifuged at 2500 ×
Quantitative POlymerase Chain Reaction (QPCR)
TaqMan-based qPCR assays for GI, GII, and GIV NoV were performed with a LightCycler 480 Real-Time PCR Instrument II (Roche Diagnostics, Mannheim, Germany), as described previously.10,11 Briefly, reaction mixtures (25 μL) consisted of 12.5 μL of LightCycler 480 Probes Master (Roche Diagnostics), forward and reverse primers, probe(s), and 2.5 μL of cDNA template. The reaction mixtures were subjected to thermal cycling, and fluorescence readings were collected and analyzed with LightCycler 480 Software version 1.5 (Roche Diagnostics).
Results
Outbreak Summary
The overall incidence of NoV-like symptoms of AGI among river rafters who launched from Lee’s Ferry between May 9 and September 28, 2012, was 1.4% (97 of 7136 total rafters). Ten of 347 trips had at least one affected individual (2.9% trip infection rate), and the incidence rate of AGI within infected trips varied from 6% to 88%. The affected trips included 6 commercial, 2 private, and 2 science study trips, with a trip duration of 8 to 9 days for motorboat rafting and 13 to 18 days for oar rafting (Table 1). The AGI symptoms started at various locations along the river corridor.
Summary of the gastroenteritis outbreaks among the Colorado River rafters in the Grand Canyon in 2012 summer season
Clusters identified based on the onset of illness date.
NA, not available; numbers in parentheses indicate the number of samples tested for norovirus (NoV).
Based on the onset of illness date, the 10 trips were grouped within 3 distinct clusters (Table 1, Figure); trips 1 and 2 (cluster I, onset of illness date of May 9–12), trips 3 and 4 (cluster II, May 30–June 5), and trips 5–10 (cluster III, June 24–July 3) were all in close geographical and temporal proximity to each other throughout their respective river trips. However, the first onset of illness occurred at various locations along the river even within a cluster. Six of the 10 trips had first onset of illness before reaching the Phantom Ranch lodge (river mile 88), where the passengers were exchanged for some of the trips, whereas the other 4 trips experienced onset of illness at or after leaving Phantom Ranch.
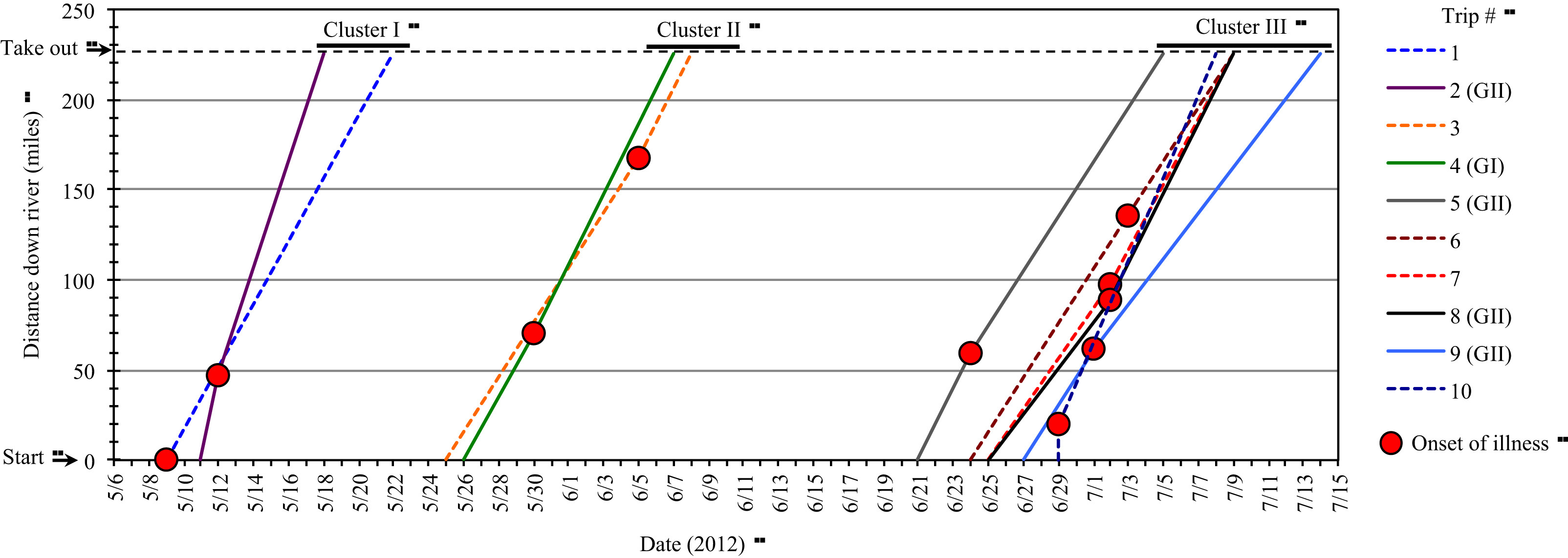
Temporal and geographical relationship of trips and onset of gastroenteritis on the Colorado River, summer 2012. Red circle indicates index case within individual trips. Norovirus was detected in stool samples from the trips indicated with solid lines, whereas no stool sample was available from the trips indicated with broken lines.
Detection of Norovirus
Stool samples from the portable toilets were collected from 5 of the 10 rafting trips that reported AGI symptoms. All of the 5 portable toilet samples tested positive for NoV as determined by RT-qPCR (Table 1). Trips 2, 5, 8, and 9 had confirmed GII norovirus from toilet fecal samples, whereas trip 4 had the only confirmed GI norovirus from a sample of vomitus as well as a group toilet fecal sample (Table 1). All surface swab samples taken on the same date at the trip’s warehouse (food containers, water jugs, toilet seats, soap containers, and inflatable sleeping pad nozzles) were negative for NoV. The swab fomite sample set from trip 7 (collected after the cleaning process from materials and supplies including a “toilet key,” toilet brushes, and cleaned groover boxes and lids) was also negative for NoV. All 26 swab samples for NoV throughout the main hiking corridors in the Grand Canyon were negative.
Discussion
In the last few decades, several major gastroenteritis outbreaks have occurred among Colorado River rafters, some of which have been confirmed to be caused by NoV.6,7 Norovirus outbreaks in 2002 were associated with the Glen Canyon Dam wastewater treatment plant upstream from the Lee’s Ferry departure point. 6 All of these NoV outbreaks began in the first few days of the rafting trip downstream (a temporal pattern not found in the current study). Contaminated delicatessen meats that were handled by an ill individual at a meat company, packaged, and then consumed on 13 river trips that infected 136 rafters caused the 2005 outbreak. 7 More recently, NoV outbreaks on 10 river trips in 2010 affected 63 people (a similar infection rate to the present study). Fecal samples from 3 of these trips tested positive for the GII genogroup. The authors suggested that the virus was most likely imported into the trips and spread within and between river trips. 8 Consistent with typical patterns of NoV outbreak, 1 the trips with infected individuals temporally clustered and in some cases intersected in 2012 (Figure). In all cases, clinical symptoms on the illness reports fit the first 3 definers of the Kaplan criteria established to diagnose NoV outbreaks in the absence of laboratory diagnostics4,5 (Table 2). The presence of norovirus RNA was detected in 100% of fecal toilet samples and was confirmed by laboratory analysis for 5 trips.
The NoV identified from trips in cluster 1 (trip 2) and cluster 3 (trips 5, 8, and 9) was GII, whereas the NoV identified from a single trip (trip 4) in cluster 2 was GI. The presence of 2 different genogroups suggests that all of the virus infections were not from a single source such as food or river water contamination. It is possible that infections within a given group could have originated from a common source, such as the GII strain that infected the trips in group 3. However, the identification of the primary source(s) of the 2012 NoV outbreaks is beyond the scope of the current study. Future laboratory sequencing analysis will explore the molecular origin of these NoV strains in an attempt to further identify their environmental sources.
Norovirus is highly infectious owing to its very low infective dose, reportedly requiring as few as 18 virus particles. 12 As ill individuals on multiple river trips traveled down the Grand Canyon river corridor, high quantities of vomiting and fecal shedding of NoV may have occurred during the outbreak periods. Illness reports stated that rafters were vomiting on beaches, boats, and into the river. It is known that projectile vomiting of 30 mL distributes up to 3 × 108 aerosolized virus particles. 13 Ill individuals also had diarrhea for 24 to 48 hours that may have been deposited onto toilet lids, onto beach sand, and into the river. After infection, and the NoV incubation period of 24 to 48 hours, individuals will begin to show symptoms. Fecal shedding peaks approximately 4 days after NoV infection, with a median peak amount of viral shedding of 9.5 × 1010 genomic copies/g of feces. 14 Infected individuals shed NoV in their feces for an average of 14 to 30 days after the resolution of symptoms.14,15 Therefore, if proper hand hygiene, disinfection, or containment were not followed, NoV particles can be transmitted to surfaces, beach sand, river water, and person-to-person or trip-to-trip during the rafting trips.
Norovirus is also known to be easily transmitted in close quarters 16 and recreational water, and can survive at cold temperatures for long periods. 17 The Colorado River in the Grand Canyon averages 10°C and forms very large eddies often adjacent to camping beaches. Although the main current contains a large volume of water and flushes quickly downriver, eddy water does not readily circulate or enter the main current. Therefore, these cold-water eddies are a potential source of NoV contamination within or between river trips via direct bathing in contaminated river water or through consumption of incompletely treated contaminated water. Additionally, physical contact with contaminated beach sand can be a source of NoV contamination that people may not be aware of while on a river trip. 18 The NoV-affected trips within the 3 groups camped at some of the same campsites on the same night or within 1 night of each other while individuals were actively ill. One trip reported witnessing another passenger vomiting into Deer Creek while other trips were present. A member of the observer’s party declared AGI illness the day after the encounter. The notion that the river (and a possible location upstream or from a side stream) could be the primary source is possible; however, this is unlikely because of the high percentage of asymptomatic trips (97.1%) and the varied geographical distribution of illness onset (ranging from mile 1 to mile 180). In addition, the turnover time of guides between trips is 2 to 3 weeks, suggesting that it is unlikely that the guides were a source of cross-cluster contamination.
Multiple studies have confirmed the stability of NoV on a variety of surfaces for days to weeks after contamination. 18 –20 Contaminated food-contact surfaces, such as cutting boards and metal bowls, can easily transfer virus particles to common river trip foods such as lettuce and ham. 11 The guides of river trips are usually the food handlers for the entire group. Therefore, it is critical that they practice proper hand hygiene. In addition, contaminated fomites have been previously linked to a sustained NoV outbreak on successive houseboat trips. 16 Therefore, these fomites were most likely a key route of sustaining outbreaks of NoV during the summer of 2012 among rafters in the Grand Canyon.
Norovirus could not be detected in restroom or other fomites along the frequently traveled Bright Angel Trail hiking corridor in mid-summer 2012. Samples were taken 20 days after the last reported AGI among the rafters. Sampled surfaces were touched daily by hundreds of hikers, some of whom hiked down the Bright Angel Trail and joined a river trip at the halfway point at Phantom Ranch. However, the stability of the virus in the extreme temperatures of Grand Canyon summers is unknown, and short-term environmental contamination during an active outbreak cannot be ruled out. In addition, the sensitivity of the detection method (ie, swabbing a limited area of surface or fomite or testing only a few microliters of the samples) may too low to detect NoV RNA in the environmental swab samples. Future monitoring will include testing of the corridor areas during an active outbreak to determine whether potentially infective NoV particles can be transmitted in the hiking corridor.
Trip 1 is a good example demonstrating the importance of proper precautions and disinfection protocol to reduce the spread of disease in an active outbreak. Trip 1 had 2 passengers with their start of illness on day 1, the day the trip launched from Lee’s Ferry. Immediately, the trip leader took specific precautions to isolate the 2 ill individuals and prohibited them from food lines. They were instructed to diligently wash their hands after using the restroom, and common surfaces were disinfected with the proper bleach solution. Consistent with usual NoV infection, the ill passengers reported relief of their symptoms on day 2 within 24 to 48 hours of onset. It is possible, but not proven in the current study, that because of proper precautions no one else on the trip fell ill, as suggested by the absence of additional illness reports. In addition, the large variation of the proportion of rafters with AGI symptoms within an infected trip (6% to 88%) may be caused by variations in hygiene practices, which further emphasizes the importance of precautions.
It is possible that a river trip with ill passengers may have had NoV fomite contamination throughout their river gear including life jackets, boats, coolers, and kitchen and toilet equipment. River companies routinely clean their supplies and equipment in the warehouse within 24 hours after completion of a trip. Surface swab samples of cleaned groovers, groover lids, toilet brushes, and life jackets, taken after trip 7 (which had a 15% AGI incidence rate), tested negative for NoV RNA by RT-qPCR. Cleaning methods included the use of pressure washing equipment, rinsing life jackets, and professionally cleaning toilet boxes. This suggests that this cleaning approach after an AGI-affected trip may greatly reduce or eliminate the spread of NoV between groups of individuals via contaminated surfaces. Future studies may include a more thorough testing of surfaces for fomites before, during, and after river trips to find whether the virus is introduced and spread throughout the trips via this mode of transmission.
Limitations
Although we succeeded in investigating the epidemiology of the AGI outbreaks among rafters and identifying the causative agents, our study had several limitations. First, composite toilet stool samples were obtained from only 5 of the 10 ill trips owing to substantial logistical difficulty in acquiring these samples. In addition, we were unable to obtain individual stool samples from each ill passenger. Furthermore, we were unable to identify asymptomatic passengers who may have been infected. Second, because this project was designed as a retrospective study, the AGI reports were not always received in a timely fashion, sometimes arriving a few days to a week after a trip had concluded and thereby prohibiting the collection of any samples. It is also possible that not all trips with AGI reported to the National Park Service (NPS), or that ill individuals within a trip did not self-report to the guides. Third, the environmental study could not be conducted during the period of an active outbreak in which people were reported vomiting into sinks and waterspout areas. Without this testing, we could not determine whether NoV was detectable along the corridor during the period of active outbreaks. Also, the stability of NoV in extreme heat environments is unknown; thus the absence of NoV RNA in the swab samples does not necessarily mean a lack of contamination.
Conclusions
The overall incidence of NoV infection on the Colorado River in 2012 was relatively low (1% to 3%). However, once individuals became ill, the highly contagious virus appeared to quickly infect others within the trips because of their close proximity to one another. Various modes of viral transmission may have been involved including shared equipment and confined spaces within an infected trip and the common camping locations between trips. Previous studies on NoV have shown its remarkable transmissibility and stability on surfaces, in cold water, on beach sand, and on food. Although the exact route(s) of transmission could not be identified in this investigation, proper hygiene and preventative precautions, when implemented, as well as equipment cleaning protocols after trip completion, appear to be effective at limiting NoV infection rates. As a result, the NPS and Coconino County Health District established “The Norovirus Outbreak Prevention and Contamination Guidelines” in 2012 in an attempt to decrease the incidence of NoV in these remote, yet tightly clustered, rafting trips 21 (Table 3).
Footnotes
Acknowledgments
This study was partly supported by The University of Arizona National Science Foundation Water and Environmental Technology (WET) Center and Water Research Foundation for laboratory analyses, the Coconino County Health District for collection of samples and illness reports, and a travel grant from Midwestern University to Anne Magill-Collins for her presentation at Winter Conference of the Wilderness Medical Society in Park City, UT, in February 2013. Material support was provided by the Coconino County Health District and the Department of Soil, Water and Environmental Science, University of Arizona.
☆
Presented in the Student Research Projects Symposium at the Wilderness Medical Society Winter Conference in Park City, UT, February 2013.