
Abstract
Introduction
From April 1 to May 31, 2022, Grand Canyon National Park received increased acute gastroenteritis reports. Pooled portable toilet specimens identified norovirus genogroups I and II. We sought to determine outbreak transmission contributors and individual risk factors while rafting or backpacking in the park.
Methods
Grand Canyon rafters and backpackers were surveyed online from June 13–July 8, 2022, and a Cox proportional hazards model was used to identify predictors associated with illness and adjusted for potential confounding factors.
Results
Among 762 surveys, 119 cases and 505 well persons submitted complete survey data. Illness among rafters was associated with interaction with ill persons during the trip (adjusted hazard ratio [adjHR] = 3.4 [95%CI 2.3–5.0]) and lack of any hand hygiene (1.2 [0.7–1.9]) or use of only sanitizer or water (1.6 [1.04–2.6]) before snacks. Younger rafters had higher illness rates compared to those ≥60 y (1.5 [1.2–1.8] for ages 40–59 and 2.2 [1.4–3.5] for ages <40 y).
Conclusions
Person-to-person transmission likely accounted for the widespread outbreak. Future outbreak mitigation efforts on river trips could focus on symptom screening before the trip starts, prompt separation of ill and well passengers, strict adherence to hand hygiene with soap and water, minimizing social interactions among rafting groups, and widespread outbreak notices and education to all park users.
Keywords
Introduction
Norovirus is a non-enveloped RNA virus in the Caliciviridae family that contributes to millions of gastroenteritis cases annually in the United States.1,2 Norovirus is also the most identified source pathogen among acute gastroenteritis (AGE) outbreaks.3,4 A review of US AGE outbreaks from 2009–2019 found that 62% were spread primarily by person-to-person contact. 3 Norovirus transmissibility can be reduced by handwashing with soap and water, avoiding food preparation until ≥48 h after symptoms end, and proper cleaning and disinfection of contaminated surfaces. 5 Factors that facilitate the transmissibility of norovirus include prolonged viral shedding after symptoms subside, the small number of viral particles (<100) required to result in infection, and its ability to persist on surfaces and resist heat, including outdoors.1,5
In 2022, Grand Canyon National Park (Grand Canyon) received nearly 65 000 overnight backcountry (undeveloped park areas) backpackers and rafters embarking on commercial and noncommercial (private) trips along a nearly 280-mile stretch of the Colorado River. 6 Rafting trips may have up to 18 persons per raft, including professional guides, and typically launch at Lees Ferry7–9 (Supplemental Figure 1). Rafting trips include access to hygiene facilities and portable toilets with waste going into a bag within sealed containers, which are referred to as “groovers.” Backcountry camping sites do not offer hygiene facilities, potable water, or toilets. All solid waste (feces and vomitus) must be carried out of the park.
The National Park Service Office of Public Health (NPS-OPH) requires commercial rafting outfitters to report 1–2 cases of AGE (nausea, vomiting, and diarrhea) at trip’s end by filling out an illness report form (IRF) for each ill person; when there are ≥3 cases, the trip leader is required to contact NPS-OPH by satellite phone as soon as possible. 8 Private trips must report 1–2 cases within 7 days of the trip and ≥3 cases within 24 h of the third case onset. 7 Backpacking permit holders are encouraged, but not required, to report illness to NPS-OPH. To reinforce adherence to public health statutes and codes, Coconino County Health and Human Services (CCHHS) conducts routine environmental inspections of all commercial outfitter warehouses during trip preparation.
Description of Outbreak Investigation
On April 8, 2022, NPS-OPH and Grand Canyon staff were notified of 7 cases of AGE on a commercial rafting trip. At that time, NPS-OPH and CCHHS shared norovirus infection control recommendations with outfitters, and CCHHS collected pooled groover samples for testing. CCHHS and NPS-OPH distributed a supplementary questionnaire for trip-level characteristics (trip report form [TRF]) to all affected commercial rafting trips. Outfitters and trip guides reported contact information, dates, means of transport (row or motor), food and beverage suppliers, menus, trip plans including stops and overnight stay locations, exchanges of passengers at Phantom Ranch, other group contact, and illnesses. By May 10, 5 additional commercial rafting trips reported cases, leading NPS-OPH, CCHHS, and Arizona Department of Health Services (ADHS) to contact the Centers for Disease Control and Prevention (CDC). By May 21, 13 additional trips with 102 cases were documented, and 27 backpackers also reported AGE. A specific source for the case increases had not been identified; therefore, NPS-OPH and CCHHS requested CDC aid in conducting an outbreak investigation.
During April 1–June 30, 2022, the Colorado River NPS Backcountry Permit Office (NPS-BPO) permitted 142 private trips (1824 persons) and 317 commercial trips (7182 persons) for a total of 9006 persons across 459 trips. The NPS-BPO reported 1206 hike-in permits (3976 persons) were issued for backcountry campers with at least one night outside of the main canyon corridor (developed campgrounds along popular trails linking North and South Rims).
We sought to determine outbreak transmission contributors and individual AGE risk factors while rafting or backpacking in the Grand Canyon by comparing behaviors (eg, hand hygiene practices) and environmental exposures (eg, drinking water source and treatment) among trips with ≥1 AGE cases during the trip or ≤7 days of trip end with trips that reported no cases.
Methods
The outbreak investigation team, comprised of NPS-OPH, CCHHS, and CDC, analyzed the initial IRFs and TRFs from trips before the expanded investigation began on June 1. Among 116 IRFs collected through May 31, most cases reported fatigue, vomiting, diarrhea, and nausea. 10 Acute onset, short duration (median 24 h), and predominance of vomiting implicated norovirus as the causative pathogen. CCHHS coordinated with the University of Arizona to test groovers from rafting trips before survey distribution. Nine pooled specimens from ill trips were positive for norovirus, including 2 trips in April (genotype I) and 7 trips in May (genotype II) 10 further supporting the suspicion of norovirus transmission.
Case Definitions
Since norovirus was suspected at investigation onset, we defined a probable case as a person who participated in Grand Canyon rafting or backcountry backpacking from April 1–June 16 and experienced any vomiting or diarrhea (≥3 loose stools in 24 h) within the 24 h before trip start through 3 days after their trip end. Unaffected trips were identified using the Grand Canyon online river trip launch calendars. 11 Well persons were defined as persons who did not report AGE, regardless of whether they were on an affected or unaffected trip.
Survey Distribution
We developed an online survey (Supplemental Materials) available through Qualtrics from June 13–July 8 and provided an email template with a survey link to river outfitters for distribution to passengers on affected and selected unaffected trips. As we were unable to obtain contact information for commercial passengers, rafting companies were asked to distribute the survey to participants of selected trips. All 14 commercial trips launched during the time of interest with ≥1 AGE case were selected, and 14 unaffected trips with a similar distribution of launch dates, group size, and trip duration were selected using information from NPS trip launch calendars 11 and rafting permits. We partnered with NPS-BPO to distribute the survey on June 16 to all private rafting trip participants aged ≥16 y and backpacking trip leaders with routes reported outside the main canyon corridor from April 1 to June 16. Survey distribution was limited to backpacking trip leaders due to the permit issuance process; leaders were asked to share the survey with their party members. The survey asked about symptoms, meals consumed, drinking water sources and treatment methods, and environmental exposures. We do not know the number of people who received the survey; however, completed surveys represented an estimated 14% of rafters and 12% of backcountry backpackers who were permitted for their respective activities from April–June 2022.
Analysis
IRF, TRF, and survey data were merged using name, age, sex, home state or country, and trip dates and analyzed using SAS v.9.4 (Cary, NC). Epidemic curves and frequencies of participant characteristics and exposures were stratified by activity type (commercial or private rafting or backpacking). Individuals with AGE onset in the 24 h before trip start were excluded (n = 5) for risk factor analysis, as their exposure preceded their backcountry trip. Cohort analysis was limited to persons who completed a survey and reported a trip start date during April and May. We generated Kaplan-Meier curves describing differences among rafters between cases and well persons by known risk factors, including age, encounters with ill persons, and hand hygiene. Univariable and multivariable Cox proportional hazard models 12 were used to assess the statistical significance of risk factors among rafters only. To improve sample size, commercial and private rafters were collapsed into a single multivariable model; commercial versus private trip type was included as a predictor in the model to account for the difference in participation of healthy participants due to survey distribution methods. Survival time was defined as days from trip launch to symptom onset; those with no symptoms were censored 3 days after trip end. Variables were selected using backward elimination. Month of trip launch was forced into the model to adjust for differences in risk over time.
Results
A total of 1255 persons consented to the survey and reported, at minimum, their activity type and whether they had AGE symptoms. Of 129 IRFs submitted to NPS, 57 were matched to the survey responses. In the merged dataset (n = 1242), 222 persons met the definition for cases and 1020 for well persons. Due to low case numbers among backpacking survey respondents, only descriptive analyses were conducted.
Backpackers
In total, 484 backpackers completed the survey and met either the case (n = 31) or well person (n = 453) definitions (Supplemental Table 1). Backpacker age ranged from 16 to 82 y (median 40 y), and 329 (69%) were male. Three reported AGE symptoms in the 24 h before the start of their hike. Among cases, hiking routes included most designated trails into the canyon, including North and South Rims, and hiking areas both east and west of the main park corridor. Most cases used the same toilet facilities or camping locations as other ill backpackers or visited river areas shared by rafters; however, potential exposures were spread out in time, and no single location was associated with all cases. Due to low case numbers among backpacking survey respondents, no additional analyses were conducted.
Rafters
Our analysis included 286 commercial and 470 private rafters (Table 1). Participants’ ages ranged from 18–82 y (median 52 y), and 440 (58%) were male. Most commercial trips lasted 1–2 weeks (median [interquartile range (IQR)] = 7 [6–13] days), while private trips lasted 2–3 weeks (16 [15–20] days). Among survey respondents, commercial trip participants had a higher proportion of AGE cases (n = 136, 47%) compared to private rafters (n = 55, 12%); however, in the context of the number of the 7182 commercial rafters and 1824 private rafters permitted to raft during April–June, the overall attack rate detected in the investigation was somewhat lower on commercial trips (2%) than private trips (3%).
Descriptive characteristics of Colorado River rafters in the backcountry of Grand Canyon National Park by activity type and gastroenteric symptom status, April–June 2022.
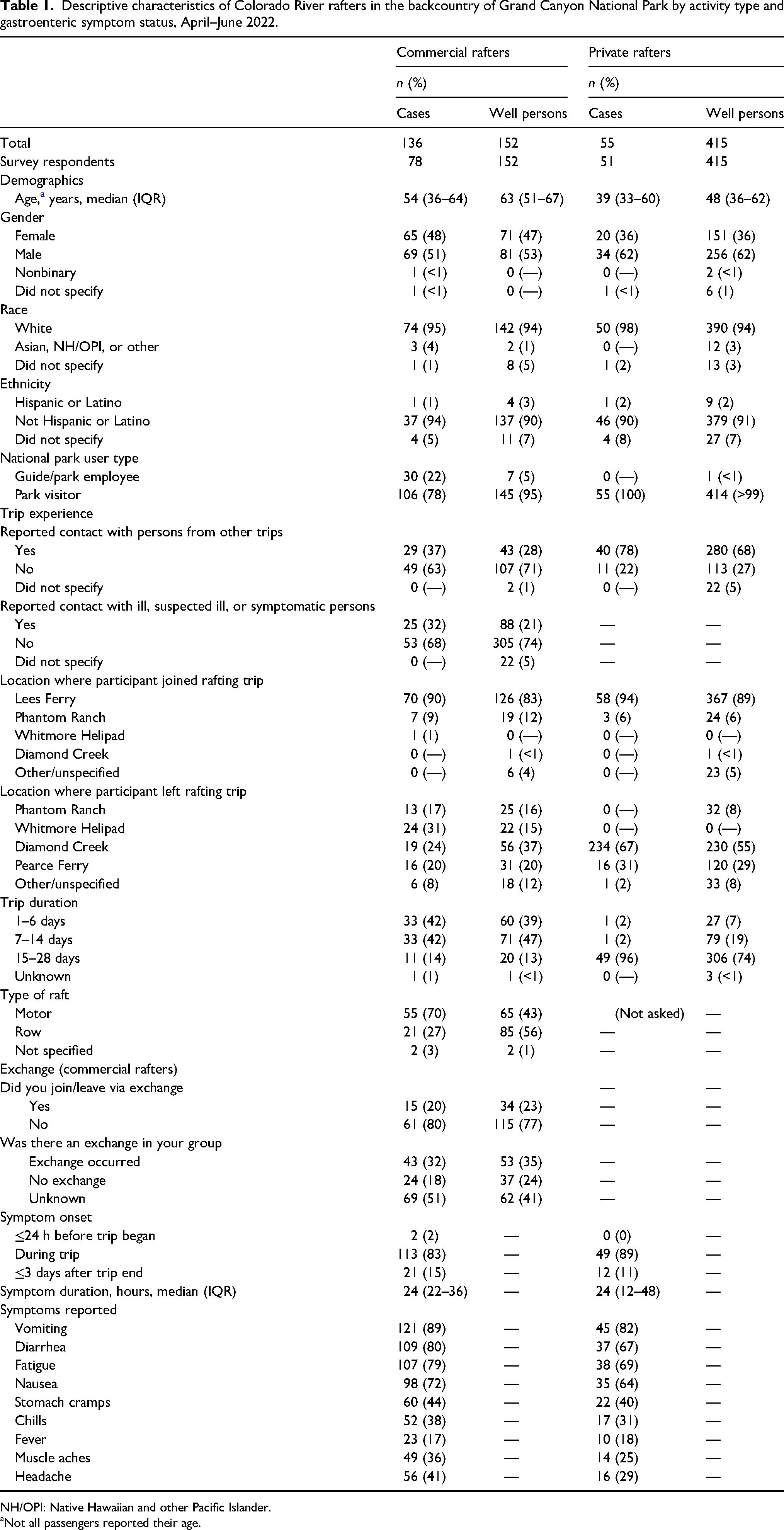
NH/OPI: Native Hawaiian and other Pacific Islander.
Not all passengers reported their age.
AGE onset was reported from April 4–June 8, with 5 (4%) of the 191 total cases reporting onset after May 22 (Supplemental Figure 2). Most cases occurred among park visitors (161; 84%) and the remaining (30; 16%) among professional guides. AGE onset was geographically widespread (122 [IQR: 82–183] miles from Lees Ferry) and occurred a median of 7 days (IQR: 4–10) into the rafting trip. Potential exposure locations occurred throughout the river corridor, including multiple popular attraction sites (Supplemental Figure 3). Symptoms lasted a median of 24 h (IQR: 18–42 h) and were characterized by vomiting (n = 166, 87%), nonbloody diarrhea (n = 146, 76%), and fatigue (n = 145, 76%). Other commonly reported symptoms were headache (n = 72, 38%), chills (n = 69, 36%), and muscle aches (n = 63, 33%) (Table 1).
Univariable Cox regression was used to examine the influence of single characteristics on time to AGE. All characteristics shown in Table 1 were assessed for statistical significance or excluded due to small strata size (n < 5); significant predictors and those of particular interest to the investigation are shown in Table 2. Among commercial participants, younger age groups had higher rates of AGE compared to older groups (<40 y: HR [95%CI] = 1.5 [1.2–1.9] and 1.6 [1.1–2.4] for those 40–59 y, compared to persons aged ≥60 y). Guides (who are concession employees) had higher rates of AGE than visitors (2.2 [1.5–3.3]). Sharing dishes or utensils (1.9 [1.2–3.1]), suboptimal hand hygiene (ie, use of hand sanitizer, wipes, or only water as compared to washing with soap and water) before snacking (1.9 [1.1–3.3]), and known contact with ill persons, such as being on a trip with an ill person or reporting contact with ill individuals from other affected trips (3.0 [1.8–4.8]), were all associated with AGE. Of note, 99% of respondents reported washing hands with soap and before all meals, while only 65% reported doing so before snacks. Among private trips, only contact with ill persons (4.1 [2.2–7.3]) was associated with AGE. No association was identified for specific food or water exposures or for exchanges (eg, being on a trip in which new individuals joined the trip halfway through). There was no difference in AGE occurrence by sex or race/ethnicity. The survival curves in Figure 1 show the timing of illness onset by age and known contact with ill persons. All age groups became ill at around the same rate early in the trip, but younger individuals continued to fall ill later in the trip after cases plateaued in the older age groups. Respondents who reported known interactions with ill persons became ill at a faster rate throughout their trips than those who did not.
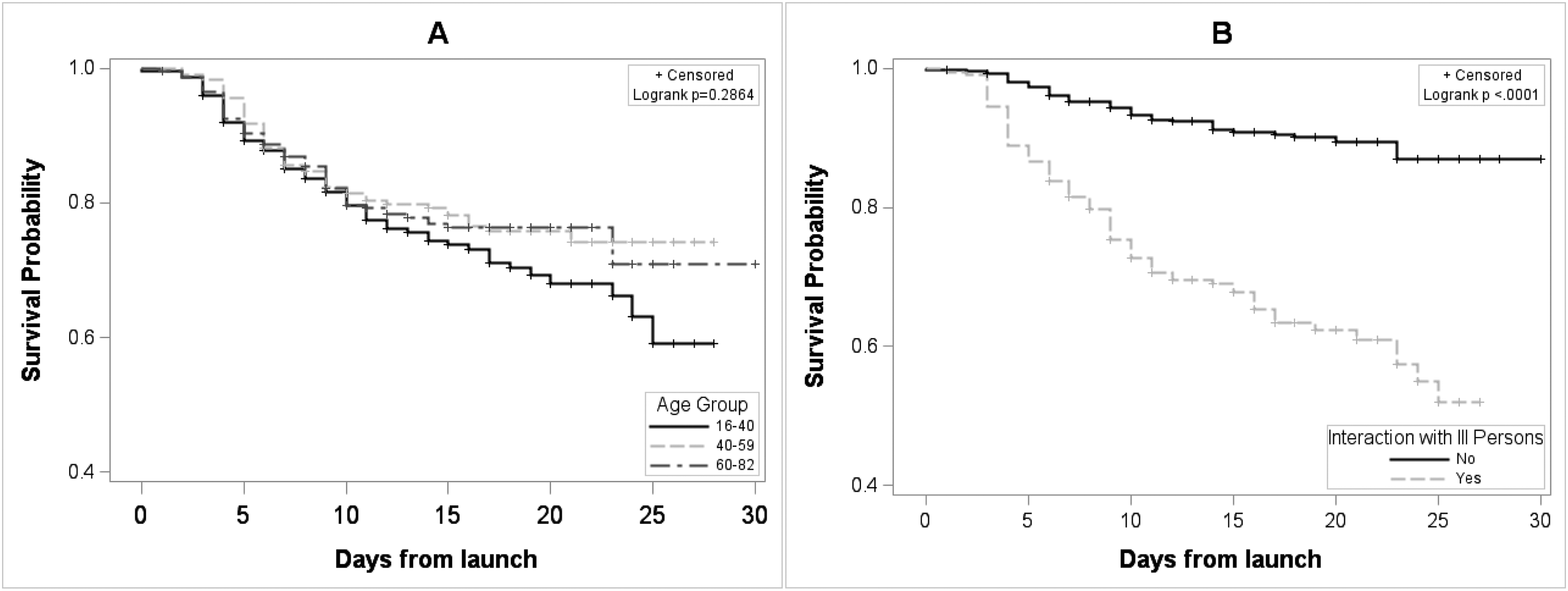
Survival curves* of symptom-free days from trip launch among Colorado River rafters†, Grand Canyon National Park, April–June 2022. A, Age groups; B, contact with ill persons. *Survival time was defined as days from trip start acute gastroenteritis onset. †Persons that remained well >3 days after trip end were censored (not included).
Univariable Cox proportional hazards regression model for the rate of acute gastroenteritis among Colorado River rafters by demographic characteristics and behaviors, stratified by trip type, Grand Canyon National Park, April–May 2022.
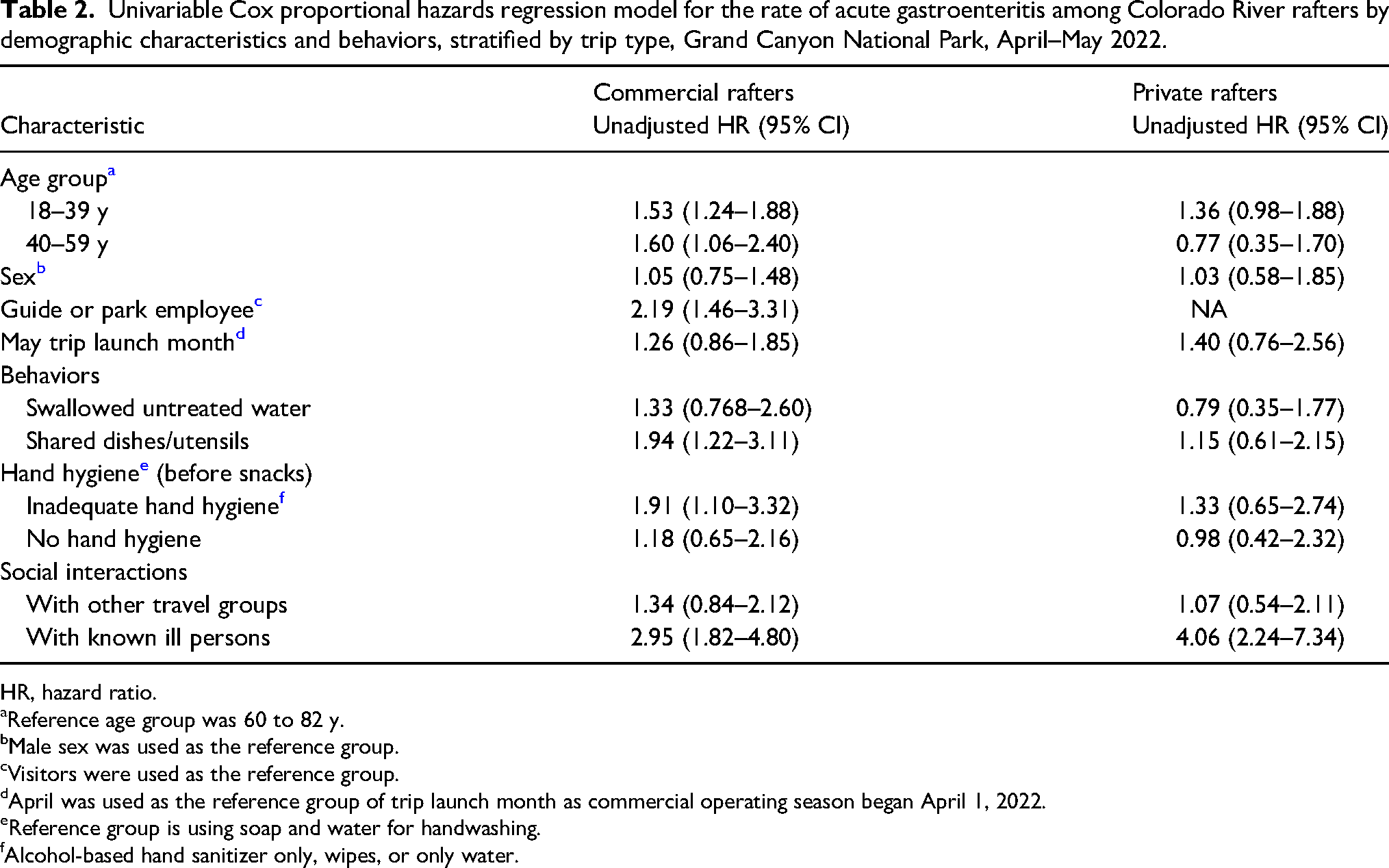
HR, hazard ratio.
Reference age group was 60 to 82 y.
Male sex was used as the reference group.
Visitors were used as the reference group.
April was used as the reference group of trip launch month as commercial operating season began April 1, 2022.
Reference group is using soap and water for handwashing.
Alcohol-based hand sanitizer only, wipes, or only water.
Our multivariable Cox regression analysis included 119 cases and 505 well persons with complete survey data. The final model included age, contact with known ill persons, hand hygiene before snacks, the trip launch month, and whether the trip was commercial or private. Results were like those of the univariate analysis, highlighting contact with ill persons, inadequate hand hygiene, and younger (≤60 y) age being associated with AGE (Table 3). Of note, significant differences in reported behaviors by age group were observed (Supplemental Table 2). When excluding age from the model, sharing dishes remained significant (Supplemental Table 3).
Hazard ratio estimates a from multivariable Cox proportional hazards regression model comparing rates of acute gastroenteritis among Colorado River rafters, Grand Canyon National Park, April–May 2022.
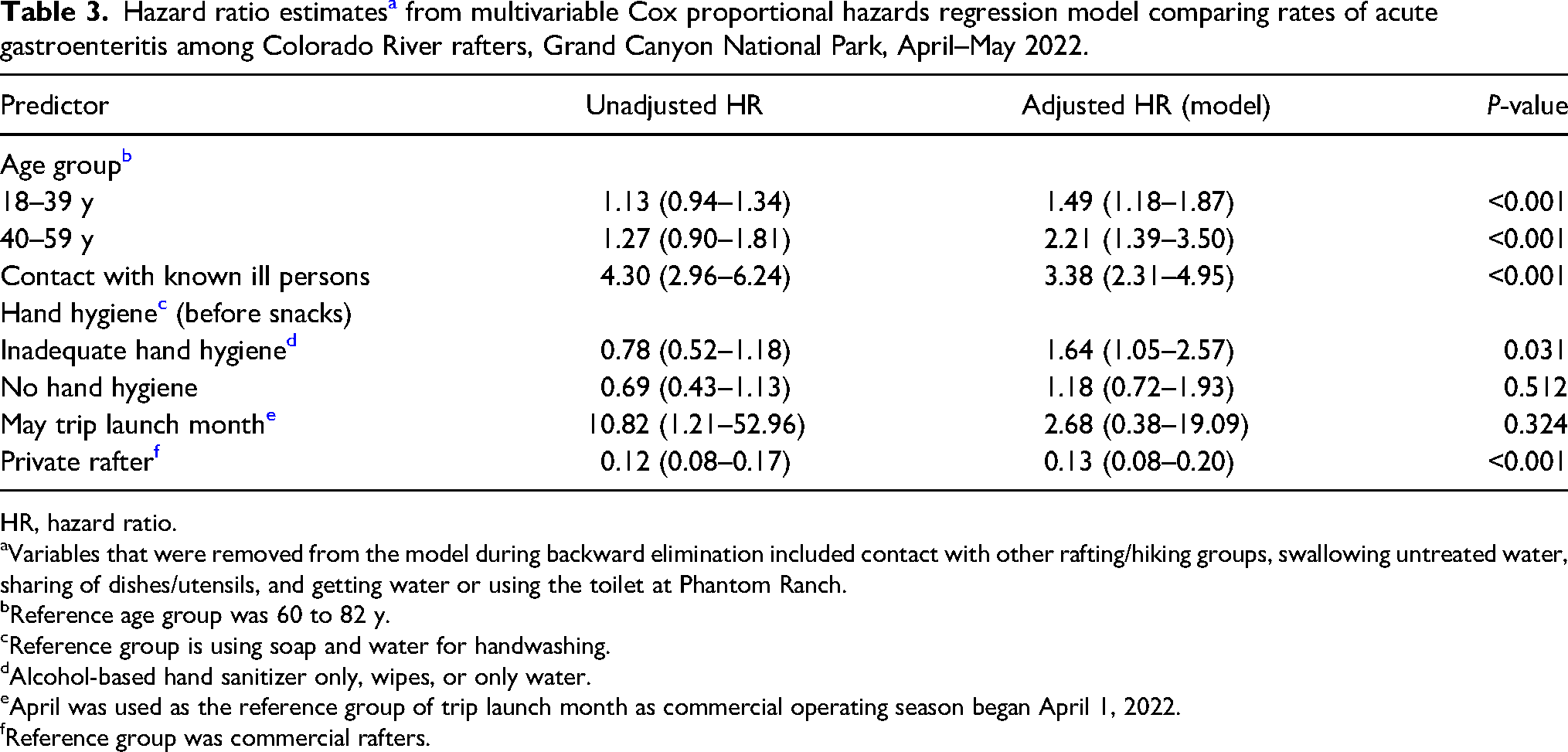
HR, hazard ratio.
Variables that were removed from the model during backward elimination included contact with other rafting/hiking groups, swallowing untreated water, sharing of dishes/utensils, and getting water or using the toilet at Phantom Ranch.
Reference age group was 60 to 82 y.
Reference group is using soap and water for handwashing.
Alcohol-based hand sanitizer only, wipes, or only water.
April was used as the reference group of trip launch month as commercial operating season began April 1, 2022.
Reference group was commercial rafters.
Discussion
Our investigation of the largest AGE outbreak ever documented in Grand Canyon did not implicate a single contamination source but rather known modifiable factors associated with illness spread. Previous outbreaks have been reported among US rafters and river users.13–16 Among those where etiologies were confirmed, norovirus was the primary pathogen. The illness timelines, reported symptoms, and detection of two norovirus genogroups in pooled samples are highly suggestive that norovirus was the primary causative agent in this outbreak. At the time of the investigation, there were increased norovirus cases reported locally and nationally.4,17 Inadequate hand hygiene and contact with ill persons and contaminated high-touch surfaces likely contributed to the escalation of cases. Although our investigation did not find water spigot use or an exchange/camp site to be a statistically significant risk factor for illness, transmission may still have occurred through contact with contaminated high-touch surfaces as groups stop at and camp in the same locations. Extensive person-to-person spread of norovirus may have resulted in short-term contamination of environmental areas where vomitus and stool were not properly deposited or disposed of or where groovers were repeatedly placed at similar locations in campsites. Contaminated equipment such as coolers, personal water bottles, groovers, and other fomites may have also contributed to transmission.
Inadequate hand hygiene was associated with AGE among all rafters. Commercial outfitters are required to provide handwashing setups near camp kitchens and groover areas. The stations must consist of liquid soap and either potable water or water containing at least 100–200 ppm of chlorine bleach, depending on the water source. 8 Many (60%) respondents reported washing their hands before all meals but not before snacks, which for rafters would often be eaten on the river rather than on shore. Even if hand sanitizer was used, alcohol-based hand sanitizer alone is not effective against norovirus.1,5,18 Of note, respondents aged ≥60 y reported better hand-hygiene practices than their counterparts. This is consistent with research that suggests older adults perform more hand hygiene compared to younger age groups.19,20 Our findings underscore the importance of maintaining handwashing with soap and water among all age groups and isolation of ill persons to prevent norovirus transmission.
In our survey, rafters aged ≥60 y made up a large proportion of total cases, but they had a lower attack rate compared to younger respondents. Survey respondents aged ≥60 y reported participating in fewer behaviors associated with AGE exposure like interacting with people outside of their travel group and swimming in or swallowing nonpotable recreational water throughout the canyon (Supplemental Table 2).
Swimming may have been a risk factor since norovirus can be transmitted in recreational waters and environmental surfaces.21–23 Throughout the main canyon there are dozens of side canyons and waterfalls that are popular among rafters. 9 While the main Colorado River current contains a large volume of water that moves quickly down river, the water in the pools found along the trails does not continuously circulate or enter the main current. Thus, the environmental surfaces around the swimming spots may have prolonged norovirus contamination, and physical contact with contaminated beach sand and rocks may have been an exposure source. Norovirus is known for its infectious persistence, up to 2 weeks on environmental surfaces and over 2 months in water, 23 dependent on weather conditions and other environmental factors.
AGE was also associated with sharing dishes or utensils. Survey responses found that rafters often reported traveling with relatives or friends. Persons infected with norovirus shed particles when symptomatic and potentially for weeks after symptoms stop. 23 Norovirus can contaminate a diverse range of fomites, 23 thus sharing personal items with friends or family may contribute to the spread of AGE. NPS river guidelines for washing dishes and utensils include using potable water containing at least 100 ppm of chlorine bleach or river water containing approximately 200 ppm of chlorine bleach, as determined by testing strips with a 10 s contact time, but there are no specific rules on sharing items among group members. 8
To mitigate AGE transmission, there are strict guidelines on rafters assisting in the preparation of food during commercial trips; ill persons are not allowed to prepare food. If a guide develops AGE, they must not handle food or treat water while sick and for at least 72 h after symptoms have resolved. Passengers who experience AGE during a trip cannot assist in the kitchen for the remainder of the trip. If ≥2 passengers become ill on a trip, no passengers may help with food for the trip duration. 8
Finally, on commercial river trips, while guides were more likely to experience AGE than passengers, the data did not support the guides as the source of the outbreak. The increased rates among guides may have been a result of selection bias as guides had a high survey response rate, but they may truly be at higher risk of illness. Guides may act as caregivers to sick passengers and have contact with potentially contaminated equipment like groovers or used dishes. These exposures and activities are like what is seen in household transmission literature, where households with two or more cases are associated with a high secondary attack rate. 24 We noted that all guides had symptom onset after a passenger illness was reported on a trip. Moreover, the rotation time of guides between trips is at least 2 to 3 weeks, and ill guides must sit out the next trip, making it unlikely that a guide was responsible for initiating the outbreak. Further, commercial river guides must go through river apprenticeships, have certificates in food handling and wilderness advanced first aid, and demonstrate a practical knowledge of equipment and sanitation procedures. 8 Notably, survey respondents from commercial trips were complimentary of the way their guides handled hygiene procedures and implementation of infection control practices.
In the past 20 y (2000–2019), among reported untreated recreational water-associated outbreaks with known infectious etiology, norovirus is the most frequent enteric pathogen identified.21,22 Outdoor adventure activities, like whitewater rafting and backpacking, have been associated with multiple outbreaks of norovirus and other AGE. 25 Between 1994 and 2005, there were only 6 published AGE outbreak investigations associated with Grand Canyon Colorado River rafters; 3 could not identify the source. 13 In 2005, sandwich meat sliced by a processing-plant employee after recovering from AGE was implicated in 137 ill persons. 14 A 2012 outbreak among 97 rafters detected norovirus in 2 genogroups from groovers and clinical specimens but not from environmental and fomite samples. 15 Norovirus outbreaks are difficult to prevent and control in general, but transmission in this setting may be increased since hygiene is more difficult and often neglected without running water and toilets. While Heijne et al 26 reported enhanced mitigation measures during a norovirus outbreak at an international scouting jamboree in the Netherlands, including hand hygiene, surface cleaning, and using separate toilets for ill persons reduced spread by 84%, it did not entirely eliminate the spread. This speaks to the remarkable transmissibility and stability of norovirus and may account for a continuous low level of norovirus among the public or within any community.
Limitations
This study has several limitations. First, we were unable to assess statistical significance for several factors due to small strata sizes, particularly among private rafters. The small number of ill backpackers who responded to the survey precluded statistical modeling of hiker data. We were also unable to apply trip-level matching in our analysis of commercial rafters, as we were only able to reach a few unaffected trips. Second, the total number of cases associated with this outbreak is likely underreported among more casual recreators in the park, as an increase in norovirus activity was observed at a national level in spring 2022. 4 There is also the potential for recall bias or misclassification since the survey asked about experiences that took place up to 2 months before the survey was available, and case classification was symptom-based. Third, we were unable to collect clinical specimens from ill individuals for lab confirmation, so we cannot rule out additional pathogens as reasons for symptoms. A 2013 AGE outbreak among rafters in Idaho was attributed to both Giardia and norovirus. 16 Fourth, the detection of 2 norovirus genogroups suggests there were likely multiple introductions of norovirus into the Grand Canyon during spring 2022. Finally, norovirus can spread in multiple ways, and it is impossible to assess all potential sources of contamination in the Grand Canyon.
Conclusions
Norovirus cases are returning to near prepandemic levels, 4 as are Grand Canyon visitation numbers. 6 Therefore, it is likely that there may be future outbreaks among rafters and backpackers in the park. This investigation's recommendations for control and prevention measures remain broad,7,8,10,27 with a focus on public messaging, screening for AGE, surface decontamination, hand hygiene, and limiting contact with ill persons unless as a necessary caregiver. Since AGE prevention and control guidelines are already tailored to this unique environment, interventions for mitigation could focus on modifiable behaviors in patrons like enhancing norovirus education to all backcountry permit holders. Persons could consider taking steps, such as carrying biodegradable soap for handwashing, when possible. Outfitters could consider implementing a pre-arrival symptom screening process and encouraging rebooking for people with AGE onset within 72 h of trip start. Moreover, information including plain language recommendations of isolation and hand hygiene (emphasizing soap and water when available) could be distributed following any illness onset. At the time of this publication, NPS-OPH developed a “Norovirus on the River” handout and web page for outfitters, which includes a description of mitigation measures recommended during an outbreak. 27 Additional signage with information regarding AGE outbreaks could be posted on bulletin boards throughout the park and restroom signs about the importance of proper hand hygiene and reporting illness. During periods of increased AGE, if staffing allows, parks could increase the regular cleaning and disinfection of high-touch points like restrooms, water fountains, and spigots at the launch sites and trail heads to reduce spread. Beyond launch sites, the Colorado River is accessible only by rafting, hiking, pack animal, and helicopter, emphasizing the importance of public health messaging before trip start in addition to existing measures. Despite norovirus's environmental stability and remarkable transmissibility, infection control mitigation measures are effective in other settings and can be readily applied to the wilderness environment to reduce the spread in future outbreaks.
Supplemental Material
sj-docx-1-wem-10.1177_10806032241245093 - Supplemental material for Acute Gastroenteritis Outbreak Among Colorado River Rafters and Backpackers in the Grand Canyon, 2022
Supplemental material, sj-docx-1-wem-10.1177_10806032241245093 for Acute Gastroenteritis Outbreak Among Colorado River Rafters and Backpackers in the Grand Canyon, 2022 by Shanna Miko, Laura Calderwood, Ariella P. Dale, Ronan F. King, Matthew B. Maurer, Maria A. Said, Marette Gebhardt, Laurie P. Dyer, Wendy Maurer, Mary E. Wikswo, and Sara A. Mirza in Wilderness & Environmental Medicine
Footnotes
Acknowledgments
We would like to thank Grand Canyon National Park Leadership, Glen Canyon National Recreation Area, tribal partners, concessioners (including commercial rafting companies), Stefanie Campbell, Shawna Crosby, John Dillon, Conor Fitzgerald, Charles Gerba, Christian Glime, Jake Hojnacki, Nigel Jones, Hasna Karim, Mia Catherine Mattioli, Mary Ellen Ormsby, Elizabeth Richardson, Steve Q. Sullivan, and the Epidemic Intelligence Service Program for their support in this investigation.
Author Contribution(s)
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.