
Abstract
Abstract
Purpose
Titanium elastic nail (TEN) as an alternative to traction and spica cast in preschool children has not been widely studied for its safety and effectiveness.
Methods
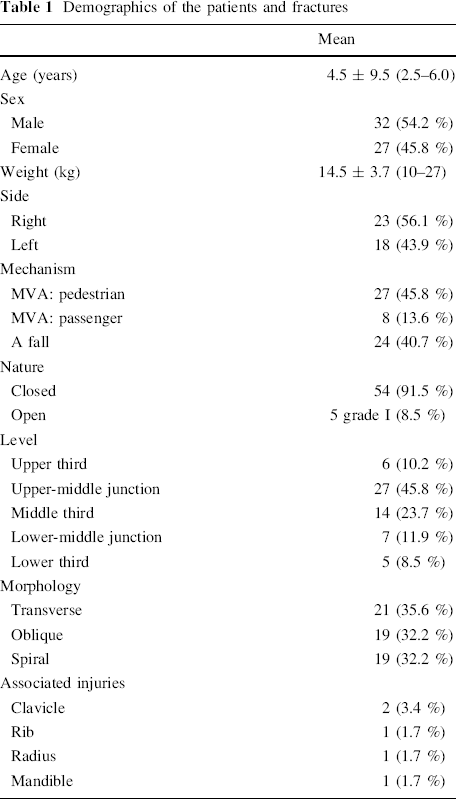
A cohort of 59 children with 59 fractures (non-pathological; not involving condyles or cervicotrochanteric area) were retrospectively examined. Their mean age was 4.5 ± 0.9 years and their mean weight was 14.5 ± 3.7 kg. All but five were closed (21 transverse, 19 oblique and 19 spiral). Thirty-five were caused by motor vehicle accidents and 24 by falls. There were six upper third, 27 upper-middle junction, 14 middle third, seven lower-middle junction, and five lower third fractures.
Results
The mean follow-up was 41.8 ± 4.3 months, the mean hospital stay was 1.3 ± 0.87 days, and the mean time to nail removal was 20.3 ± 10.2 weeks. The mean time to union was 7.6 ± 1.5 weeks. Union was significantly correlated to age (p = 0.000) and fracture shape (p = 0.005), but not to the fracture level, nature, or mechanism. Shortening of ≥1.0 cm occurred in two cases (3.4 %), with an overall mean of 0.06 ± 0.21 cm. Shortening was significantly correlated to the fracture shape (p = 0.020), but not to the level. Overgrowth of ≥1 cm occurred in seven cases (11.9 %), with an overall mean of 0.22 ± 0.41 cm. Overgrowth was insignificantly correlated to the fracture level and shape. Frontal angulation of 5–9° occurred in six cases (10.2 %) and sagittal angulation of 3–7° occurred in seven cases (11.9 %). A rotational deformity of 10° occurred in two cases (3.4 %). Five cases had a painful nail end (8.5 %) and exteriorization with superficial infection occurred in two cases (3.4 %).
Conclusion
TEN is a dependable, safe, and cost-effective alternative to traction and cast in preschool children.
Keywords
Introduction
Femur fracture is among the most common and most disabling injuries in childhood. Many treatment options are reported for school age children [1, 2], but only five papers addressed the problem in preschool children, with three of them about titanium elastic nail (TEN) [3–7]. The treatment options for preschool femur fractures include immediate [8] or delayed spica cast immobilization [9], skin or skeletal traction on a splint [10], plating [11], elastic nail [9], and external fixators. The most commonly used treatment for preschool children are spica cast immobilization and traction. Although these produce very good union rates [2, 10], they mean delayed weight-bearing, late return to school, and impose psychological burden on the child [12, 13]. Among the reported complications are: the usual necessity for repeated adjustment of fragments; cast sores; joint stiffness; compartment syndrome; loss of reduction; shortening; and angular or rotational deformities [10, 14, 15]. The choice of treatment may be influenced by the child age, location and pattern of fracture, and, to a great extent, by regional, institutional, or surgeons’ preferences. This study hypothesized that TEN produces good results in treating femur fractures in preschool children in both the short and the long term and avoids the complications due to traction and spica cast.
Patients and methods
After obtaining Institutional Review Board approval, this non-randomized retrospective study was performed. The study included children with femur fractures treated with TEN between 2000 and 2008. The inclusion criteria were: (1) age below 6 years; (2) closed or grade I open fractures according to the Gustilo classification; (3) 3-year minimum follow-up; and (4) surgery done by the same surgeon (the author) utilizing the same technique. Exclusion criteria were: (1) segmental or type II–IV comminuted fractures according to the Winquist classification; (2) pathological fractures; (3) grades II or III open fractures; (4) fractures involving femoral condyles or cervicotrochanteric area; and (5) solid malunion requiring open correction. Among 243 fractures, only 59 satisfied the inclusion criteria. The included patients’ demographics are shown in Table 1.
Demographics of the patients and fractures
Operative technique
The patient was positioned supine on a standard radiolucent orthopedic table with traction piece and fluoroscopic control. The technique was the standard technique described by Metaizeau [16], with two differences: (1) we utilized a 1-cm incision made by a scalpel inserted directly through the skin, soft tissue, and periosteum 1 cm above the epiphyseal plate under fluoroscopy, and (2) the insertion portal was not made with an awl but with a 3.2-mm drill bit through a drill sleeve, and then enlarged with a 4.5-mm drill bit through its sleeve. The drill bits were aimed at the opposite cortex at an angle of 45°, to make way for the nails. The nail ends were slightly bent at the end of the procedure.
Postoperative management
Postoperative radiographs were requested to check for reduction and nail length. Clinical examination for length discrepancy and rotational malalignment was performed. Stitches were removed after 10 days. Postoperative mobilization was encouraged from the second day. Partial weight-bearing was allowed after 3–5 weeks, according to the stability of reduction, type of fracture, weight, and compliance of the child. Full weight-bearing was allowed after union was achieved. Nail removal was done at least 3 months after surgery.
Follow-up analysis
Follow-up ranged from 36–50 months, with a mean of 41.8 ± 4.3 months. Each patient was seen every 2 weeks until union was achieved, then every 4 weeks up to 6 months, and then every 6 months for 3 years. At each follow-up, we documented the range of motion of the hip and knee, evidence of soft tissues irritation by nail ends, length discrepancy (measured by a tape from the anterior superior iliac spine to the medial malleolus), rotational alignment (by comparing hip rotation to the normal side), exteriorization, infection, gait, and status of weight-bearing. Radiographs were requested to document union, malunion, nail position, and remodeling. Fracture union was defined as the ability to fully bear weight (or resume previous level of activity for non-walkers) without pain in the presence of bridging callus on at least three cortices. Delayed union was defined as the persistence of bone pain and tenderness 3 months after the reduction without complete radiological union. Non-union was defined as absence of osseous union more than 6 months after injury. Nail removal was done when the fracture line completely disappeared on radiographs. Removal was done as an outpatient procedure under general anesthesia or local anesthesia with sedation. The final outcome was graded excellent, satisfactory, or poor based on the Flynn score [17].
Statistical analysis
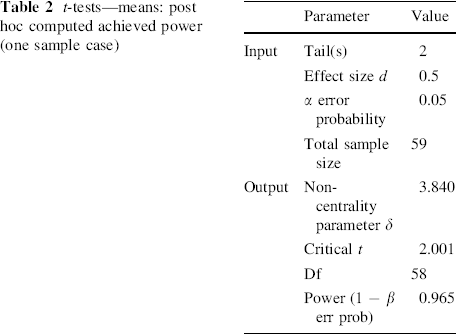
The data are shown in the form of mean ± standard deviation (SD) and range. All statistical analyses were done using the SPSS program (SPSS 15.0, SPSS Inc., IL, USA). Post hoc power analysis was performed using the parameters shown in Table 2 and the statistical power was 96.0 %.
t-tests—means: post hoc computed achieved power (one sample case)
Results
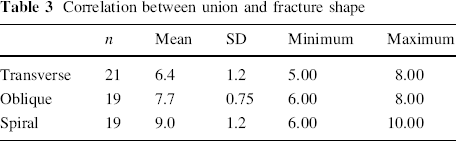
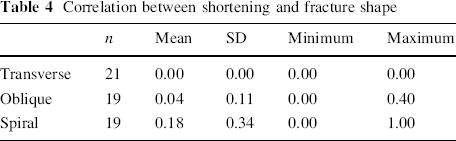
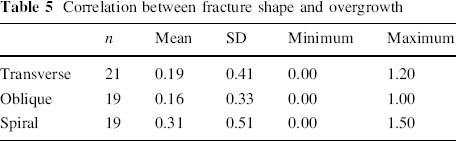
Closed reduction was achieved in 56 cases, while open reduction was resorted to in three cases with soft tissue or bone fragment occluding the medullary canal. Thirty-seven patients were discharged on the same day of surgery. The total mean hospital stay period was 1.3 ± 0.97 days. The time to union (Figs. 1 and 2) was 5–10 weeks (mean 7.6 ± 1.5). Union was correlated to age (p = 0.000) and fracture shape (p = 0.005), but not to the fracture level (p = 0.762), fracture nature (p = 0.689), or mechanism (p = 0.497). Correlation between union and fracture shape is shown in Table 3. Shortening of ≥1.0 cm occurred in two cases (3.4 %), with an overall mean of 0.06 ± 0.21 cm. Shortening was significantly correlated to the fracture shape (p = 0.020), but not to the level (p = 0.520). Correlation between shortening and fracture shape is shown in Table 4. Overgrowth of ≥1 cm occurred in 7 cases (11.9 %). Overgrowth reached its maximum by 18–24 months. Overgrowth was insignificantly correlated to the fracture level (p = 0.204) or shape (p = 0.137). Correlation between overgrowth and fracture shape is shown in Table 5. All patients regained full range of motion of the hip and knee by 16 weeks. We had no refractures or deaths. No patient required revision or repositioning of nails.
An oblique closed mid-shaft fracture in 5.5-year-old boy is shown: 

Correlation between union and fracture shape
Correlation between shortening and fracture shape
Correlation between fracture shape and overgrowth
Complications
Painful nail end occurred in five cases (9.4 %). One of them required trimming of the nail end to relieve the pain. Nail exteriorization with superficial infection occurred in two of these cases and was managed with intravenous antibiotics and dressings, with early nail removal at 13 and 14 weeks, respectively. A bursa over the nail ends at the time of nail removal was found in 35 out of 59 cases. These bursae were clinically detectable at 6–10 weeks and were excised at the time of nail removal. The final results are shown in Table 6. Penetration of the greater trochanter with a nail end occurred in one case (Fig. 1), but with no clinical sequence. Comminution at the fracture site occurred in two cases; one had no clinical sequence and the other had 4° of varus (Fig. 2).
Overall results at 36 weeks follow-up
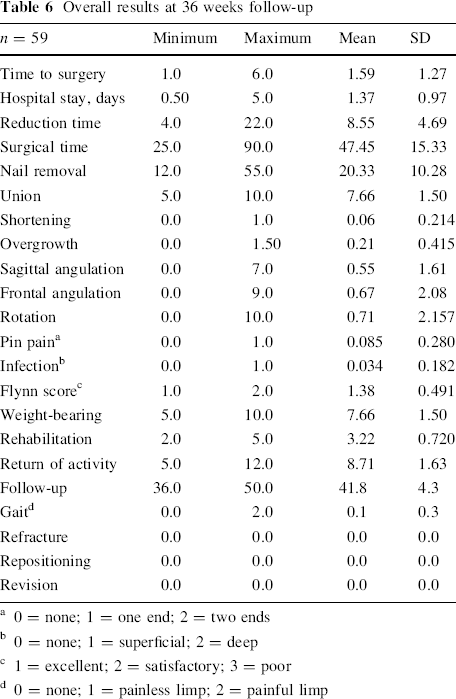
0 = none; 1 = one end; 2 = two ends
0 = none; 1 = superficial; 2 = deep
1 = excellent; 2 = satisfactory; 3 = poor
0 = none; 1 = painless limp; 2 = painful limp
Discussion
Femur fracture is the most disabling fracture in children. Children at school age are treated using various methods, such as compression plating, submuscular plating, locking bridge plates, rigid intramedullary nails [18], stainless steel or titanium elastic nails, and external fixators [19].
Preschool children are usually treated with traction, immediate spica cast, or traction then delayed spica cast. Although they produce very good union rates, their disadvantages include loss of reduction requiring repeated adjustments under anesthesia, prolonged immobilization, high malunion rate, compartment syndrome, and Volkmann's ischemic contracture [20]. The care for the child in spica is particularly troublesome [10, 15].
External fixation has been used in children as young as 3 years of age and, despite the simplicity of its insertion, it is cumbersome and has many complications, such as pin tract infection, which might lead to septic shock [19], limitation of knee motion, refractures of up to 21.6 % [21], ugly scars, and the need to apply plaster spica after removal in some cases [18, 19]. There are no reports of rigid intramedullary nailing in preschool children because of the risk of avascular necrosis of the femoral head and coxa valga [18].
Minimally invasive submuscular and bridging plating for preschool children has been successful [2, 18]. It offers more rigid fixation than flexible nails, which is reflected in easier mobilization and safer weight-bearing. However, it is more invasive and its invasiveness can increase at the time of metal removal, where bony overgrowth may develop over plate ends, which requires open release of plate ends [18, 22]. Formal plating carries the same risks besides blood loss, periosteal stripping which might lead to femur overgrowth, and infection [18].
Elastic stable intramedullary nailing was introduced by Prévot et al. in 1979 [23], utilizing the three-point fixation principle. The technique offers good reduction, dynamic axial stabilization, and early rehabilitation. However, it has many disadvantages, such as length discrepancy, rotational malalignment, malunion, nail exteriorization, and interference with knee motion by the prominent nail ends.
Our surgical time, resorting to open reduction, time to union, incidence of painful nail ends, time to nail removal, rotational malalignment, limb overgrowth, shortening, and angulation are more or less similar to other reported series. Spiral fractures were significantly correlated to shortening (p = 0.020), slower union (p = 0.005), and overgrowth (which did not reach clinical significance).
We had five cases of painful nail ends with exteriorization and superficial infection in two of them compared to nine cases in Bopst et al.'s series [3]. Care should be practiced during the trimming of nail ends at the completion of surgery because too long nail ends lead to soft tissue irritation and a second surgery for retrimming is definitely an avoidable complication. A bursa overlying one or both ends in 35 out of 59 cases imply irritation by the nail ends. There is no mention of bursae in the reported series.
This minimally invasive technique requires short hospital stay compared to other methods of treatment [24], and this series proved that it can be done with minimum hospital stay, as 37 out of 59 children were discharged on the day of surgery.
Preschool children constituted a small number of patients treated in many series, but, to the best of our knowledge, only five articles in the literature have specifically addressed this age group and only three of them were about elastic nailing. The children studied were treated using the one-surgeon–one-technique approach, which would give a better assessment of the results. External fixators were reserved for open fractures of grades II or III (Gustilo's). Plating was also reserved for comminuted fractures where restoring and retaining the femur length would not be feasible with elastic nails and for solid malunion where an open osteotomy is required. A rigid nailing option is not on the table in these young femurs, so we were left with two options for fractures without inherent instability: spica cast and TEN. Our choice of TEN was based on frequent complications of spica cast, lack of ideal cast care in rural communities which constitute the main referral base of our institution, choice by the child's parents, and the better results of TEN compared to spica [25]. We limited our indication to TEN to non-comminuted fractures to avoid collapse at the fracture site with subsequent shortening and angulation, which occurred in 10 out of 15 unstable fractures in Sink et al.'s series [26].
In conclusion, none of the available treatment tools to fix femur fractures in preschool children is perfect because each method has its own set of complications. Complications, however, constitute the motive for developing new techniques or changing the design of currently available devices. We found TEN to be a safe, effective, and cost-effective choice in both the short and the long term if properly chosen for the right fracture in the right patient. It allows early mobilization and weight-bearing, requires minimal hospital stay, is minimally invasive, and is superior to spica in terms of union, rates of malunion, rehabilitation period, and return to nursery. However, it requires an additional surgery for removal and may require trimming of its ends in some cases, and needs modifications in its design and method of insertion to suit more fracture configurations.
Footnotes
The authors did not receive any financial support or benefits from commercial sources for the work reported in this manuscript and do not have any other financial interests that could create a potential conflict of interest or the appearance of a conflict of interest with regard to this work.