
Abstract
Abstract
Purpose
A common treatment for pediatric femur fractures is intramedullary nail (IMN) insertion. Elastic stable intramedullary nails (ESINs) are often used for these procedures in heavier patients, but the potential for complications and malunion is greater. We describe here a rigid IMN specifically designed for adolescents, the adolescent lateral entry femoral nail (ALFN). The purpose of this study was to compare the recovery and complications for patients treated with ESINs to those treated with the ALFN.
Methods
Our study design was a retrospective cohort study. We performed a review of medical records of 22 children ages 10–17 requiring surgical fixation of a femur fracture for a 2½-year period. Patients selected for the study had traumatic diaphyseal femur fractures and were treated with ESINs without end-caps or ALFNs. Our analyses evaluated injury, surgical, and outcome information for all patients.
Results
Twenty-two patients were eligible for inclusion and were divided into two groups according to their treatment: the ESIN group with 7 patients and the ALFN group with 15 patients. We then performed a comparison of complications and recovery for these patients. The mean time to full weight-bearing was significantly less for the ALFN group (4.1 weeks; SD, 2.2), than the ESIN group (9.4 weeks; SD 3.9). There was no statistical difference in the incidence of major or minor complications.
Conclusions
Older, heavier pediatric patients treated for femur fracture with ALFNs had a shorter recovery time than similar patients treated with ESINs. However, the outcomes for both groups were satisfactory.
Keywords
Introduction
Treatments for pediatric femoral fractures usually result in satisfactory outcomes. In general, the patient's age dictates the treatment of choice. The very young often undergo non-surgical management consisting of a spica cast [1, 2]. In older children, surgical management of the fracture may be indicated and includes retrograde insertion of ESINs, open reduction and plate fixation, submuscular bridge plating, external fixation, and antegrade trochanteric entry nails [1, 3–5]. Insertion of retrograde ESINs is one of the least disruptive to soft tissues of these treatment options, and therefore is often preferred because of the high incidence of bone union along with decreased recovery time and low occurrence of complications [6, 7]. In recent years there has been a decline in the use of spica casting in children 6 years and older, with a concomitant increase in use of ESINs for the same age group, likely because when intramedullary nailing first gained popularity in North America, there were no satisfactory rigid nails available for children or adolescents. However, although ESINs are the standard of care for most uncomplicated pediatric femoral fractures, they do have limitations.
Because of the flexible nature of these nails, they may not provide adequate stability when older or heavier patients are treated with ESINs, resulting in an increased incidence of malunion and other complications [1, 8, 9]. One contributing factor to these complications is the increasing weight of the pediatric population. In one multi-center study, the incidence of experiencing a poor outcome was five times greater in heavier patients [10]. The use of end caps or locking screws with ESINs has recently been shown to reduce complications [11–13]. Some authors state that failure of ESINs is often due to incorrect insertion or inappropriate use [14, 15]. Other groups have used stronger nails designed for antegrade insertion through the piriformis fossa. These larger antegrade entry femoral nails allowed for lower complication rates and less time to weight-bearing ambulation, but in skeletally immature patients, there existed the potential for disruption of the blood supply to the femoral head, leading to avascular necrosis (AVN), which results in irreparable damage ultimately requiring a hip replacement. In addition, the anatomic position of the piriformis fossa causes greater difficulty in insertion of the nail, especially in overweight patients, due to the greater soft tissue mass [16–18]. An alternative insertion site is the lateral surface of the greater trochanter, which is more easily identifiable and accessible than the piriformis fossa, especially in overweight patients when in the supine position. Figure 1 is a schematic diagram showing the lateral insertion point for antegrade nailing with the ALFN [19]. In addition, the sites of other common insertion points are shown in Fig. 1, Panel a.
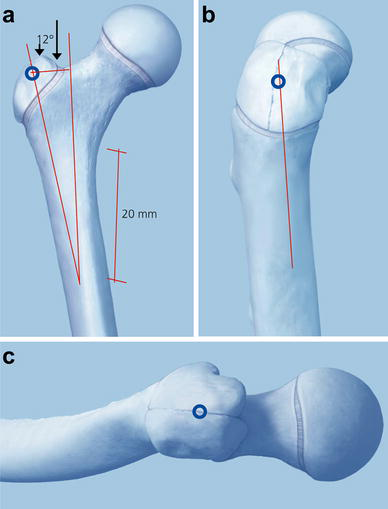
Illustration of the insertion site for the ALFN, which is 12° lateral to the tip of the trochanter, as measured from a point 20 mm distal to the lesser trochanter.
Recent investigations have shown that insertion of IMNs through the greater trochanter leads to high union rates and low incidences of complications, in addition to greater ease of use [16–18, 20–22]. In contrast, one investigation found similar complication rates and recovery for patients treated with flexible nails compared to those treated with rigid nails [23]. However, most IMNs intended for antegrade insertion were designed for entry through the piriformis fossa, and because of the dual curvature of the femur, insertion of these IMNs through the greater trochanter can also lead to complications including malreduction and iatrogenic fracture during insertion [24, 25]. These problems can be avoided by using an IMN specifically designed for insertion through a point on the lateral surface of the greater trochanter and to follow the intramedullary canal, which has been shown to exhibit a helical shape [24, 25]. These ALFN devices are designed to promote ease of insertion through the helical design, shaped to follow the anatomic curvature of the femoral intramedullary canal and reduce the rate of complications including malunion or iatrogenic fracture during insertion or removal. The use of the lateral entry point prevents incidence of AVN by avoiding potential disruption of the blood supply and promotes ease of insertion, especially in overweight patients. In addition, because these nails are interlocking, the stability is greater than for standard ESINs, allowing successful use for heavier patients, while still enabling minimally invasive insertion.
Recent studies showed the effectiveness of using rigid intramedullary nails inserted laterally to the greater trochanter for treatment of femur fractures in adults [16–18]. Furthermore, rigid IMNs inserted laterally to the greater trochanter tip have been used successfully for treatment of pediatric femur fractures, but these were modified nails, not designed for this purpose or point of entry [20, 26–28]. There is limited evidence in the literature supporting the use of rigid nails for pediatric femur fractures [29], as shown in the recent AAOS practice guideline summary [30]. We describe here an exploratory investigation of the use of a new lateral entry intramedullary device specifically designed for treatment of femoral fractures for adolescent patients weighing more than 45.5 kg (100 pounds) that results in satisfactory union with a minimally invasive insertion procedure.
The objective of this exploratory study was to determine if use of the titanium cannulated adolescent lateral entry femoral nail (ALFN; Synthes, Westchester, PA) for fracture treatment of children aged 10 years and older results in good patient outcomes with satisfactory bone union/fracture alignment, short patient recovery times, and low complication rates, including AVN and malunion.
Materials and methods
After approval by the Institutional Review Board, a retrospective cohort study of surgically treated femur fracture patients was undertaken. All patients who underwent intramedullary nail insertion by one of three attending surgeons for treatment of a femoral shaft fracture during the 2½-year period between 1 July 2006 and 23 January 2009 were considered for inclusion. A total of 65 patients at our institution underwent intramedullary nail insertion during this time period. The decision to use the ALFN for treatment was based upon fracture stability and comminution. End caps were not used on the patients included in this study.
Children and adolescents meeting the following criteria were included: (1) having a femur fracture, (2) aged 10–17, and (3) intramedullary nail insertion performed. Criteria for exclusion from the study were: (1) aged 9 years or younger, (2) fracture caused by pathological bone disease or neuromuscular disease, (3) prior, concurrent or subsequent treatment of the same fracture with a spica cast, (4) femur fracture outside of the diaphysis, (5) femur fracture sustained as part of limb shortening surgery, and (6) patients who concurrently sustained a severe head injury that would affect their recovery. Patients were followed at least until full weight-bearing status was achieved and clinical union of the fracture site was observed. Weight-bearing status for the ALFN patients was allowed as tolerated based upon pain. Weight-bearing status for ESIN patients was determined by fracture stability and the level of bony callus formation, and was allowed upon initial formation of bony callus, as determined by the treating physician. Full weight-bearing status was considered achieved when recommended by the treating physician. Patients with less than 2 weeks follow-up were considered lost to follow-up. After exclusions, a total of 22 patients were eligible for the study with adequate follow-up time.
Fractures were classified by R.A.K.R. from radiographs taken at the time of injury using the AO Foundation software program, AO COIAC Comprehensive Injury Automatic Classifier Pediatric Long Bone Fracture Documentation Database [31] (www.aofoundation.org/aocoiac). Fracture alignments were determined from the radiology reports both immediately after fixation and at last follow-up. Malunion was defined according to the published literature as follows: coronal angulation >10°, sagittal angulation >15°, or an axial rotation >10° [7, 16, 32]. Axial rotation was measured both by physical exam, evaluating internal and external rotation of the hip compared to the contralateral side, as well as by radiological examination of cortical mismatch, evaluating the relative position of the lesser trochanter in relation to the knee, as viewed on anterior/posterior (AP) radiographs.
The patients’ medical records were examined for patient demographics, information regarding patient recovery and outcomes, as well as surgical and injury information. The mechanism of injury and associated injuries were documented. Operative and recovery information, including time to weight-bearing, which we define as full weight-bearing status, and incidence of and time to nail removal, were noted. The incidence of minor and major complications was also recorded. For ALFN patients, radiographs at final follow-up were reviewed by R.A.K.R. to confirm there was no evidence of AVN at that time.
SPSS Version 17.0 was utilized to perform all statistical procedures. To examine proportional differences between study groups non-parametric Fisher's exact chi-square tests were performed. Similarly, to examine mean differences between study groups, parametric independent sample t tests were performed. In the cases that assumptions of normality and/or homogeneity of variance were violated, non-parametric Mann-Whitney U tests were substituted. Statistically significant differences were considered achieved at a p value ≤0.05, two-tailed. Sample Power Version 2.0 was employed to calculate sample size and power. Standard deviations, when shown, are noted in parentheses after the mean value of the variable being discussed.
The Institutional Review Board reviewed and approved the protocol for this research study. Food and Drug Administration clearance for use of the ALFN was granted in 2007.
Results
During the 2½-year study period, 22 patients qualified for inclusion in the study. Of these patients included in the study, 18 out of 22 (81.8 %) were male, the average age of the enrollees was 12.7 years, and the average weight was 55.4 kg (Table 1). The gender for the two groups was similar, 100 % of ESIN patients in this age group were male, and 73.3 % of ALFN were male (Table 1). The age ranges for the two groups were also similar, but the mean ages were different (Table 1, non-parametric Mann-Whitney U test, p = 0.035). When the weights for the two groups were compared, they were similar, with an average weight for the ESIN group of 46.4 kg, while the ALFN group weighed an average of 59.6 kg, a difference that was not statistically significant (Table 1, non-parametric Mann–Whitney U test, p = 0.084).
Characteristics of older surgically-treated femur fracture patients (n = 22)
Non-parametric Mann-Whitney U test
Pearson's χ2 test
We recorded the mechanism of injury for all patients, the most common of which was a motor vehicle accident (MVA) (36.4 % of all patients). Other mechanisms of injury included contact sports, fall, and pedestrian versus auto accident, and are consistent with findings from other investigations [15, 33].
The occurrence of other injuries in addition to the femur fracture was rare, with most patients (70.3 %) sustaining no other injury. The most common associated injury was a closed head injury, with 21.6 % of all patients suffering from this associated injury. The fractures were classified according to the AO Foundation Pediatric Long Bone Classification system [31] and were statistically similar for both groups. According to this classification system, the fracture morphology for half (50.0 %) of all of the patients was complete, transverse <30°, and 59.1 % of the fractures were classified as simple in severity.
Information about the patients’ surgeries and recovery were assessed and are summarized in Table 1. Time to weight-bearing for all patients was, on average, 5.8 weeks (SD, 3.8) from the time of the injury. Upon evaluation of difference between the two groups for the patients’ time to full weight-bearing, we found that patients in the ESIN group experienced a longer time to full weight-bearing, with an average of 9.4 weeks (SD, 3.9) post-treatment, while patients in the ALFN group progressed to full weight-bearing an average of 4.1 weeks (SD, 2.2) after surgery, as shown in Table 1 and Fig. 2. This difference was significant (non-parametric Mann-Whitney U test, p = 0.005). The operative time for fixation of the fracture and insertion of the nail(s) was an average of 124.1 min (SD, 37.4 min). The average length of follow-up was 40.2 weeks overall (S.D., 22.9) and similar for the two groups (Table 1).
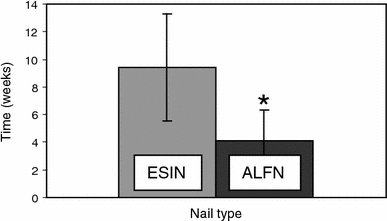
Average time to weight-bearing. Graph illustrating the average time in weeks to achieve full weight-bearing status for elastic stable intramedullary nail patients (ESIN) and adolescent lateral entry femoral nail patients (ALFN). Bars indicate standard deviations. An asterisk (*) indicates a statistically significant difference (p ≤ 0.05)
We noted the incidence of minor (pain/implant pain/irritation, superficial infection, trochanteric heterotopic ossification, delayed union) and major [malunion, limb length discrepancy (LLD) greater than 2 cm, deep infection, AVN of the femoral head, refracture] complications, also shown in Table 1. The minor complications that occurred were primarily pain, implant pain or irritation, with 59.1 % of all patients reporting this complication. The incidence of major complications was also noted, with 4.5 % of patients (1 patient experienced a deep infection) experiencing a major complication (Table 1). Finally, none of the patients included in the study was found to have AVN.
Discussion
In the past, children with femur fractures were treated with a spica cast for young patients or an external fixator for adolescents. Although children under 6 are still treated with spica casts or external fixators [32], the use of external fixators for older children has fallen out of favor, and recently, the standard of care for most pediatric femur fractures has been the use of ESINs, whether stainless steel or titanium. This is largely because the procedure is minimally invasive and usually results in satisfactory outcomes. However, an increased complication rate has been shown to be a consequence of use of flexible nails in older and/or heavier patients [1, 34]. This finding is particularly relevant today, as the percent of overweight children is greater than in the past, especially in urban regions. The purpose of this study was to determine whether use of the ALFN in older and/or heavier patients would result in satisfactory patient recovery while avoiding the occurrence of serious complications such as AVN of the femoral head, leg length discrepancy, and malunion.
We present here an exploratory study that shows that surgical fixation of femur fractures with ALFNs in older and heavier patients results in shorter recovery time than in a similar group of patients treated with ESINs. Although the patients in the ALFN group were older and slightly heavier on average, this difference was expected, since the ALFN was specifically designed for older, heavier children. The recovery time for our ESIN patients, although longer than our ALFN patients, was consistent with those in other studies [34–36]. Patients in this study treated with ALFN had a very low rate of complications, with no major complications. The incidence of major complications for all patients in this report is low compared to other published studies of flexible intramedullary nails, interlocking nails, and other fixation procedures [1, 7, 27, 33, 34, 36–38], with only one patient suffering from a deep infection that resolved upon treatment with antibiotics. In addition to demonstrating good patient outcomes with low complication rates, treatment of complicated or unstable fractures with the ALFN results in good alignment with no complications. Although satisfactory outcomes have been achieved with ESINs in complicated fractures, often in these cases the time to complete union is quite long, on the order of 6–10 months [39]. Furthermore, the patients in this case series were an average of 8.7 years old, an age that has a higher success rate of satisfactory outcomes for femur fracture treatment with ESINs [1, 34]. Similarly, patients with unstable fractures treated with stainless steel elastic nails achieved satisfactory outcomes; these patients were also younger, an average age of 9.2 years [33]. However, in length-stable femur fractures, it has been demonstrated that use of ESINs and rigid nails both result in satisfactory recovery and healing [40]. Often in the past, pediatric patients with comminuted fractures were treated with locking plate fixation, since this treatment provides greater stability than elastic nails or casting, with an average time to weight-bearing of 10.5 weeks, although there are disadvantages to this treatment [41]. One group found lower complications for unstable femur fractures treated with rigid nails inserted at the lateral trochanter [42].
As an example of a severe fracture successfully treated with ALFN, Fig. 3 shows radiographs of a 13-year-old, 58-kg male who sustained a femur fracture as the result of a gunshot wound. The fracture at the time of injury was severely comminuted. As shown in the radiographs taken 17 weeks postoperatively, fixation of this fracture with the ALFN resulted in near anatomic alignment of the fracture. In addition, this patient did not suffer any complications and achieved full weight-bearing ambulation at only 8 weeks postoperatively, a much shorter time than reports of other treatments for complicated fractures. Another example of a comminuted fracture in a younger patient treated with ALFN is illustrated in Fig. 4, which shows radiographs of a 12-year-old, 55-kg male who sustained a femur fracture from a motor vehicle accident. As depicted in the radiographs, the fracture is well aligned at 2 weeks postoperatively, and well-healed with anatomic alignment at 28 weeks postoperatively and after nail removal. Furthermore, this patient did not experience any complications and achieved full weight-bearing ambulation at 6 weeks postoperatively.

Lateral and anterior/posterior radiographs of a 13 year old with a femur fracture caused by a gunshot wound. Radiographs showing a severely comminuted fracture at 2 weeks postoperatively and a well-healed fracture with significant bony callus formation at 17 weeks postoperatively.

Anterior/posterior and lateral radiographs of a 12 year old with a femur fracture caused by a motor vehicle accident. Radiographs showing a comminuted fracture at the time of the injury, and 2 weeks postoperatively, as well as a well-healed fracture at 28 weeks postoperatively, and after nail removal.
Until recently, the options for treatment of femur fractures in older and heavier children have been limited, with risks associated with each option. When ESINs are used, there is an increased incidence of malunion and limb length discrepancy, in addition to pain and irritation at the implant insertion site [1, 34]. The use of more rigid nails designed for antegrade insertion through the piriformis fossa has largely been abandoned because of the potential for AVN of the femoral head, a devastating complication with lifelong consequences [24, 26, 27, 43]. The potential for this complication can be avoided by inserting the nail through the greater trochanter. This method has yielded good results, but most of the studies were performed on adult subjects [16–18, 44]. One study showed that rigid nail insertion through the greater trochanter in adolescents results in satisfactory patient outcomes, although the nails used for this study were designed for insertion through the piriformis fossa [26]. In a case series of 78 patients, the use of a modified rigid humeral nail inserted laterally to the trochanteric tip has been shown to be effective with few complications [27]. Most importantly, in a systematic analysis, it was concluded that an entry point lateral to the trochanteric tip has the lowest risk of AVN when rigid antegrade nails are used to treat femur fractures in children [20]. The ALFN is specifically designed for adolescent femoral fractures, with insertion into the femoral intramedullary canal through a site lateral to the trochanteric tip, and a helical shape that follows the anatomic path of the intramedullary canal [25].
Some limitations of this study include the fact that the time to weight-bearing status is subjective. However, weight-bearing status was determined by the fracture stability, level of bony callus formation, and pain, as recommended by the treating surgeon. In addition, the time of follow-up for these patients averaged 40 weeks, while some complications, as well as bone remodeling, can occur for up to 2 years after the surgical procedure [32]. Although we did not see any evidence of AVN in the ALFN group at the final follow-up visits, we cannot rule out the possibility of this complication appearing after the final follow-up visit. Attempts were made to contact patients for follow-up appointments, but were unsuccessful. In addition, the incidence of AVN is approximately 1–4 %, so we may not detect this complication because of the size of our study group [4, 30]. It should also be noted that while the patients in the ESIN group in this study experienced longer recovery times, all of the patients followed for this study experienced a full recovery, with no functional deficits.
In conclusion, use of a rigid intramedullary nail specifically designed for insertion lateral to the greater trochanter in adolescent patients yields good outcomes in older, heavier patients. Although all of our patients had satisfactory outcomes, our study shows that the use of this device results in faster patient recovery when compared to other accepted treatments for adolescent pediatric femur fractures. Therefore, we recommend further studies to evaluate the safety and effectiveness of the ALFN for treatment of adolescent femur fracture patients.
Footnotes
None of the authors received financial or grant support for this study.
Acknowledgments
The authors would like to thank the AO Foundation for use of their fracture classification software program, AO COIAC Comprehensive Injury Automatic Classifier (AO Clinical Investigation and Documentation, Dübendorf, Switzerland, ![]() ). The authors would also like to thank Synthes, Inc., and its affiliates, for use of images from their technical manual.
). The authors would also like to thank Synthes, Inc., and its affiliates, for use of images from their technical manual.