
Abstract
Purpose
Traditional teaching for fixation of paediatric femur fractures recommends 80% nail diameter/medullary canal diameter ratio (ND/MCD) for successful maintenance of reduction. Prior studies have investigated this with stainless steel Enders nails. Our aim was to assess the impact of ND/MCD on maintenance of reduction and malunion rates in paediatric femur fractures treated with flexible intramedullary nails (FINs).
Methods
Retrospective data was collected on all paediatric patients treated with FINs for diaphyseal femur fractures at a single tertiary care institution over a ten-year period. Patients with co-morbidities affecting bone quality were excluded. Patients were subdivided into groups based on ND/MCD.
Results
A total of 66 patients met inclusion criteria. Mean ND/MCD was 76.3% (32.9% to 98.8%, SD 14.3). In all, 50% (n = 33/66) of patients had > 80% ND/MCD, and only 13.6% (n = 9/66) of patients had less than 60% ND/MCD. When controlling for fracture stability, ND/MCD had no correlation with mean shortening (p = 0.07) There was no correlation between ND/MCD and angulation in the sagittal (p = 0.96) or coronal plane (p = 0.20). Three patients fit malunion criteria. ND/MCD for these patients were 40%, 67% and 79%.
Conclusion
There was no correlation between ND/MCD and shortening or malangulation. The majority of patients in this series with less than 80% fill with FIN healed within acceptable parameters.
Level of Evidence
III
Introduction
The use of flexible intermedullary nails (FINs) for the treatment of paediatric femur fractures is well established. FINs act as an intramedullary splint, providing internal stabilization to the fractured bone while also allowing for earlier ambulation, less angulation and fewer economic and social side effects than alternatives like spica casts, rigid reamed nails or external fixation devices.1–4 Multiple studies have demonstrated high rates of excellent or satisfactory results and low rates of complications necessitating reoperation when FINs are used to fix paediatric femur fractures, particularly in young children with stable fracture patterns.1,4–9
However, significant risk factors for complications associated with FINs include inexperienced surgeons, unstable fracture patterns, higher patient age and higher patient weight.7,10,11 This may be due, in part, to the increased size of older adolescent and obese patients. Traditional teaching recommends a nail diameter to medullary canal diameter ratio (ND/MCD) of 80% for successful maintenance of reduction, a percentage which may be difficult to achieve in larger patients.
Numerous biomechanical studies have analyzed the efficacy of different nail sizes and configurations in maintaining fracture stability. In length stable fractures, the stability of reduction may be improved by higher ND/MCD, although Green et al 12 noted that restoration of alignment was improved with decreased ND/MCD. However, stability may also be affected by method of insertion, location of fracture and numerous other factors. Mehlman et al 13 found that, for transverse fractures in the distal third of the femur, retrograde nailing was superior to antegrade nailing in tests of flexural stiffness. Additionally, Bland et al 14 demonstrated superior bending stiffness using an all-lateral entry technique versus combined lateral and medial entry for simulated oblique and transverse fractures.
Biomechanical studies of length unstable and complex fracture patterns suggest that these fractures may also benefit from increased ND/MCD. Mahar et al 15 found increased torsional and compression stability in comminuted fractures with increasing ND/MCD, with the biggest increase between 67% and 78% fill. Kaiser et al 16 found improved anterioposterior bending, internal rotation and compression stability in spiral fractures fixed with a three-nail model versus the traditional two-nail configuration, but only when the third nail was placed anterolaterally. However, for extremely unstable fractures, especially in larger children, biomechanical studies suggest that locked plating should be considered over FINs, even at 80% ND/MCD, due to superior torsional and compression stability. 17
In the clinical literature, several authors have recommended ND/MCD exceeding 40% for each nail used.6,8,18,19 However, these recommendations are often difficult to generalize due to vast differences in stability caused by different fracture types, patient age and patient weight. Lascombes et al,18,19 in two separate studies, noted an association between decreased ND/MCD ratios and increased complication rates, however, these studies analyzed fractures of the humerus, radius, ulna and tibia in addition to the femur. In a study of 43 femur fractures of varying type Luhmann et al 6 found that increasing nail size was associated with decreased coronal angulation and a trend towards decreased sagittal angulation. In addition, Sink et al 5 found that when the ND/MCD of FINs used to fix unstable femur fractures was < 80%, the complication rate was 35% versus 5% for higher ratios. However, other clinical studies have not found any association between ND/MCD and complication rate when outcomes were controlled for patient weight. 20
Our aim was to assess the impact of ND/MCD on maintenance of reduction and rate of malunion in paediatric femur fractures treated with FINs.
Patients and methods
Institutional review board approval was granted for this study.
All patients with diaphyseal femur fractures treated with FINs between 2004 and 2014 at the Children's Hospital Los Angeles were eligible for inclusion (n = 95). Patients were excluded if they had co-morbidities affecting bone quality, such as osteogenesis imperfecta, mucopolysaccaridoses or dwarfism (n = 9), failed to follow-up until time of radiographic union (n = 14) or had inadequate radiographic documentation of their fracture (n = 6).
Patients were subdivided into groups based on the ND/MCD: < 40%, 40% to 60%, 60% to 80% and 80% to 100%. Percentage ND/MCD was calculated using the width of the canal as measured on a plain radiograph and the size of the nails as recorded in the operative notes.
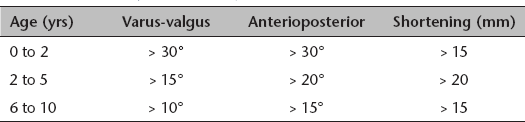
Charts and radiographs were reviewed to determine demographic information, mechanism of injury, fracture type, postoperative complications and fracture angulation and shortening at time of bony union. For the purpose of analysis fractures were characterized as either length stable (oblique or transverse fractures) or length unstable (comminuted or spiral fractures). Complications were defined as painful implants, prominent implants, nonunion, malunion and revision surgery for any reason. Criteria for significant angulation or malunion were defined in accordance with values reported in Rockwood and Wilkins’ Fractures in Children 21 and varied with age (Table 1).
Malunion criteria (data taken from Rockwood and Wilkins’ Fractures in Children, 5th edition 21 )
Statistical analysis
Linear regression was used to determine the relationship between percentage ND/MCD and patient age, patient weight, shortening, sagittal angulation and coronal angulation. Independent t-tests were used to analyze the relationship between fracture stability and shortening or angulation. A chi-square analysis or Fisher's exact test were used to analyze the relationship between percentage ND/MCD groups and development of post-surgical complications.
Results
A total of 66 patients met inclusion criteria. There were 80.3% (n = 53/66) male patients and 19.7% (n = 13/66) female patients. Mean age at time of injury was 6.6 years old (1.8 to 17.7, sd 3.1). Mean patient weight was 25.5 kg (11.1 to 67.7, sd 10.3). The most common mechanisms of injury were: fall (40.9%, n = 27/66), MVA (36.4%, n = 24/66), and pedestrian vs automobile accidents (7.6%, n = 5/66). There were 41 length stable fractures (27 transverse, 14 oblique) and 25 length unstable fractures (21 spiral, four comminuted).
Mean ND/MCD was 76.3% (32.9% to 98.8%, sd 14.3). In all, 50% (n = 33/66) of patients had > 80% ND/MCD and only 13.6% (n = 9/66) of patients had < 60% ND/MCD (Fig. 1).
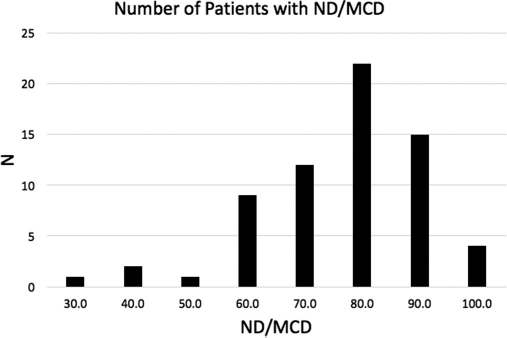
Distribution of patients with given ND/MCD ratios.
Mean shortening was 5.9 mm (0 to 21.7, sd 6.4). Shortening was not correlated with patient age (p = 0.15) or weight (p = 0.06). Length unstable fractures demonstrated significantly more shortening than length stable fractures (unstable = 9.8 mm, stable = 3.5 mm; p < 0.001). When controlling for fracture stability, percentage ND/MCD had no correlation with mean shortening (p = 0.07) (Table 2, Fig. 2).
Variable association with shortening, angulation, and complications
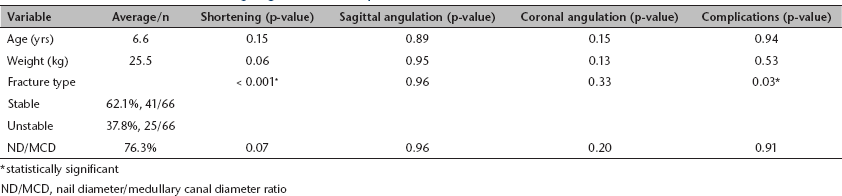
statistically significant
ND/MCD, nail diameter/medullary canal diameter ratio
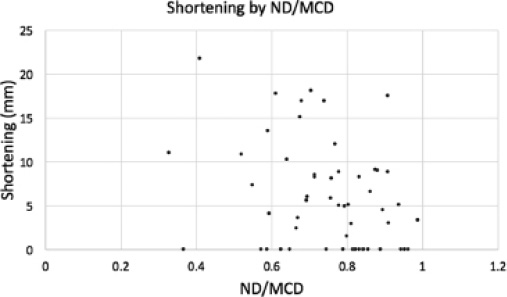
Shortening by ND/MCD ratio.
Mean angulation in the sagittal plane was 4.9° (0° to 16°, sd 4.0). Angulation in the sagittal plane was not correlated with patient age (p = 0.89), weight (p = 0.95), type of fracture (p = 0.96) or percentage ND/MCD (p = 0.96) (Table 2, Fig. 3).
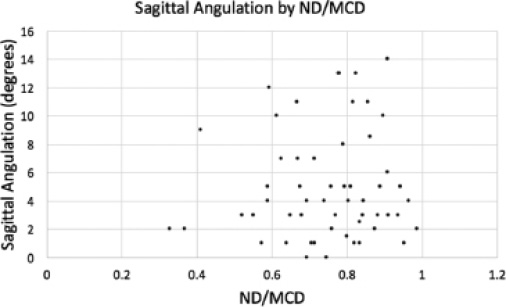
Sagittal Angulation by ND/MCD ratio.
Mean angulation in the coronal plane was 3.3° (0° to 15°, sd 3.0). Angulation in the coronal plane was not correlated with patient age (p = 0.15), weight (p = 0.13), type of fracture (p = 0.33) or percentage ND/MCD (p = 0.20) (Table 2, Fig. 4).
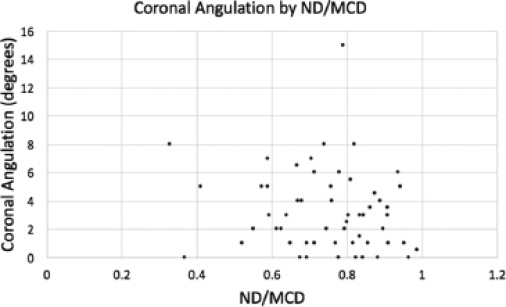
Coronal Angulation by ND/MCD ratio.
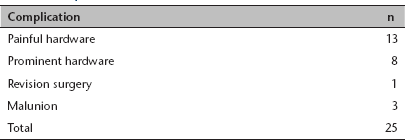
In all, 37.9% (n = 25/66) of patients experienced complications; 13 patients had painful hardware, eight had prominent hardware, three fit malunion criteria and one required conversion to an external fixator due to extreme shortening. Development of complications was not correlated with patient age (p = 0.94) or patient weight (p = 0.53). Length unstable fractures were more likely to develop complications than length stable fractures (unstable = 14/25, 56%; stable = 12/41, 29%, p = 0.03). When controlling for fracture type, percentage ND/MCD did not correlate with development of complications (p = 0.91) (Table 2). ND/MCD for the patients who developed malunions were 40%, 67% and 79%. The patient who required conversion to an external fixator had 80% ND/MCD. For a breakdown of complications see Table 3.
Complications
Discussion
Traditional teaching recommends 80% or greater ND/MCD when fixing paediatric femur fractures with FINs. This has been thought to improve fracture stability and maintenance of reduction, but previous clinical studies have generated mixed results. This study was conducted to quantify the association between ND/MCD and maintenance of reduction in paediatric femur fractures treated with FINs.
Increased ND/MCD did not significantly correlate with maintenance of optimal reductions or complication rate. The majority of patients in this series with < 80% ND/MCD with FINs healed within acceptable parameters. While the overall complication rate in this study was high (37.9%, n = 25/66), there were only four major complications (three cases of malunion and one case of conversion to external fixator due to early excessive shortening).
The most common complications were painful implants (19.7%, n = 13/66) and prominent implants (12.1%, n = 8/66), which is typical of FINs.1,4–11 Although these are ‘minor’ complications in relation to long-term functional outcomes, it should be noted that pain and prominence are not necessarily minor considerations for patients. Reducing postoperative pain should be a goal for all procedures, especially considering the impact pain may have on a patient's quality of life and ability to participate in rehabilitation. In addition, pain and prominence may indicate an undetected telescoping of the fracture due to fracture instability or deficient surgical technique when placing the nails. The presence of excessive pain or prominence warrants careful examination for possible causes, included failed reduction.
Although biomechanical studies on femur models fixed with FINs showed increased stability at higher ND/MCD, this did not seem to translate to clinical practice.12–16 Our results are consistent with data published by Canavese et al 20 which found no correlation between nail size/medullary canal diameter ratio and development of complications. One reason for the apparent conflict between biomechanical and clinical studies may be due to the practice of using two or more smaller nails to fix fractures. Green et al. 12 found that higher ND/MCD provided excellent stability at the expense of ease of reduction and thus recommended using multiple nails for the best combination of reduction and stability. All but one (< 40% fill) of the fractures in our study were fixed using two nails. This may have contributed to increased stability even at lower ND/MCDs.
This study is limited by its retrospective nature. Data was dependent on the availability and quality of medical records. However, the reasons for inadequate documentation are multifactorial and therefore it is unlikely that the data was skewed in one direction over another. In addition, the low number of patients with < 80% ND/MCD may have contributed to the lack of significant findings in this study; only 13.6% (n = 9/66) of patients had < 60% ND/MCD. The complication rate in these patients was 33% (n = 3/9) versus 37% and 38% in the higher percentage fill groups. Detecting a statistical difference in complication rates between ND/MCD groups may require a much larger cohort of patients with < 60% fill.
Use of FINs to fix paediatric femur fractures is well established. Prior research, for both FINs and stainless-steel ender nails, has suggested that aiming for 80% ND/MCD can reduce the complications associated with femoral nailing. However, our current study found no correlation between ND/MCD and maintenance of reduction or complication rate.