
Abstract
Abstract
Purpose
There is little information in the literature regarding flexible intramedullary nails (FIN) for treating femur fractures in children with neuromuscular disorders. The purpose of this study is to investigate the outcomes of FIN for femoral shaft fractures in non-ambulatory children with neuromuscular disorders.
Methods
A retrospective review was conducted on patients with femur fractures at a paediatric hospital between 2004 and 2018. Inclusion criteria were femoral shaft fracture treated with FIN. Outcomes were compared between patients with neuromuscular disorders (NM group) and a control group of those without neuromuscular disorders.
Results
A total of 37 patients with 37 femoral shaft fractures were studied (12 patients in the NM group and 25 in the control group). All NM group patients were non-ambulatory at baseline. Fractures were length stable in all 25 patients in the control group and in 2/12 (17%) patients in the NM group. All fractures healed in both groups. Three complications (all nail migrations) requiring reoperation before fracture union occurred in the NM group, yielding a major complication rate of 25% (3/12) in the NM group versus 0% (0/25) in controls (p = 0.03). Angular deformity occurred in 5/12 (42%) NM group patients and 1/25 (4%) control group patient (p = 0.009); none required reoperation.
Conclusion
Femur fractures in non-ambulatory children with neuromuscular disorders can be successfully treated with FIN. Angular deformities are common in this population, but had no functional impact in the non-ambulatory NM group patients. Surgeons must also be vigilant for implant prominence and skin breakdown in these patients.
Level of evidence
III
Keywords
Introduction
Children with neuromuscular disorders such as cerebral palsy or spina bifida commonly have low bone mineral density and are prone to fractures.1–4 The femur is the most common anatomical location of fractures in these patients, and there are significant challenges to the appropriate management of femur fractures in this population.1–4 Nonoperative treatment with casting has been noted to result in high rates of both malunion and pressure ulcers. Nonoperative treatment also requires prolonged immobilization which may further lower bone mineral density and lead to additional fractures. In addition, the presence of contractures may render nonoperative management unfeasible.3,4
Past authors have supported surgical treatment for femoral shaft fractures in children with neuromuscular disorders; operative fixation provides more stable fracture reduction than casting, facilitates earlier mobilization, and is less likely to be complicated by the development of pressure ulcers. 4 Flexible intramedullary nails (FIN) are an established, effective treatment for femoral shaft fractures in neurologically-intact children.5–8 However, there is little information in the literature on the use of FIN to treat paediatric femoral shaft fractures in patients with neuromuscular disorders.
The purpose of this study is to investigate the outcomes of femoral shaft fractures treated with FIN in non-ambulatory children with neuromuscular disorders compared with those in typically-developing controls. We hypothesized that FIN would yield favourable outcomes despite technical challenges in this population.
Materials and methods
Approval was obtained from the institutional review board, and a retrospective review was conducted on patients with femoral shaft fractures at a tertiary care paediatric hospital between 2004 and 2018. Inclusion criteria were: femoral diaphyseal fracture treated with FIN; age < 18 years; and more than five months of follow-up. Medical charts and radiographs were reviewed for information including age, weight, sex, diagnosis of neuromuscular disorder, ambulatory status, fracture pattern, mechanism of injury, treatment, fracture union, reoperations and complications.
Complications were categorized as either minor or major. Major complications were those that required revision surgery before fracture union. Minor complications were those, such as angular deformity, that did not require revision surgery prior to fracture union. Painful or prominent implants that did not require removal prior to fracture union were categorized as minor complications. Angulation was measured as the angle between the anatomical axes of the proximal and distal fracture fragments, and angular deformity was defined as coronal angulation > 10° or sagittal angulation > 15°. Postoperative canal fill was measured on anteroposterior radiographs and defined as the ratio of the sum of the diameters of the FIN to the diameter of the intramedullary canal of the femur.
Patients were categorized into two groups: those with neuromuscular disorders (neuromuscular or NM group) and a control group of patients without neuromuscular disorders. The majority of control group patients were treated with FIN in accordance with the guidelines of the American Academy of Orthopaedic Surgeons 9 (length stable femur fracture, aged five to 11 years and weight < 50 kg), however, some patients aged more than five years were treated with FIN and were included in the control group. 9 Both length stable and length unstable fractures were included in the neuromuscular group given that there are no evidence-based recommendations for using FIN in neuromuscular disorder children. Fracture pattern in the neuromuscular group was categorized as either length stable (transverse or short oblique) or length unstable (comminuted, spiral, long oblique). Long oblique fractures were defined as those in which the length of the obliquity was greater than twice the diameter of the diaphysis at the fracture site.
Statistical analysis
The neuromuscular group and the control group were compared using chi-squared test, Student's t-test and Fisher's exact test. Statistical analyses were performed with STATA software version 14 (STATACorp, College Station, Texas). Statistical significance was defined as p < 0.05.
Surgical technique
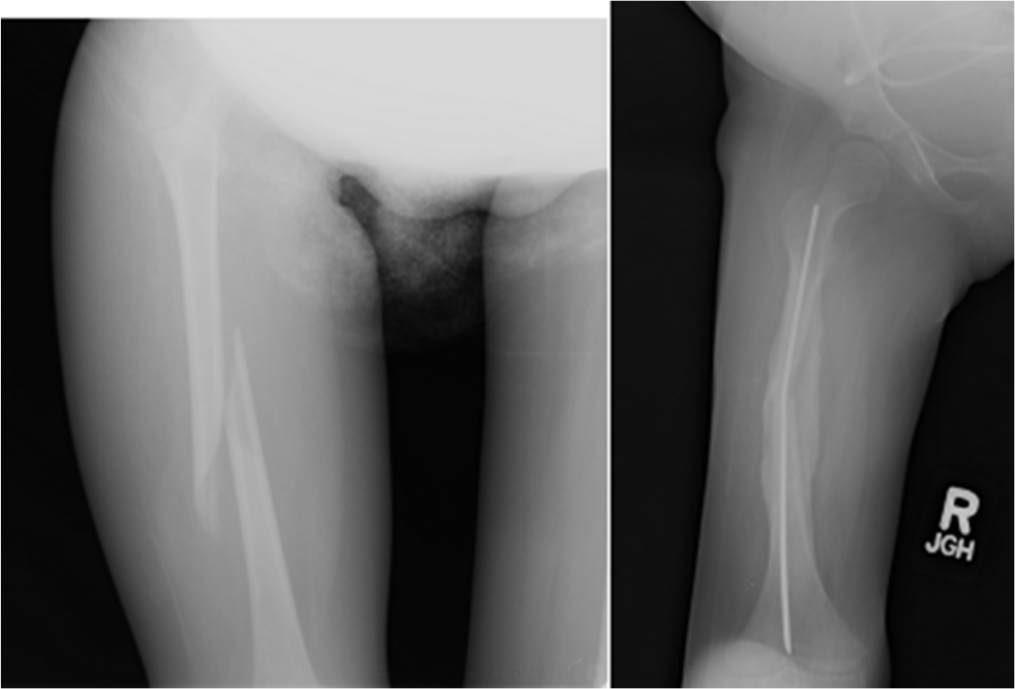
Titanium FIN were used in all patients. The preferred surgical technique for internal fixation using a FIN was similar to that described by Flynn et al, 10 whenever possible. As such, an incision on the lateral distal thigh was followed by obliquely drilling retrograde through the metaphyseal cortex proximal to the distal femoral physis. Two FINs were bent into a C-shape, and one nail was placed through the breached cortex and advanced retrograde. The second FIN was then similarly advanced retrograde. The fracture was reduced and both FIN were advanced across the fracture site. After confirming via fluoroscopy that reduction was achieved and that both FIN crossed the fracture site, the nails were advanced to their final position. The lateral FIN was advanced to the level of the greater trochanteric apophysis while the medial FIN was advanced to either the level of the lesser trochanter or into the distal femoral neck at the discretion of the surgeon. However, this technique is more challenging in children with neuromuscular disorders who often have stiff muscles, poor bone quality and narrow intramedullary canals (Fig. 1). In patients with a very narrow femoral intramedullary canal, internal fixation was achieved using a single FIN if dual FIN could not be placed. The method and duration of postoperative immobilization were at the discretion of the surgeon, and immobilization in this group included spica casting, knee immobilizer, hip-knee-ankle-foot orthosis or no immobilization.

Non-ambulatory eight-year-old male with arthrogryposis who sustained a femoral shaft after a sibling jumped on his leg (left). Operative fixation using two flexible intramedullary nails was performed (middle), with some translation but no angular deformity. Radiographs four months postoperatively reveal healing fracture with satisfactory alignment and no angular deformity (right).
Results
A total of 37 patients with 37 femoral shaft fractures met the inclusion criteria. The neuromuscular group (NM group) was comprised of 12 non-ambulatory patients and the control group had 25 patients. Diagnoses in the NM group were: cerebral palsy (n = 7), spina bifida (n = 3), spinal muscular atrophy (n = 1) and arthrogryposis (n = 1). All cerebral palsy patients were Gross Motor Function Classification System level V. All fractures resulted from either low energy trauma or had no identifiable preceding trauma. Mean age was 9.8 years (sd 3.7; 5 to 17) in the NM group and 5.6 years (sd 2.5; 1 to 11) in the control group (p < 0.001). Mean weight was 26.5 kg (sd 19.0; 12.6 to 81.5) in the NM group and 21.7 kg (sd 8.0; 11.0 to 40.5) in the control group (p = 0.30). Mean follow-up was 32.9 months (sd 28.4; 5.6 to 85.6) in the NM group and 18.8 months (sd 17.3; 6.0 to 81.2) in the control group (p = 0.07).
All fractures in the control group were length stable, compared with only 2/12 fractures (17%) in the NM group (Table 1). All fractures in the control group were treated with two FIN. Within the NM group, operative fixation using two FIN occurred in 9/12 (75%) fractures and 3/12 (25%) were treated with one FIN due to narrow medullary canal diameter. The diagnoses of the patients treated with one FIN were spina bifida (n = 2) and cerebral palsy (n = 1). The mean intramedullary femoral canal fill was 78% (sd 13%) in the NM group and 84% (sd 1.7%) in the control group (p = 0.11). No patient in either group developed a nonunion.
Distribution of fracture patterns in children with neuromuscular disorders
All three major complications in the series involved FIN migration (two of which threatened the skin, and one of which had perforated the skin) and all occurred in length unstable fractures in the NM group, resulting in major complication rates of 25% (3/12 patients) in the NM group and 0% (0/25) in the control group (p = 0.03) (Table 2). Among the NM group patients, the mean canal fill was 71% (sd 9%) in patients that experienced a major complication (n = 3) compared with 80% ± 14% in those who did not have a major complication (n = 9) (p = 0.31). All major complications occurred in non-verbal, non-ambulatory neuromuscular patients with two FIN. Two patients experienced FIN migration resulting in severe implant prominence threatening the skin. Both patients underwent revision surgery for FIN shortening prior to fracture union. One additional patient also experienced FIN migration with resultant skin breakdown and exposed implant. This patient was also treated with FIN shortening prior to fracture union.
Major and minor complications children in femoral shaft fractures treated with flexible intramedullary nails

In all, 17 minor complications that did not require revision surgery prior to fracture union occurred in 17 patients, with minor complications in 5/12 patients (42%) in the NM group and 12/25 patients (48%) in the control group (p = 0.72; Table 2). No patients developed pressure ulcers, neurovascular injuries, or refracture. A total of 11 out of 12 of the minor complications in the control group were symptomatic implants; all cases of symptomatic implants that did not require early revision surgery occurred in the control group and were treated with implant removal after fracture union. There was no relationship between canal fill and minor complications (p = 0.78).
Angular deformity occurred in 5/12 (42%) patients in the NM group and 1/25 (4%) patient in the control group (p = 0.009). Within the NM group, one patient had a coronal plane deformity, two had a sagittal plane deformity and two had angular deformity in both planes. The mean angular deformities in the neuromuscular patients were 12° (sd 4°; 7° to 15°) in the coronal plane and 21° (sd 16°; 16° to 45°) in the sagittal plane. Within the NM group, angular deformity occurred in 3/3 (100%) patients treated with one FIN and 2/9 (22%) treated with two FIN (p = 0.045). Among NM group patients with angular deformities, none had difficulties with hygiene or positioning in a wheelchair or bed due to the deformity. The single angular deformity in the control group was a 14° coronal plane deformity. All angular deformities in both groups were treated with observation and did not require revision surgery.
Discussion
The management of femoral shaft fractures in children with NM disorders is challenging due to unique characteristics of this patient population.1,11 Surgical treatment for these injuries has been described, but the use of FIN has not specifically been studied.1,3,4 This study is the first to describe the use of FIN for the treatment of femur fractures in non-ambulatory children with neuromuscular disorders. Our study found that treatment with FIN lead to successful healing in all neuromuscular disorder patients and avoided the significant risks of nonoperative treatment, but also carried a higher rate of revision surgery than the control group.
There were three major complications requiring revision surgery prior to fracture union in our study, all of which occurred in length unstable fractures in neuromuscular disorder patients, resulting in a 25% rate of major complications in the NM group and 0% in the control group (p = 0.03). The FIN migrated in all three patients with major complications, resulting in prominent implants that threatened the skin and an exposed implant in the third patient. All of these patients required revision surgery to shorten the FIN. These cases highlight the importance of monitoring the nail insertion site for implant prominence postoperatively. Symptomatic implants are the most common complications of femur fractures treated with FIN. 12 Children with neuromuscular disorders often have poor nutritional status resulting in lower body mass and low bone density; decreased soft-tissue around the FIN insertion site coupled with low bone density can predispose these patients to distal rod migration as seen in our study.13,14 Current guidelines advise trimming the inferior aspect of the FIN to ensure that no more than 1 cm to 2 cm of the nail extends beyond the cortex. 10 In children with neuromuscular disorders with limited soft tissue around the nail insertion site, it may be advisable to trim the nails further and/or to consider the use of end caps to prevent implant prominence and skin breakdown.
Additional technical considerations can be examined to potentially optimize the treatment of femoral shaft fractures using FIN in this population. All patients in this study were treated with titanium FIN, however, Rathjen et al 6 reported that stainless steel FIN, which exhibit increased rigidity compared to titanium, yielded superior outcomes with fewer complications and reoperations than with titanium alternatives. Examining whether the subset of children with neuromuscular disorders would similarly benefit from the use of stainless steel FIN would be a worthwhile investigation. Also, all cases of nail migration requiring reoperation occurred in length unstable fractures in the neuromuscular group, however, the low sample size of the NM group, and the fact that only 2/12 fractures in the NM group were length stable, is an obstacle to interpreting these results. Of the ten length unstable fractures in the NM group patients, three (30%) resulted in nail migration which necessitated early reoperation. Further investigation should focus on determining whether the fracture pattern affects FIN outcomes in non-ambulatory patients.
Further, the mean canal fill was lower (71%; sd 9%) in NM group patients who experienced a major complication than those that did not have a major complication (80%; sd 14%); this correlation, however, this did not reach statistical significance (p = 0.31). Achieving a canal fill of < 80% using FIN is associated with a higher complication rate after paediatric diaphyseal femur fractures in neurologically-intact children, but a similar result was not seen in our NM group. 12 The lower canal fill in the NM group may have contributed to the higher complication rate of FIN, and the low sample size of the NM group may be an obstacle to the accurate statistical evaluation of the effect of canal fill on outcomes of FIN. Further examination using a larger sample size on the effects of FIN material and canal fill is warranted to more accurately investigate these factors and guide future patient care.
Symptomatic implants were also seen in the control group; 11/25 patients (44%) in our control group experienced prominent FIN with pain at the distal nail insertion site. However, these can be an ‘expected complication’ with FIN given the high reported incidence in the literature, and none of the patients in the control group required nail removal prior to fracture union. Angular deformity was another minor complication experienced by our patients (Fig. 2). Patients with neuromuscular disorders can have spasticity which exerts significant deforming forces on the fracture fragments; high muscular tone has been shown to facilitate loss of reduction and is associated with a high incidence of malunion.3,4 There was a higher rate of malunion in the neuromuscular group than the control group in our study (42% versus 4%; p = 0.009). Angular deformities occurred in 100% of neuromuscular disorder patients treated with a single FIN, while the prevalence of angular deformity was 22% in those with two FINs (p = 0.045). These results suggest it is highly advisable to achieve internal fixation with dual FINs as opposed to a single FIN, when possible. Unfortunately, placement of dual FINs is often not possible in these NM patients for several reasons: 1) the femoral intramedullary canal of a child may be quite small following years of limited or no weight bearing; 2) bone density is often poor after years of limited weight bearing; and 3) cortices are often quite thin, and passing of significantly contoured FINs may result in cortical penetration and/or fracture propagation (Fig. 3). The incidence of angular deformity in our patients treated with FIN (42%) was comparable with that reported in the literature among patients treated nonoperatively (32% to 52%).3,4 Femoral angular deformities in non-ambulatory children with neuromuscular disorders could potentially interfere with maintaining hygiene or sitting in a wheelchair, however, Leet et al 3 reported that there are few additional functional consequences of angular deformity in this population given their non-ambulatory status. Fortunately, none of our patients had challenges with sitting or hygiene due to their angular deformity. Thus, despite the risk of angular deformity in femur fractures treated with FIN, there may be few actual clinical implications in non-ambulatory paediatric patients with neuromuscular disorders.

Seven-year-old, Gross Motor Function Classification System V male with spastic quadriplegic cerebral palsy who sustained a femoral shaft fracture during physical therapy with his mother (top). He underwent surgical treatment using two flexible intramedullary nails (middle). Final radiographic follow-up nine months postoperatively shows malunion with procurvatum deformity in the sagittal plane (bottom). The angular deformity was treated with observation and had no functional impact on the patient given his non-ambulatory status.
An 11-year-old female who fell from her wheelchair, sustained a femoral shaft fracture, and underwent surgical treatment with single flexible intramedullary nail. Final radiographic follow-up five months postoperatively show abundant callus formation and acceptable coronal alignment.
Communication between providers and patients with neuromuscular disorders, many of whom are non-verbal, may be difficult.1,3 This can lead to the development of pressure ulcers or neurovascular injury in patients treated with casting who are unable to verbally express their pain or discomfort in the cast.1,3,4 Persiani et al 4 reported a 33% incidence of pressure ulcers in non-ambulatory patients treated with casting; they recommended that, due to the lessened risk for pressure ulcers and neurovascular injury, any method of open reduction and internal fixation is preferred over nonoperative treatment for femur fractures in non-ambulatory children. Also, children with neuromuscular disorders are often osteopenic, and casting may necessitate prolonged immobilization which can worsen bone mineral density and lead to additional fractures.15–19 No patients in our neuromuscular group treated with FIN developed a pressure ulcer, neurovascular injury or additional fracture. This provides further support that FIN are a suitable treatment option for femoral shaft fractures in children with neuromuscular disorders. Further, the FINs can provide protection against future fractures; even if fractures occur, the FINs can limit the risk of displacement and need for additional intervention.
The only prior study to describe a comparable method of operative fixation for femur fractures in this population was a retrospective review of four patients treated using FIN in conjunction with external fixation. 11 Kong and Sabharwal 11 asserted that their technique resulted in good outcomes and avoided the risks of nonoperative treatment. However, they strongly cautioned that careful attention to pin site care and cleanliness was imperative to prevent pin tract infection. They noted that a pin tract infection has the potential to progress to deep infection given the presence of an intramedullary implant. One out of four patients in their study developed a pin tract infection requiring oral antibiotic therapy but none progressed to deep infection. Our study shows that fracture union can be achieved using FIN alone for the treatment of femur fractures in children with neuromuscular disorders, thereby avoiding the potentially serious risks of simultaneous external fixation.
Limitations exist in this study. The single centre nature of this retrospective review hinders the generalizability of our results to a broader population. It is well-established that patients with neuromuscular disorders often sustain fractures from lower-energy trauma compared with healthy patients with similar injuries; this difference may be an obstacle to accurately comparing outcomes between groups.1,4,20 There was also no institutional protocol that guided whether patients with neuromuscular disorders were treated surgically or nonoperatively. In addition, there was no standardization of postoperative immobilization, which was left at the discretion of the treating surgeon. Variability in treatment decisions may have caused our NM group to not be representative of the wider population of similar patients with femur fractures. A randomized prospective study could address these challenges and provide further insight on the surgical management of these injuries.
Femoral shaft fractures in non-ambulatory children with neuromuscular disorders can effectively be treated using FIN. Common risks of nonoperative treatment such as pressure ulcers or additional fracture due to prolonged immobility can be avoided by surgical fixation with FIN. Malunion with angular deformity may occur in these patients, but the incidence is comparable with that after nonoperative treatment, and there are few clinical implications of lower limb angular deformity in non-ambulatory patients. Surgeons must be cautious, however, regarding the potential for implant prominence and skin breakdown at the FIN insertion site, especially in nutritionally-deficient children with limited soft tissue around the distal femur.
Footnotes
EMM reports holding stock or stock options in Joint Development LLC, outside the submitted work.
RMK reports holding stock or stock options in Biomet, Johnson & Johnson, Medtronic, Pfizer and Zimmer; is a board or committee member of Commission for Motion Lab Accreditation; son is an employee of Intrinsic Therapeutics; and is on the editorial or governing board of Journal of Pediatric Orthopedics, all outside the submitted work.
AAS and OAA have no conflict of interest.
KDI: Study idea, Study design, Manuscript review, Final approval of manuscript.
OAA: Study idea, Study design, Manuscript review, Final approval of manuscript.
EMM: Study idea, Study design, Manuscript review, Final approval of manuscript.
RMK: Study idea, Study design, Manuscript review, Final approval of manuscript.