
Abstract
Purpose:
To compare the effects of postoperative splint immobilization versus early mobilization on 1-year radiological and functional outcomes in pediatric diaphyseal both-bone forearm fractures treated with elastic stable intramedullary nailing (ESIN).
Methods:
A retrospective analysis was performed on 124 children (6–14 years) who underwent ESIN for closed mid-diaphyseal radius–ulna fractures between January 2018 and December 2023. Patients were divided into splint (n = 64) and non-splint (n = 60) groups according to postoperative protocol. Radiological healing was evaluated using the Lane–Sandhu score at 1, 3, 6, and 12 months, and functional outcomes using the Price classification at 3, 6, and 12 months.
Results:
Baseline characteristics were comparable. At the third month, radiological scores were slightly higher in the splint group, while functional results favored early mobilization, though differences were not statistically significant. By the 6th and 12th months, complete union and excellent functional recovery were achieved in all patients, with no significant intergroup differences (p > 0.05).
Conclusions:
Early mobilization following ESIN is feasible and does not delay bone healing or impair function. Routine splinting may be unnecessary, and postoperative care can be tailored to the patient and fracture characteristics. Moreover, our findings demonstrate that when ESIN principles are properly applied, splint use in appropriately selected patients does not lead to any long-term functional deficit, and excellent outcomes can still be expected.
Keywords
Introduction
Diaphyseal both-bone forearm fractures in childhood account for approximately 3%–5% of all pediatric fractures. 1 These injuries are more frequently observed in school-aged children. 2 In infants, forearm fractures can be managed conservatively; however, with increasing age, the risk of malunion due to rotational and angular deformities rises. 3 Consequently, surgical treatment tends to be favored after the age of 8–10 years. Owing to its minimally invasive nature and the stability it provides, elastic stable intramedullary nailing (ESIN) has become a widely adopted surgical option. Nevertheless, there is no consensus regarding the extent and duration of postoperative immobilization following ESIN. 4 Many centers advocate for splinting to ensure pain control and soft tissue protection. 5 On the other hand, several leading authorities emphasize the importance of early mobilization, highlighting that the stability achieved with ESIN allows for such an approach. 6
In our clinic, the natural variability in practice—where some surgeons prefer 1 month of splinting while others utilize only elastic bandaging—offered an opportunity to compare these two strategies under real-world conditions. The aim of this study was to evaluate the effects of splint versus non-splint protocols on radiological union and functional outcomes in children aged 8–14 years with closed diaphyseal radius–ulna fractures treated with ESIN.
Materials and methods
Study design
This study was conducted in accordance with the principles of the Declaration of Helsinki and approved by the Non-Interventional Clinical Research Ethics Committee of Kutahya Health Sciences University (Approval No: 2025/08-31 / Date: 19/06/2025). Written informed consent was obtained from all participants and/or their legal guardians prior to inclusion in the study. Pediatric patients aged 8–14 years who underwent surgical treatment for diaphyseal both-bone forearm fractures between January 2018 and December 2023 were retrospectively evaluated.
Participants
The study included pediatric patients aged 8–14 years who underwent surgical fixation with ESIN. The inclusion and exclusion criteria applied in this study were as follows:
Inclusion criteria
Age 8–14 years
Closed diaphyseal fractures of both radius and ulna
Mid-diaphyseal location
Transverse or short oblique pattern
Successfully managed with closed reduction + ESIN
Acute fractures operated on within 3 days
Minimum 1-year clinical and radiological follow-up
ESIN principles fully respected on postoperative radiograph
Exclusion criteria
Open fractures
Pathological fractures
Comminuted or segmental patterns
Any case requiring open reduction
Additional trauma to the same upper limb
Prior upper extremity surgery
Incomplete records Follow-up < 1 year
Deviations from ESIN standards on postoperative imaging
A total of 349 pediatric both-bone forearm fractures treated with ESIN were screened, and after applying all eligibility criteria, a final cohort of 124 patients was included in the analysis. The stepwise screening and exclusion process is shown in Figure 1. Patients were subsequently divided into two groups according to postoperative follow-up protocols: the splint group (n = 64) and the non-splint group (n = 60). Baseline demographic and injury characteristics of both groups are summarized in Table 1.
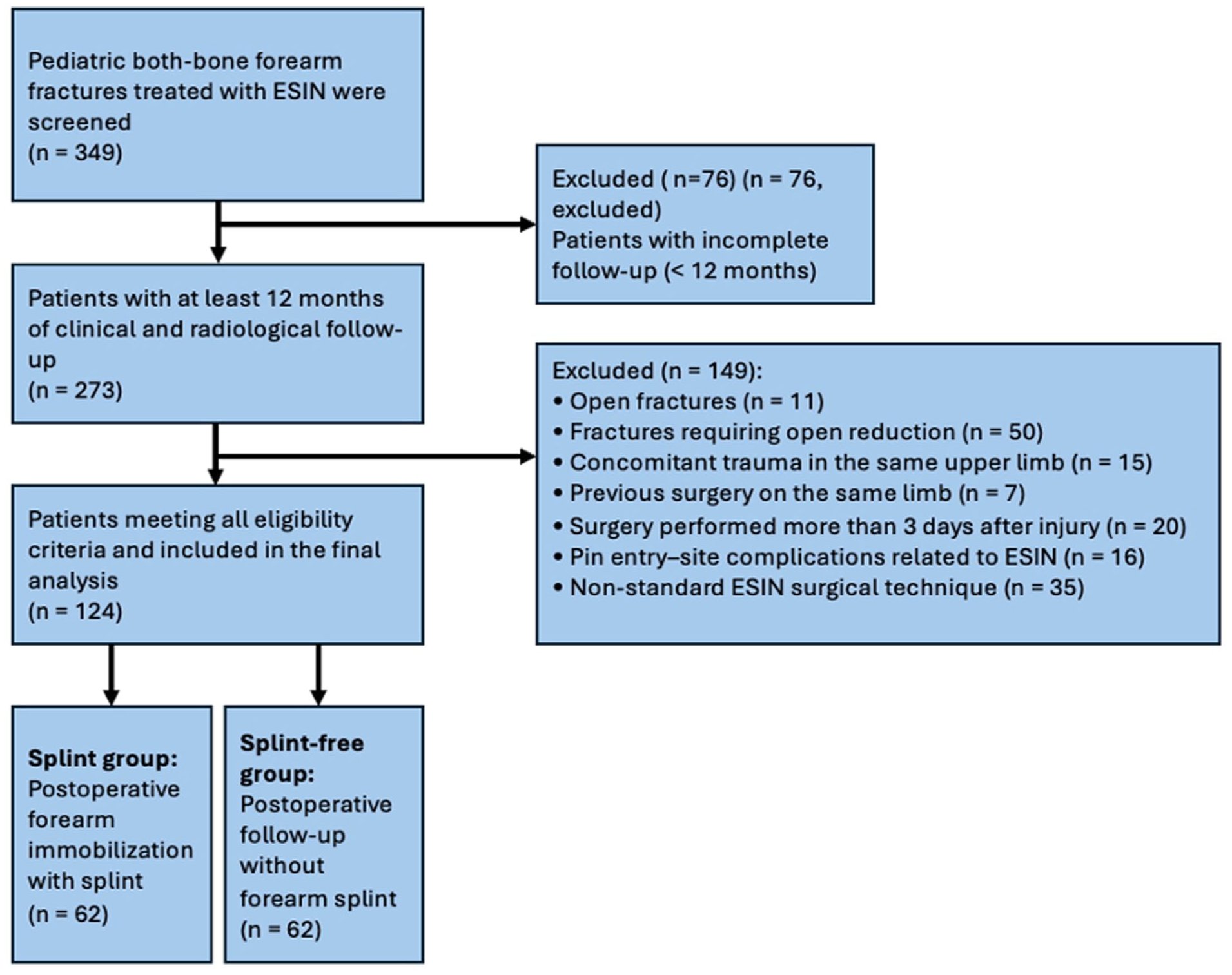
Flow diagram of the retrospective cohort: Screening, exclusion criteria, and allocation to splint and splint-free groups in pediatric both-one forearm fractures treated with ESIN.
Baseline demographic and clinical characteristics of the patients.

SD: standard deviation.
Surgical technique and follow-up
All procedures were performed under general anesthesia. Prophylactic antibiotics were administered before surgery. Fractures were reduced by closed methods, and appropriately sized ESIN implants were inserted intramedullary into both the radius and ulna. Titanium elastic nails (2.0–2.5–3.0 mm) were used in all patients. The diameter of each nail was selected to approximately 40% of the narrowest medullary canal diameter in accordance with standard ESIN principles. The nails were placed without crossing the physis, and their ends were buried subcutaneously. All patients were discharged within 24 h. In the splint group, a long-arm splint was applied postoperatively and routinely removed at the third week, after which all patients were transitioned to a sling. In the non-splint group, patients were followed directly with a sling from the early postoperative period. At the sixth postoperative month, implants were removed under short general anesthesia without complications. Patients were evaluated at 1, 3, 6, and 12 months. Radiological healing was assessed using the Lane–Sandhu score. Functional outcomes were assessed at 3, 6, and 12 months using the Price classification.
Data sources and measurements
All data were obtained from the hospital information system and archived patient files. Radiographs were independently assessed by two orthopedic surgeons, with consensus achieved through a third reviewer if necessary.
Statistical analysis
All data were analyzed using SPSS Statistics for Windows, Version 26.0. Continuous variables were expressed as mean ± standard deviation, and categorical variables as frequencies and percentages. Normal distribution was assessed using the Kolmogorov–Smirnov test. Student’s t-test or Mann–Whitney U test was used for continuous variables, and chi-square or Fisher’s exact test for categorical comparisons. A p-value < 0.05 was considered statistically significant.
Results
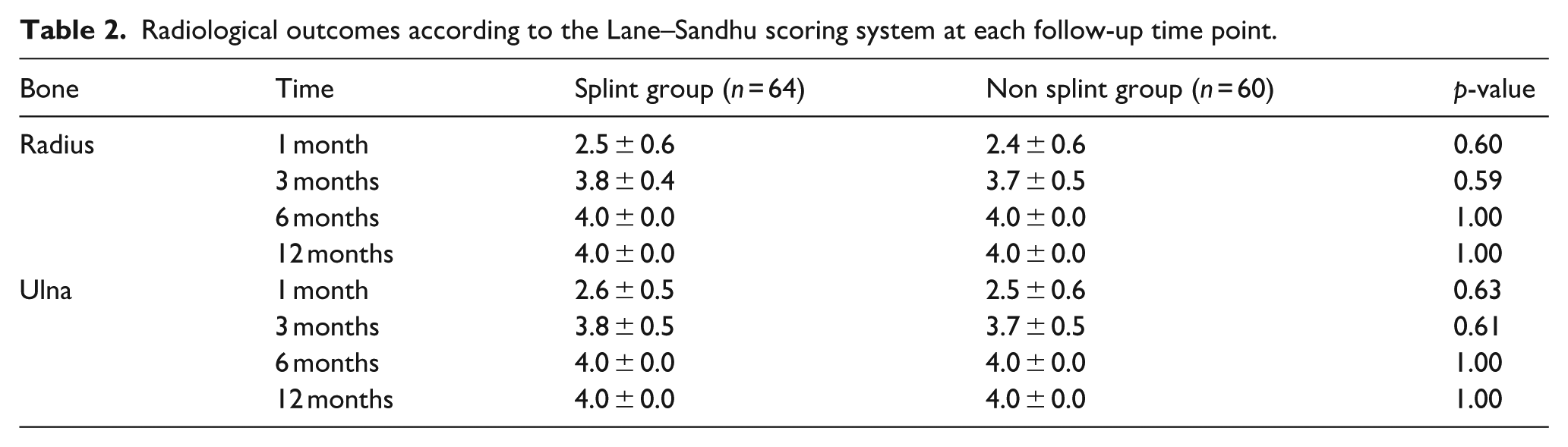
A total of 124 patients were included: 64 in the splint group and 60 in the non-splint group. The groups were comparable in baseline characteristics. Lane–Sandhu scores increased significantly from 1 to 3 months, with complete union observed in all patients at 6 and 12 months. At the third month, scores were slightly higher in the splint group (Radius p = 0.59/Ulna p = 0.61). By the 6th and 12th months, there were no differences between groups (Table 2).
Radiological outcomes according to the Lane–Sandhu scoring system at each follow-up time point.
Functionally, based on the Price classification, “excellent/good” outcomes were slightly more frequent in the non-splint group at 3 months (p = 0.96). No significant differences were observed at later time points (Table 3). No patient required reoperation. Two patients in the splint group were monitored for suspected compartment syndrome, which resolved spontaneously without intervention.
Functional outcomes according to the Price classification at each follow-up time point.

Figure 2 illustrates the progression of Lane–Sandhu scores for radius and ulna fractures in both splint and non-splint groups, demonstrating comparable healing trajectories with complete union achieved by the sixth month in all patients. Figure 3 shows the proportion of patients with excellent or good functional outcomes according to the Price classification, indicating similarly favorable recovery in both splint and non-splint groups by the 3rd month and full functional restoration in all patients by the 12th month.
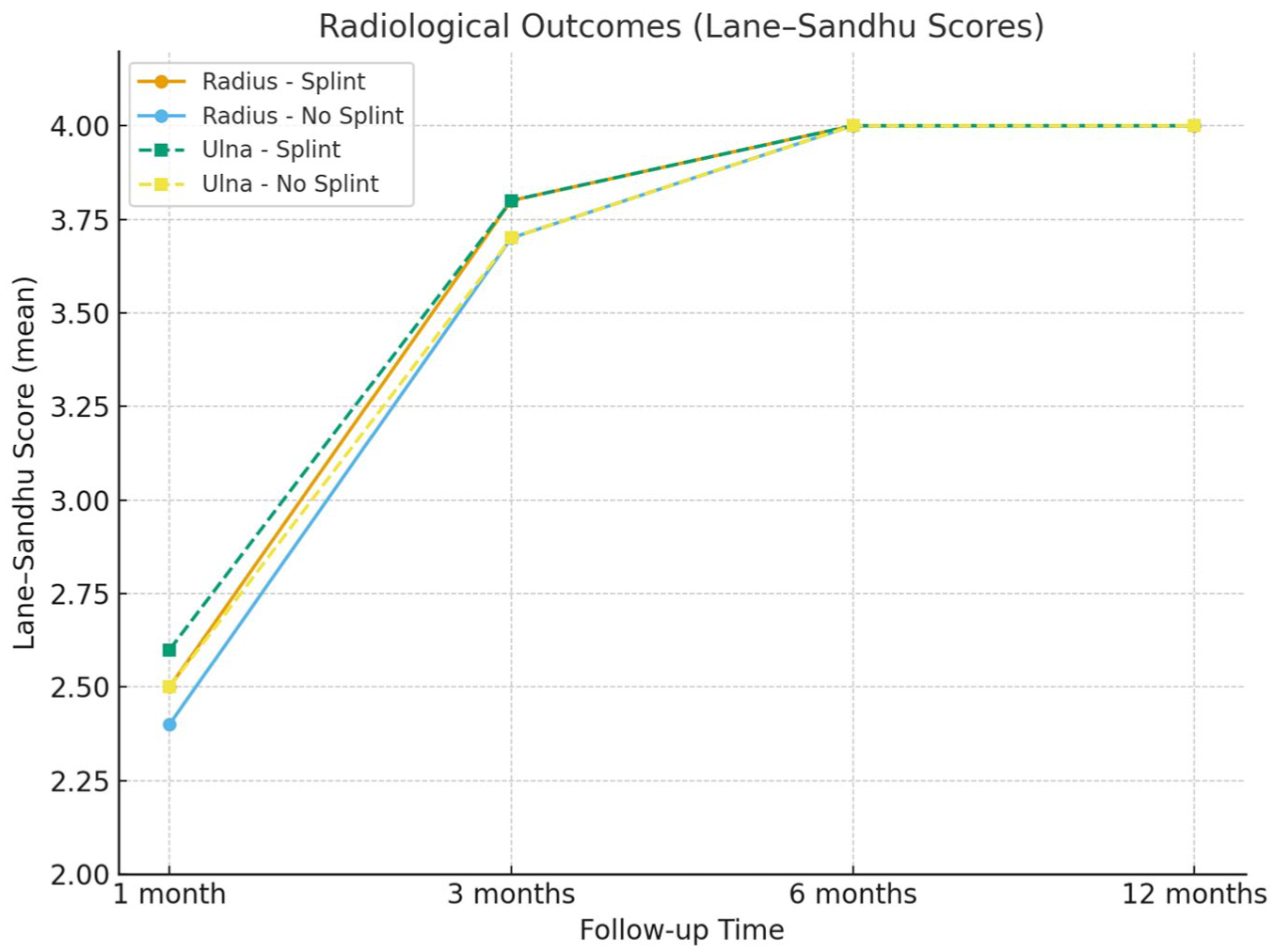
Radiological outcomes based on Lane–Sandhu scores at 1, 3, 6, and 12 months in splint and non-splint groups.
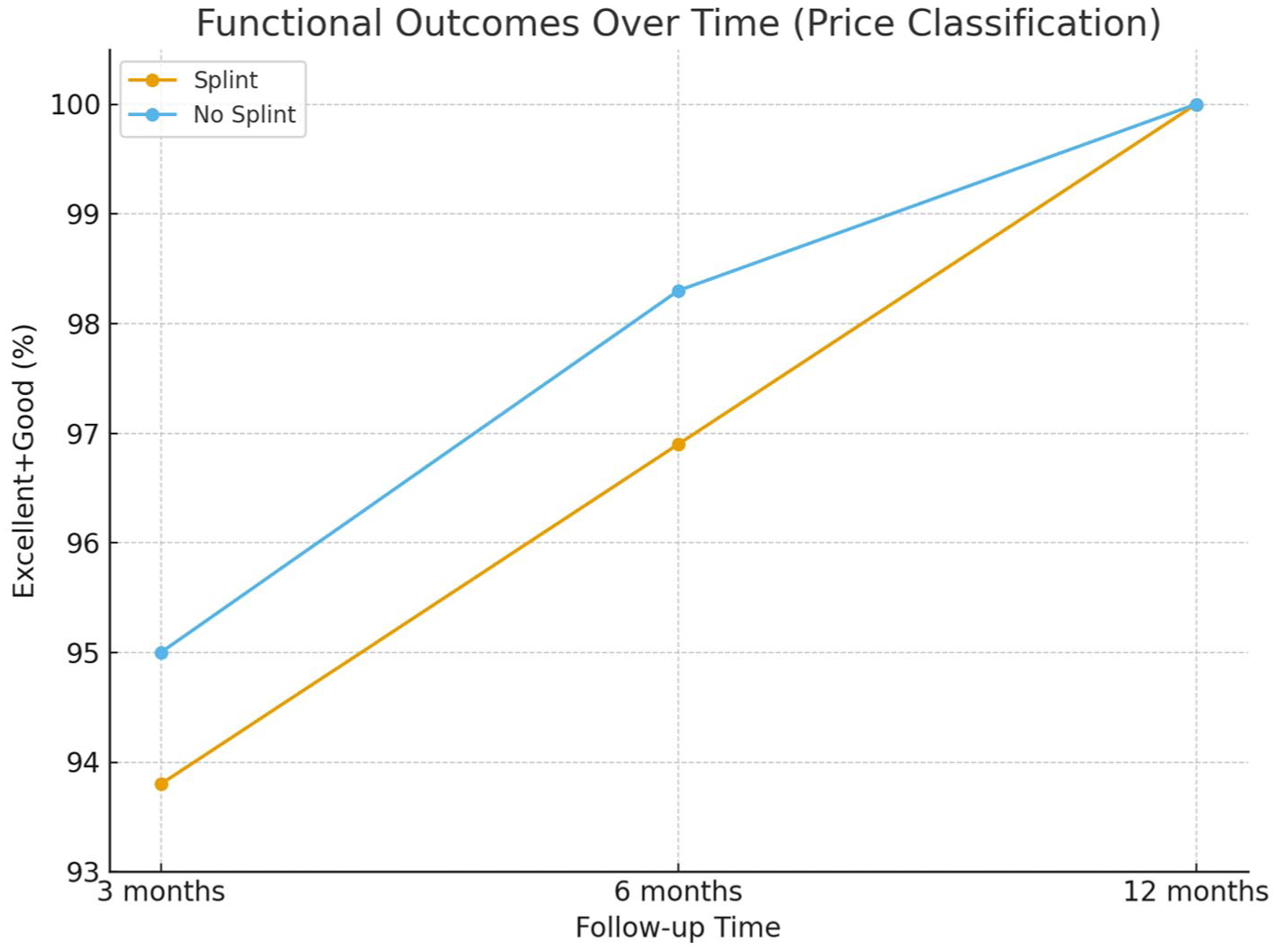
Functional outcomes based on price classification (Excellent + Good) at 3, 6, and 12 months in splint and non-splint groups.
Discussion
Although the treatment of pediatric diaphyseal both-bone forearm fractures with ESIN has become widely adopted, there is no clear consensus on the necessity or duration of postoperative immobilization with splinting. In the literature, both routine splinting and early mobilization strategies have been described; however, direct comparative studies with homogeneous cohorts remain limited. In the study by Fernandez et al., 7 factors contributing to nonunion in pediatric forearm fractures were discussed, but postoperative immobilization was not addressed. The present study specifically focused on radiological and functional outcomes in closed, mid-diaphyseal fractures treated with ESIN, aiming to compare splinting versus early mobilization within a single-center cohort.
The groups were comparable in baseline characteristics. Radiologically, Lane–Sandhu scores increased significantly from 1 to 3 months, with complete union (mean score 4.0) achieved in all patients at 6 and 12 months. At the 3rd month, the splint group showed slightly higher radiological scores (Radius p = 0.59 / Ulna p = 0.61). Functionally, based on the Price classification, the non-splint group demonstrated a slightly higher proportion of “excellent/good” outcomes at the third month (p = 0.96). At both 6 months (p = 0.97) and 12 months (p = 1), no significant differences were observed between groups in either radiological or functional outcomes. All comparisons failed to reach statistical significance (p > 0.05).
The Lane–Sandhu scoring system, which we used to assess radiological union, is a reliable and validated method for evaluating bone healing. 8 For functional evaluation, although various upper extremity scoring systems exist in the literature, we preferred the Price criteria, which are specific to pediatric forearm fractures. 9 Our findings suggest that early mobilization under the stability provided by ESIN does not delay bone healing and does not negatively affect function in the short to mid-term. The minor, opposing differences observed at 3 months (radiology favoring splinting, function favoring non-splinting) were not statistically or clinically meaningful. These findings are consistent with the notion that early motion may reduce joint stiffness without compromising union when stable fixation is achieved. In clinical practice, the selective use of splinting and encouragement of early mobilization appears rational when appropriately indicated.
Complications also warrant discussion. Potential issues such as compartment syndrome, joint stiffness, nonunion, tendon injury, osteomyelitis, and wound problems should always be considered. Interestingly, compartment syndrome has been reported more frequently in patients treated with ESIN compared to those managed conservatively with casting. 10 This unexpected finding has been primarily attributed to surgical technique rather than postoperative immobilization. In our series, two patients in the splint group developed compartment-like symptoms that required close inpatient monitoring. However, swelling resolved spontaneously without intervention, and no long-term impact on union or functional recovery was observed. No patient required reoperation.
In a recent prospective study conducted by Kłosiński et al. between 2018 and 2020, the necessity of postoperative splint immobilization in pediatric diaphyseal two-bone forearm fractures that underwent ESIN was investigated. Thirty eight patients were included in the study; a splint was applied for an average of 3.9 weeks in 14 patients, while early motion was initiated only with a triangular arm sling in 24 patients. No significant differences were found between the groups in terms of bone healing time (3.79 months vs. 3.13 months), complication rates (splint: 28.6%; without splint: 29.2%), and final functional outcomes. Although early motion regain was faster in the group without a splint, the range of motion at final follow-up was similar in both groups. However, the rate of patients without pain at the second postoperative week was found to be significantly higher in the splint group (approximately 86% vs. 50%). The authors noted that the splint only contributed to pain control in the early period; he emphasized that ESIN does not offer any additional advantage in terms of long-term function, speed of recovery, or complications, and that it is a safe and effective treatment in both approaches. 11 However, this study has several methodological limitations compared with the present investigation. First, the cohort was small and heterogeneous, including a broad age range and varying degrees of fracture instability. Radiologic healing was not assessed with validated scoring systems, and functional evaluation relied solely on the general upper-extremity range of motion degree rather than pediatric forearm-specific metrics. By contrast, our study evaluated a substantially larger and strictly homogeneous population of closed mid-diaphyseal fractures treated with standardized ESIN principles, incorporated validated radiologic (Lane–Sandhu) and functional (Price) scoring systems, and included long-term follow-up at 1 year. This methodological rigor allows our findings to provide more precise and clinically meaningful evidence regarding the true impact of postoperative splinting after pediatric forearm ESIN.
In a retrospective comparative study of 137 pediatric diaphyseal forearm fractures, Schwarz et al. evaluated complication rates in splinted and unsplinted patients after ESIN. Eighty-one patients were followed with splints, and 56 without splints, and the groups were similar in terms of age, gender, AO classification, and trauma energy. The results showed that there was no difference between the groups in terms of bone union time, but complications were significantly higher in the splinted group (16% with splints and 5.4% without splints). Observed complications included delayed union, superficial infection, refracture, and pin migration; complication rates were reported to peak in patients splinted for 3–4 weeks. It was emphasized that open fractures and the need for open reduction increase the risk of complications. Long-term functional outcomes were assessed with QuickDASH, with near-perfect results (mean score of ~0.4 points) in both groups, and splinting was not associated with functional recovery. The authors state that the stability provided by ESIN makes additional splint immobilization unnecessary and that splint use may increase the complication rate. 12 However, several key differences distinguish the present study from the work of Schwarz et al. Although their cohort was larger, it was markedly heterogeneous, including a wide age spectrum (4.9–17.6 years), mixed AO fracture types, both closed and open fractures, and cases requiring open reduction—factors known to directly influence complication rates. Postoperative management was also highly variable, with splinting duration ranging from 2 to 6 weeks according to surgeon preference, which may explain the complication peak observed in the 3–4 week subgroup. Moreover, their functional evaluation relied solely on the QuickDASH questionnaire, a generic upper-extremity instrument that is not specific to pediatric forearm injuries and may fail to detect subtle functional deficits related to pronation–supination. By contrast, our study eliminated these confounders by selecting a strictly homogeneous patient population of closed, mid-diaphyseal fractures treated exclusively with standardized ESIN principles, without open reductions, and by employing validated pediatric fracture-specific assessment tools (Lane–Sandhu for radiologic union and Price criteria for function). This methodological precision allows our findings to more accurately isolate the true effect of splint versus non-splint postoperative protocols, demonstrating that when ESIN principles are fully respected, radiologic and functional outcomes remain uniformly excellent regardless of splinting.
A recent prospective study by Herdea et al. evaluated pediatric both-bone forearm fractures treated with ESIN and compared outcomes between cast immobilization and no casting. Children aged 5–14 were randomized, and one group was followed postoperatively in a 3-week upper arm cast, while the other group was allowed active motion from the first day. The REBORNE callus score was used for radiological assessment, and the PedsQL quality of life scale was used for functional assessment. Findings showed that the cast-free group exhibited significantly faster callus formation at 3 and 6 weeks, and PedsQL scores were significantly better at 6 weeks. No major complications, such as delayed union, nonunion, or dislocation, were reported in either group. The authors emphasized that the stability provided by ESIN precludes additional cast immobilization, while early mobilization accelerates healing and improves quality of life. However, the follow-up period was limited to only 6 weeks, and long-term functional and radiological outcomes were not evaluated. 13 Although the study by Herdea et al. provides valuable early-phase data favoring cast-free management, its methodology differs substantially from the present investigation. First, the comparison was made between cast immobilization and no cast, whereas our cohort included only splint versus no-splint protocols, as plaster casting is not routinely used in our postoperative practice. Furthermore, their follow-up was limited to the first 6 weeks and relied on early callus formation assessed with the REBORNE score and on general quality-of-life evaluation using the PedsQL scale, without incorporating pediatric forearm-specific radiologic or functional scoring systems or long-term follow-up.
This study has limitations. Its retrospective, non-randomized design introduces potential selection and confounding bias, as treatment allocation was based on surgeon preference. Ceiling effects—universal union and excellent functional recovery by 6 and 12 months—may have limited the detection of subtle differences, increasing the risk of type II error. Furthermore, the single-center design and restriction to closed, mid-diaphyseal fractures reduce external generalizability. Future studies should be multicenter, prospective, and ideally randomized. Standardized immobilization protocols, incorporation of patient-reported outcomes (e.g. pain, quality of life), assessment of return-to-school and return-to-sport timelines, cost-effectiveness analyses, and systematic reporting of effect sizes and confidence intervals for time-to-union outcomes are recommended.
Similar observations have been consistently reported across major pediatric long bone shaft fractures treated with ESIN. In general, ESIN offers clear early advantages such as faster mobilization, earlier weight-bearing, and quicker pain relief; however, these short-term benefits tend to diminish over time, with 1-year functional and radiological outcomes ultimately comparable to those of conservative management. For femoral shaft fractures, the landmark multicenter study by Flynn et al. 14 demonstrated that despite earlier mobilization and shorter hospital stay with ESIN, long-term outcomes at 1 year were not significantly different from traction or spica casting. For tibial shaft fractures, Rivera et al. 15 demonstrated that although ESIN allows earlier mobilization and weight-bearing, functional and radiological outcomes at 1 year were comparable to closed reduction and casting. Consistent with these findings, our results show that although early mobilization after forearm ESIN may offer slight short-term functional advantages, both splint and non-splint groups achieved identical union and functional recovery at 1 year. Importantly, while early-versus-delayed benefits of different fixation techniques have been extensively studied in other pediatric long bones, no published study to date has reported long-term radiological and functional outcomes specifically comparing postoperative splinting versus no splinting following ESIN in pediatric diaphyseal forearm fractures. Our study, therefore, provides a novel and clinically meaningful contribution by evaluating both early and long-term results within a strictly homogeneous cohort. Moreover, in patients fulfilling intraoperative ESIN criteria—namely, successful closed reduction, appropriate nail sizing, proper three-point fixation, and atraumatic technique—our findings demonstrated a 100% rate of radiological union and complete functional recovery at long-term follow-up, regardless of postoperative splinting. These results further reinforce ESIN as the gold-standard treatment for pediatric diaphyseal forearm fractures and validate the accuracy and reliability of ESIN principles for achieving excellent long-term outcomes.
In pediatric patients with closed, mid-diaphyseal both-bone forearm fractures treated with ESIN, splint, and non-splint approaches yield equivalent long-term radiological and functional outcomes. At 3 months, radiological outcomes slightly favored the splint group, while functional outcomes slightly favored the non-splint group; however, these differences were neither statistically nor clinically significant. No differences were observed at 6 and 12 months. Postoperative follow-up protocols may therefore be tailored by the surgeon according to patient compliance and fracture morphology.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521261419324 – Supplemental material for Postoperative immobilization versus early mobilization following titanium elastic nailing in pediatric diaphyseal both-bone forearm fractures: A retrospective comparative study
Supplemental material, sj-pdf-1-cho-10.1177_18632521261419324 for Postoperative immobilization versus early mobilization following titanium elastic nailing in pediatric diaphyseal both-bone forearm fractures: A retrospective comparative study by Süleyman Kozlu, Bilgehan Ocak, Barış Görgün, Süleyman Kaan Öner and Sabit Numan Kuyubaşı in Journal of Children's Orthopaedics
Footnotes
Author contributions
The following statements should be used “Conceptualization, SK and BO; Methodology, SK; Software, BO; Validation, SKÖ, BG and SNK; Formal analysis, BO; Investigation, SK; Resources, SK; Data curation, SK; Writing—original draft preparation, SK; Writing—review and editing, SKÖ; Visualization, SK; Supervision, SNK and BG; Project administration, SK; Funding acquisition, SK. All authors have read and agreed to the published version of the manuscript.”
Data availability statement
All data generated or analyzed during this study are included in this published article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
All procedures were performed in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments. and approved by the Non-Interventional Clinical Research Ethics Committee of Kutahya Health Sciences University (Approval No: 2025/08-31 / Date: 19/06/2025). Written informed consent was obtained from all participants and/or their legal guardians prior to inclusion in the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.