
Abstract
Abstract
Purpose
We encountered problems with the Curtis and Fisher technique of quadricepsplasty for congenital quadriceps contracture, including wound dehiscence, insufficient lengthening of the quadriceps and instability of the knee. We modified the operative technique to address these three problems. We undertook this study to evaluate the results of the modified technique of quadricepsplasty to determine if we succeeded in overcoming these limitations of the original technique.
Methods
Twenty children (33 knees) underwent the modified Curtis and Fisher quadricepsplasty through a lateral incision; a long tongue of the rectus femoris was raised and the vasti mobilised without dividing the lateral retinaculae till the collateral ligaments. The children were followed up for a mean period of 63 months and evaluated. The healing of the wound, active and passive range of motion (ROM) of the knee, the stability of the knee, quadriceps power and knee function were assessed.
Results
Primary wound healing occurred in 32 of 33 knees. Adequate lengthening of the quadriceps sufficient to facilitate knee flexion to 90° was possible. Considerable improvement in the ROM was noted. In non-syndromic congenital dislocation of the knee (CDK), the quadriceps power was Grade 5, but minor degrees of extensor lag was noted. In a proportion of patients, minor degrees of joint instability was present. The majority of children were community walkers. The overall results were better in non-syndromic CDK than in children with arthrogryposis, but differences of some variables were not significant.
Conclusion
The modifications to the original Curtis and Fisher technique overcame the specific problems they were expected to avoid.
Keywords
Introduction
As with other congenital anomalies of the extremities, it is desirable that a concerted effort is made to treat congenital quadriceps contracture (CQC) and congenital dislocation of the knee (CDK) by non-operative means, since gratifying results can be achieved by serial casting and splinting in a proportion of children with these anomalies, provided the treatment is instituted in the neonatal period [1–4]. However, the more recalcitrant deformities that do not yield to these non-invasive measures and children who present late will require surgery involving quadricepsplasty or lengthening of the contracted quadriceps muscle. Several techniques of quadricepsplasty for CDK have been reported in the literature, ranging from percutaneous recession [5] and mini-open quadriceps tenotomy [6] to methods of formal open lengthening [7–9]. Among these methods, the technique described by Curtis and Fisher [7] was the most widely followed, and it was the procedure which we adopted for several years. We encountered three specific problems with the technique of Curtis and Fisher, which prompted us to modify the technique. The problems included wound dehiscence of an anteriorly placed incision, insufficient lengthening of the quadriceps to permit post-operative immobilisation of the knee in 90° of flexion and medio-lateral instability of the knee following release of the retinaculae up to the collateral ligaments. The modifications we made were aimed to address these three problems. We now report the results of surgery in a consecutive series of children who underwent the modified Curtis and Fisher quadricepsplasty.
The study was conducted in order to evaluate the results of this surgical approach in children with CQC and CDK and to determine if the limitations of the original Curtis and Fisher technique could be overcome by the modifications we made.
Materials and methods
The research protocol was reviewed and approved by the Institutional Ethics Committee.
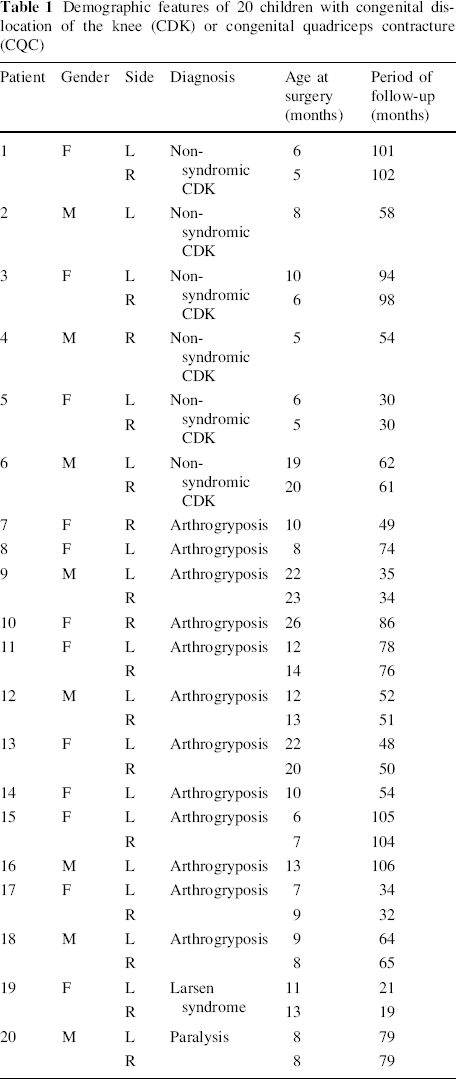
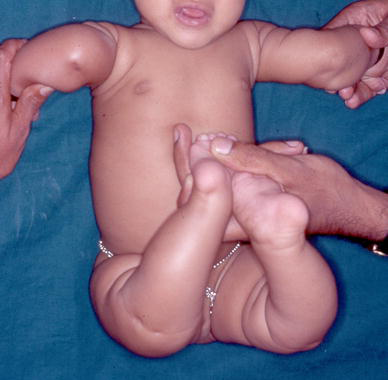
The modified Curtis and Fisher quadricepsplasty was performed on 37 knees in 23 children with CDK or CQC that were not amenable to non-operative treatment between 2003 and 2010. Twenty children (33 knees) had a minimum follow-up of 18 months and they were included in the study. Four patterns of knee anomalies were noted in these patients (Table 1). In 10 knees of 6 children, CDK was either an isolated anomaly or was associated with clubfeet or developmental dysplasia of the hip (DDH), but there were no features of classical arthrogryposis, hypermobile joint syndrome or paralysis (non-syndromic CDK; Fig. 1). In 19 knees in 12 children, CDK or CQC was associated with amyoplasia congenita (AMC or classical arthrogryposis; Fig. 2). In one child, CDK of both knees was part of hypermobile joints of Larsen syndrome (Fig. 3). One child had lower motor neuron paralysis of obscure aetiology and bilateral CDK. Associated DDH of one or both hips were present in 17 of 20 children, while foot malformations were present in 13 children.
Demographic features of 20 children with congenital dislocation of the knee (CDK) or congenital quadriceps contracture (CQC)

Non-syndromic congenital dislocation of the knees

Congenital quadriceps contracture in a child with arthrogryposis
Congenital dislocation of both knees in a child with Larsen syndrome. Note the extreme hypermobility of the shoulders
Since 18 of the children were referred from other centres, exact details of initial treatment were not available. Our indications for surgery were failure of non-operative treatment in infants below 6 months of age (n = 3) or inability to passively flex the knee beyond 45° in children who were 6 months of age or older.
The mean age at surgery was 11.8 months (range: 5–26 months). The mean period of follow-up was 63 months (range: 19–105 months). All the children underwent the same operative procedure outlined below.
The operation
The operation is performed without a tourniquet with the child in the supine position. An incision is marked on the lateral aspect of the thigh extending from the mid-thigh to the knee. In many instances, it may be difficult to obtain an orientation of the limb to clearly identify the lateral aspect of the thigh. We have found it helpful to perform the following manoeuvre to achieve a proper orientation of the limb. The knee is hyperextended passively; the posterior aspects of both the condyles of the femur are now clearly palpable (Fig. 4). By placing two fingers on the condyles, the popliteal fossa and the posterior aspect of the thigh are defined and, with this as the reference, the incision is made on the lateral aspect of the thigh (Fig. 5). The most distal part of the incision is curved gently towards the patellar tendon. The incision is deepened down to the deep facia and dissection in this plane is continued medially till the quadriceps tendon is identified. The rectus femoris tendon is separated from the vastus medialis and lateralis by sharp dissection (Fig. 6a) and a long tongue of tendon is fashioned and divided transversely at the musculo-tendinous junction of the rectus femoris (Fig. 6b). The rectus femoris tendon, along with the patella, is reflected distally to expose the knee joint and the knee is flexed to 90° (Fig. 6c). The suprapatellar pouch may often be poorly formed, but once the patella with the tongue of the rectus femoris is reflected distally, the knee can be flexed. The iliotibial band and hamstrings move posteriorly as the knee is flexed, along with the vastus medialis and lateralis, which get pulled away widely from the midline (Fig. 6c; double arrows). These structures do not need to be divided in order to obtain knee flexion. Pristine articular cartilage of the knee is clearly visualised at this stage, irrespective of the severity of the contracture of the quadriceps. The vastus medialis and lateralis are then detached from the margins of the patella and the distal fibres are detached from their origins from the respective supracondylar ridges (Fig. 6c; dotted line) so as to enable the ends of the vasti to be brought together in the midline. The knee is extended and the distal ends of the vasti (Fig. 6d; VM and VL) are anchored to the proximal end of the tongue of the rectus tendon (Fig. 6d; RFT). The medial and lateral retinaculae are not divided transversely and the collateral ligaments are also not touched. Adequate lengthening of the quadriceps mechanism is obtained to facilitate knee flexion to 90°, without any tension on the sutured ends of the vasti and the rectus tendon (Fig. 6e). The wound is closed in layers over a suction drain after meticulous haemostasis is obtained. Care is taken to see if there is any blanching of the skin over the front of the knee when the knee is flexed to 90° after wound closure (Fig. 6f). If no blanching is noted, the knee is held in 90° of flexion and an anterior above-knee plaster of Paris slab is applied. If any blanching is noted, the degree of flexion is reduced till the circulation improves and the knee is immobilised in this position. The slab is retained for 4 weeks and knee mobilisation exercises are begun thereafter. Supervised physiotherapy is given for a week and, thereafter, the parents are encouraged to continue active and passive exercises at home for 6 weeks.

The knee is hyperextended and two fingers are placed over the posterior aspects of the femoral condyles to help in obtaining an orientation of the lateral surface of the thigh before making the incision

The incision is made on the lateral aspect of the thigh and the distal part of the incision is curved towards the patella
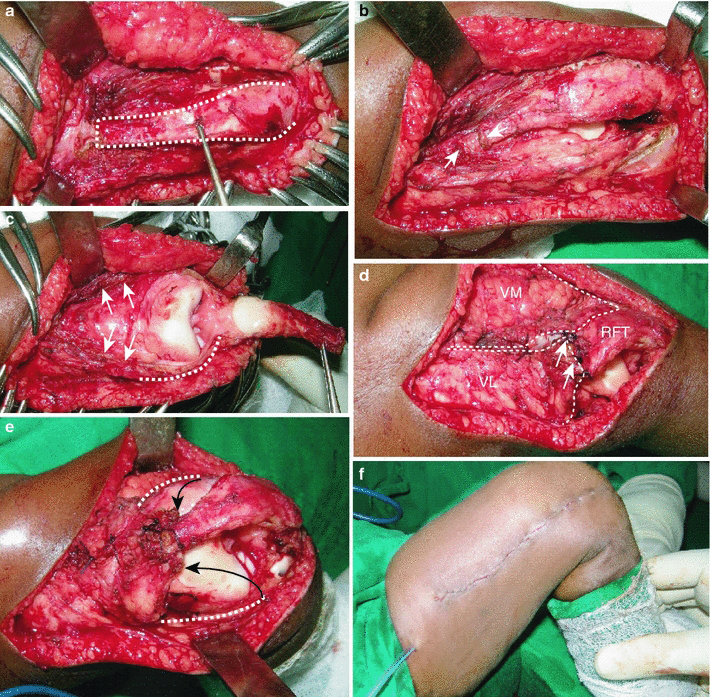
A long tongue of the rectus femoris tendon is fashioned (
Follow-up evaluation
On the last follow-up, the following variables were recorded. The width of the scar, the presence of scar hypertrophy and adherence of the scar to the deeper tissues was noted. The active and passive ranges of motion (ROM) of the knee, and the degree of hyperextension or flexion deformity, when present, were measured with the help of a goniometer. The quadriceps power was tested by manual muscle testing and graded on the Medical Research Council (MRC) scale. The stability of the knee in both the antero-posterior (sagittal) and medio-lateral (coronal) planes was checked and quantified according to the grading of Hughston et al. [10]. The children were questioned to ascertain if they had pain on movement of the knee or during physical activity. The ambulatory status of the child at follow-up was classified as community walker, household walker or non-walker. In 13 of the 20 patients, the Lysholm knee questionnaire [11, 12] was administered in order to assess the function of the knee.
Statistical analysis
The statistical analysis was performed with the Statistical Package for the Social Sciences (SPSS version 16). Differences of continuous variables between non-syndromic CDK and CDK and CQC associated with AMC were compared by the independent t-test. Differences of non-parametric variables between these two groups were compared by the Mann–Whitney test. A p-value less than 0.05 was considered as being significant.
Results
Wound closure and wound healing
In all 33 knees, it was possible to suture the quadriceps with the knee in 90° of flexion. However, the position of post-operative immobilisation was dictated by the presence of blanching of the skin on flexing the knee. In 29 knees, it was possible to immobilise the knee in 90° of flexion following the surgery; the position of immobilisation was restricted to 80° in one knee, 70° in two knees and 60° in one instance. There were no intra-operative complications. Primary wound healing was observed in 32 knees; wound dehiscence without any evidence of infection occurred in one knee (case 1, right knee; Table 2). At final follow-up, the mean scar width measured at its widest point was 9 mm (range 3–20 mm); the widest scar was noted in the knee that had wound dehiscence. Scar hypertrophy was noted in five knees and the scar was adherent to deeper tissues in one instance.
Outcome of modified Curtis and Fisher quadricepsplasty in 33 knees in 20 children
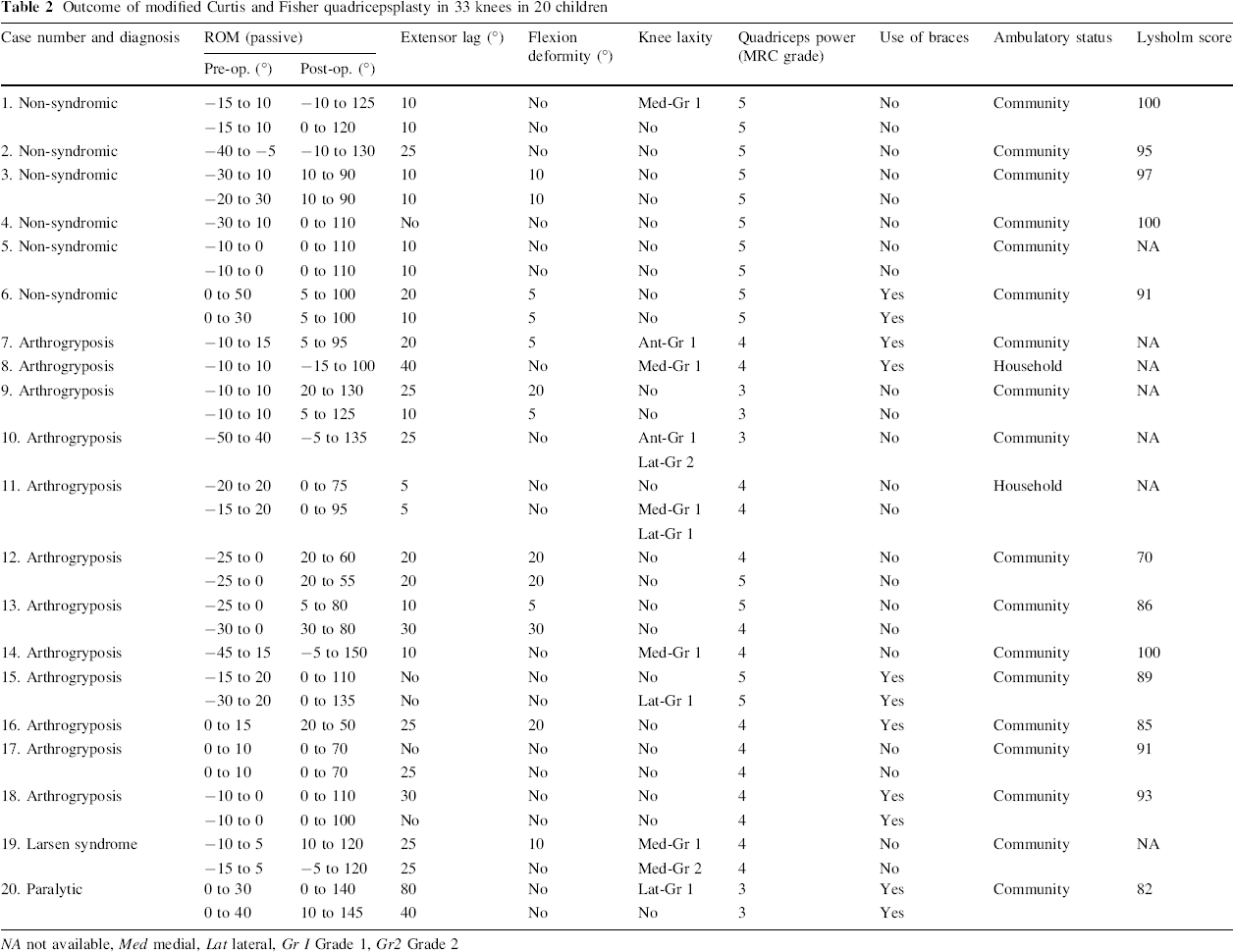
NA not available, Med medial, Lat lateral, Gr I Grade 1, Gr2 Grade 2
Quadriceps power
The median power of the quadriceps was Grade 5 in non-syndromic CDK, while it was Grade 4 in CDK associated with arthrogryposis (p < 0.01; Tables 2 and 3). The power of the quadriceps muscles of the child with paralysis was Grade 3. Some degree of extensor lag was noted in several children, even though they had what appeared to be Grade 5 power of the quadriceps on manual muscle testing (Table 2).
Comparison of outcome variables in non-syndromic CDK and CDK or CQC associated with arthrogryposis
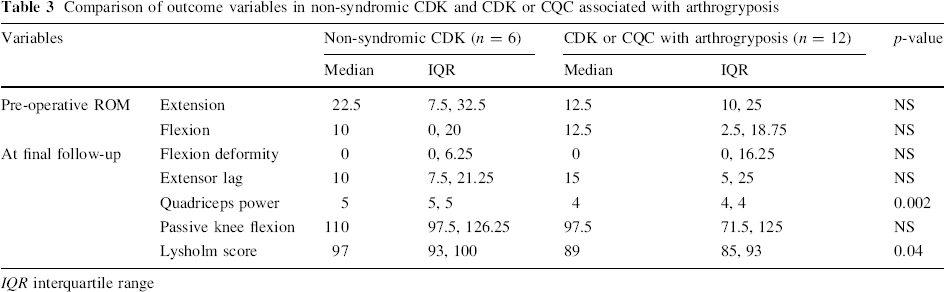
IQR interquartile range
ROM and stability of the knee
The mean post-operative passive arc of ROM of the affected knees was 99.9° (range: 30–155°), which represented a mean improvement of 68.9° from the mean pre-operative arc of ROM of 30.5° (range: 10–90°). The increase in the ROM achieved in non-syndromic CDK was comparable to that achieved in children with AMC (Table 2). Minor degrees of flexion deformity at the knee were encountered frequently (mean 5.6°). The severity of flexion deformity appeared to be greater in children with arthrogryposis than in non-syndromic CDK, but this difference was not statistically significant. Ligament laxity with demonstrable instability was noted in ten knees in either the coronal or sagittal planes; in most instances, the instability was of a minor grade (Table 2).
Functional evaluation
All the children with non-syndromic CDK were community walkers and five of them walked without any form of bracing. Among the 14 remaining children, 12 were community walkers and two were household walkers. Seven patients (35 %) used braces for walking; in six instances, the brace was not intended to support the knee but was primarily needed to stabilise the ankle and foot. The child with paralysis (Case 20) required a knee–ankle–foot orthosis in view of the quadriceps weakness.
The mean Lysholm score was excellent in children with non-syndromic CDK and was higher than in children with arthrogryposis (p < 0.05; Table 3).
Discussion
Our indications for operating on children with CDK and CQC were identical to those advocated by Johnson et al. [13] and our aim was to attempt to obtain 90° of knee flexion without weakening the quadriceps excessively.
The results of this study demonstrate that it is possible to obtain adequate lengthening of the quadriceps to facilitate tension-free approximation of the ends of the lengthened quadriceps with the knee held in 90° of flexion. This was feasible in every single instance without having to use a tendon or fascial graft and without having to shorten the femur; we attribute this to the method we adopted of fashioning a long tongue of the rectus femoris tendon. We were unaware of previous reports of this modification when we began using this technique; however, an identical method of lengthening of the quadriceps mechanism has been mentioned in the literature [7]. Curtis and Fisher attribute this modification to Calandra and furnish an illustration of the technique in their report. We believe that this modification is desirable, as it is important to obtain 90° of flexion of the knee at the outset in order to achieve satisfactory knee flexion in the long term.
Our impression that an anteriorly placed incision is fraught with risks of wound breakdown has been substantiated in the literature [13, 14], where instances of severe wound-related complications have been recorded. We encountered wound dehiscence of the lateral incision on only one occasion and subsequent healing occurred without compromising the final outcome in any way. The lateral incision gave adequate exposure of all the structures to be released, including the medial fibres of the vastus medialis muscle. In 88 % of instances, the knee could be flexed to 90° following wound closure without any compromise of cutaneous circulation. The quality of initial wound healing was satisfactory (Fig. 7), though some broadening of the scar was noted in some knees at the final follow-up. We were unable to compare the quality of wound healing in our study with other reports, as this issue has not been addressed in the literature. In the light of the results of this study, we would recommend the routine use of a lateral incision in preference to an anterior incision while performing a quadricepsplasty for CDK or CQC.

Healing of the scar of quadricepsplasty has occurred by primary intention
Several authors have reported knee instability following surgery for CDK with frequencies as high as 78 % [7, 12, 13, 15]. It is uncertain if the technique of surgery contributed to the high frequency of instability in some of these reports. We scrupulously avoided disturbing the attachments of the collateral ligaments during surgery. Among children with non-syndromic CDK, only one instance of mild medial ligament laxity was noted, though the frequency of ligament laxity was higher among children with arthrogryposis. There were no instances of severe instability, even among the children with arthrogryposis and Larsen syndrome necessitating bracing of the knee. Though we cannot state with any degree of certainty that the frequency or severity of instability was minimised by our surgical approach, we have demonstrated that release of the collateral or cruciate ligaments is not necessary for obtaining adequate knee flexion while operating on CDK and CQC, and we would recommend not interfering with these important structures.
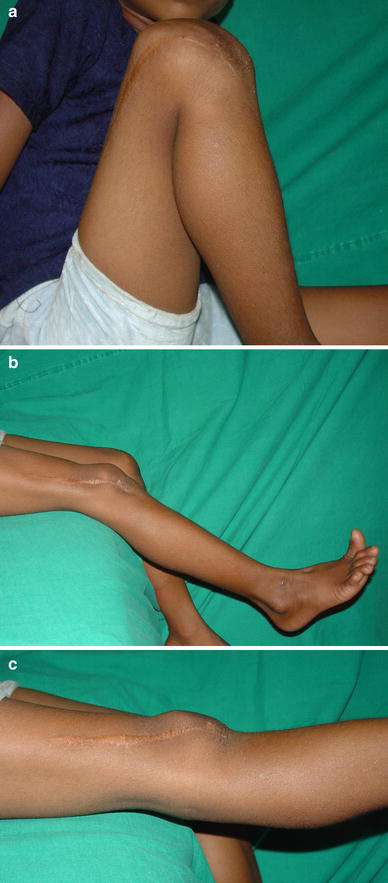
The primary aim of the study was to assess whether the modifications in the surgical technique of quadricepsplasty could avoid the complications we had encountered in the past while using the technique of Curtis and Fisher. Our results suggest that the modifications we made (Fig. 8) do help avoid these complications. However, it is also important to evaluate if the overall outcome of our surgical intervention is satisfactory. The ideal outcome of performing a quadricepsplasty for CDK and CQC would be a knee that flexes fully, with no flexion deformity or residual hyperextension, and without any quadriceps weakness or knee instability. We can achieve results close to this ideal situation in children with non-syndromic CDK, as a very minor degree of deformity or weakness (Figs. 9a–c and 10a, b) that does not compromise function may be considered an acceptable outcome in non-syndromic CDK. However, this degree of success is often not possible in children with arthrogryposis. Comparison of our results with other published series is difficult because of very disparate ages of patients, operative techniques and outcome measures. Despite these limitations, we have made an attempt to compare our results with other published series (Table 4) and our results compare well with these reports. What is particularly encouraging is that the results in children with arthrogryposis were not uniformly poor; our findings contradict the view of authors who imply that the results of treatment of CDK arthrogryposis are definitely associated with a poor outcome (Fig. 11a–c) [14]. However, these children do need to be followed up till skeletal maturity to ensure that the results are maintained, as it is possible that the ROM may deteriorate with time in arthrogryposis.
Diagrammatic representation of different techniques of quadricepsplasty. The upper row shows the structures divided and the skin incisions used. The lower row shows how lengthening of the quadriceps mechanism is achieved A good outcome of quadricepsplasty for non-syndromic isolated congenital dislocation of the knee. More than 120° of flexion of the knee is possible ( Lateral view of a child with non-syndromic congenital dislocation of the knee (CDK) prior to surgery (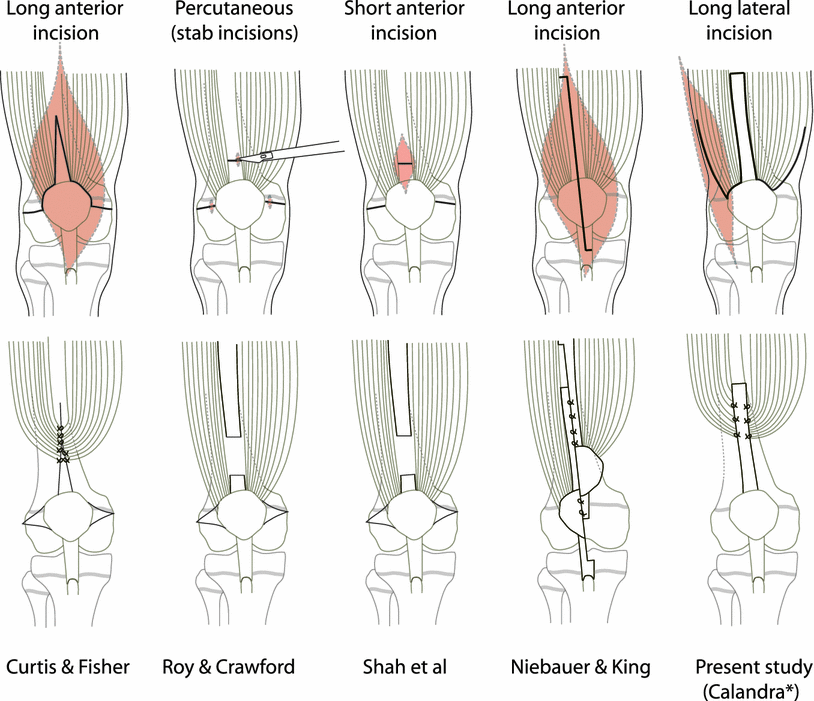

Comparison of reported outcomes in different series of cases of CDK treated by surgery
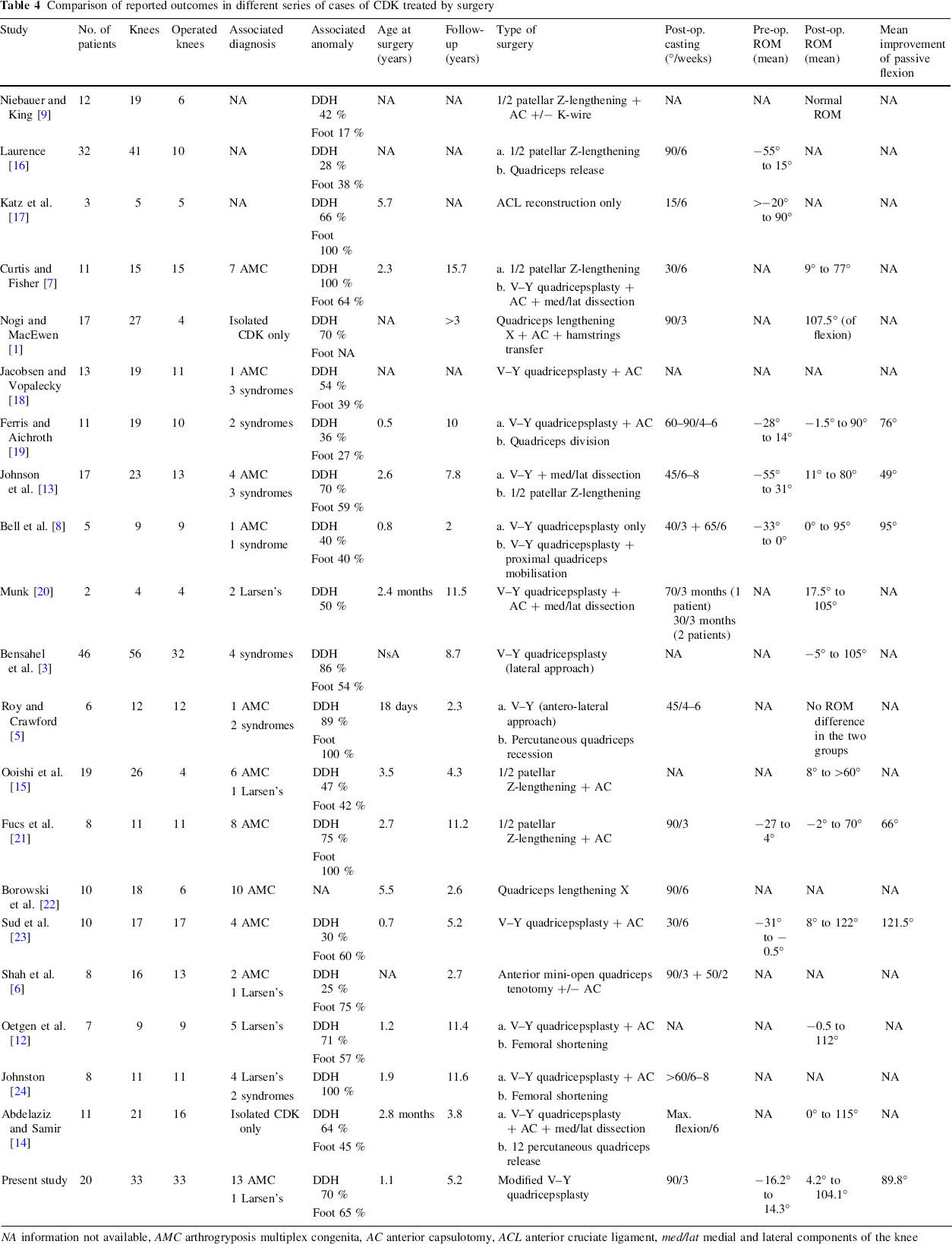
NA information not available, AMC arthrogryposis multiplex congenita, AC anterior capsulotomy, ACL anterior cruciate ligament, med/lat medial and lateral components of the knee

Lateral radiograph of the left knee (
Recently, there has been a trend to include functional outcome measures while evaluating the results of the treatment of several orthopaedic disorders in children, and this has been advocated for CDK also [12]. We administered the Lysholm questionnaire to a subset of children included in the study. However, since functional activities could be limited on account of associated problems of the hips, ankles and feet of children with arthrogryposis, it was not possible to discern if any reported limitation was on account of the knee per se. Similarly, in children with bilateral CDK, it was not possible to define which knee was responsible for functional limitations the child may have had. It, thus, became clear to us that, while the Lysholm questionnaire may be useful in evaluating the outcome of unilateral isolated CDK, it is of limited use in bilateral CDK and CDK associated with foot or hip anomalies. Hence, the observation that the Lysholm score was lower in children with arthrogryposis (Table 3) should be interpreted caution; the difference may be on account of associated problems of the hips and feet rather than a poorer result of quadricepsplasty. For this reason, we did not attempt to administer this questionnaire for all the children included in the study.
The role of quadriceps weakness and extensor lag following the treatment of CDK has been recently addressed [23]. While more severe degrees of quadriceps weakness and severe extensor lag undoubtedly compromises function (as seen in Case 20), mild extensor lag noted in several of the children did not appear to compromise function in any way.
A closer analysis of our treatment method shows that there are distinct benefits of this approach, despite the seemingly aggressive surgery through a large incision. Other authors reporting alternative techniques involving smaller incisions and limited releases have, in some instances, required a fascia lata graft to restore continuity of the quadriceps mechanism [21], encountered plastic deformation of the proximal tibia [6] and have needed more elaborate surgery subsequently for inadequate correction [6, 14]. We have not encountered tibial fractures, we have never had to resort to tendon grafting and in no instance did we have to re-operate a child. Restoration of knee motion entailed a very short period of supervised physiotherapy in this series, without having to resort to repeated manipulations under general anaesthesia every 3–4 days, as recommended by Fucs [21]. The overriding advantage of a single-event surgery over repeated general anaesthetics in an infant cannot be over-emphasised.
There are a few limitations of this study. Firstly, we did not have a control group of patients who were operated by the traditional Curtis and Fisher technique. This would have been desirable, but we were unable to locate a sufficient number of these patients to serve as historical controls. Secondly, we acknowledge that manual muscle testing of the quadriceps in young children may not be entirely reliable, but we had no better way of assessing quadriceps function.
Footnotes
Acknowledgments
The clinical fellowship of Dr. Stéphane Tercier was supported by Swiss grants (Fonds du Département médico-chirurgical de Pédiatrie et de Perfectionnement du CHUV, Fondation SICPA, Fondation de l'Hôpital Orthopédique de Lausanne et Fonds de la Société Suisse d'Orthopédie et Traumatologie).