
Abstract
Purpose
Congenital dislocation of the knee (CDK) is a relatively rare condition. It may occur as an isolated deformity, it may be associated with musculoskeletal anomalies such as developmental dysplasia of the hip and clubfoot, or it may occur as part of a syndrome such as arthrogryposis multiplex congenita or Larsen syndrome, or it may occur in paralytic conditions such as meningomyelocele. Treatment options include serial casting, percutaneous quadriceps recession (PQR) and V–Y quadricepsplasty (VYQ). The aim of this study is to evaluate the medium-term results of PQR and VYQ, and to set a protocol of management for CDK based on a modified grading system.
Methods
Eleven infants with 21 CDK were treated at our unit. Five knees were treated with serial casting, 12 knees with PQR and four knees with VYQ. Follow up averaged 41 months.
Results
Twelve knees achieved excellent results, seven knees achieved good results and two knees achieved fair results.
Conclusion
A modified grading system for CDK is introduced. Based on this, we recommend the following. Serial casting is performed in patients with GI CDK. In GII CDK in neonates (babies up to the age of 1 month) serial casting is started. A maximum of four weekly manipulations and castings are attempted. If a range of flexion >90° is achieved, serial casting is continued; if range of flexion remains <90° it is necessary to proceed to PQR. In babies older than 1 month when first seen; PQR is performed from the start. VYQ is indicated in patients with GIII CDK or in recurrent cases.
Introduction
Congenital dislocation of the knee (CDK) is a relatively rare condition, with an incidence estimated to be 1% of developmental dislocation of the hip (DDH) [1]. It may occur as an isolated deformity, it may be associated with musculoskeletal anomalies such as DDH and clubfoot [2–4], or it may occur as part of a syndrome such as arthrogryposis multiplex congenita (AMC) or Larsen syndrome or it may occur in paralytic conditions such as meningomyelocele [1, 3].
Several factors have been postulated as to the etiology of CDK. Fetal molding due to oligohydramnios or breech position was suggested by Haga et al. [5]. Abnormality of the anterior cruciate ligament was proposed by Katz et al. [6]. Quadriceps contracture was proposed by many authors to be the cause [2, 7, 8].
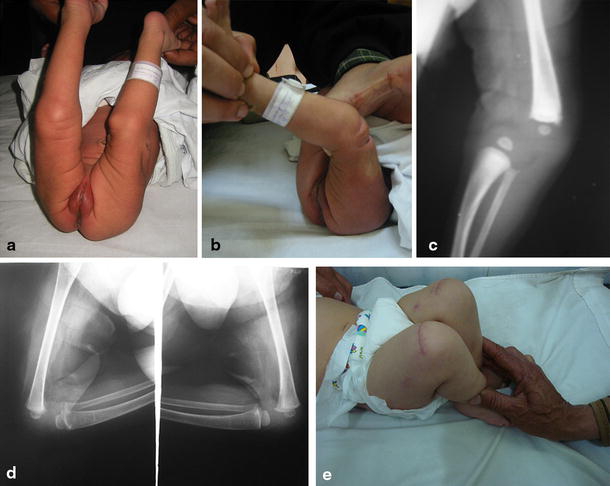
The diagnosis is established just after birth by the typical position of knee recurvatum, and is confirmed by radiography [2, 9]. Several classification systems have been described. They are all based on the radiographic findings of the femoro–tibial relationship and they classify CDK into three grades: simple recurvatum, subluxation and dislocation [1, 9–11].
Ultrasonography is useful in evaluating CDK. It provides a direct view of the pathologic lesion, is painless, and is safe. It is also useful in evaluating reduction of the joint after manipulation or surgical treatment [12].
Treatment options include serial casting, percutaneous quadriceps recession (PQR) [13] and V–Y quadricepsplasty (VYQ) [2]. Compared to PQR, VYQ is associated with increased morbidity due to a long incision with scarring, adhesions, and wound breakdown, as well as blood loss; however, it is more successful in achieving and maintaining reduction in severe and resistant cases.
The aim of this case series study is (a) to introduce a new grading system based on clinical findings (range of passive knee flexion) that correlates with the severity of the condition and allows a treatment protocol to be set, and (b) to evaluate the medium-term results of PQR and VYQ.
Materials and methods
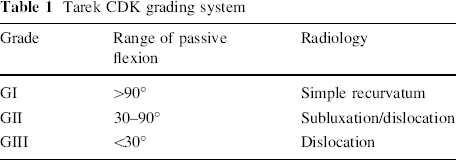
Between January 2004 and February 2008, 11 infants with 21 CDK were treated at our unit. A modification of the existing classification systems [1, 9–11] was introduced (Tarek CDK grading system); see Table 1. This was based on our observation that the range of passive knee flexion (compared to the degree of hyperextension and the femoro–tibial relationship on X-rays) is a better indicator of the severity of the condition, and consequently more suitable for selecting a treatment option. We therefore set the range of passive flexion as the primary criterion for our grading system; with a range of >90° as GI, 30–90° as GII and <30° as GIII. The reproducibility of the new grading system used in this study was good, with kappa values for intraobserver and interobserver repeatability of 0.71 and 0.72 respectively. The concordance for the intraobserver study was 82%; it was 78% for the interobserver study. Table 1 also illustrates how the X-ray findings varied regarding joint congruity in the different stages of our new grading system.
Tarek CDK grading system
CDK as part of a generalised musculoskeletal syndrome as AMC or Larsen's syndrome or as a result of spinal dysraphism were excluded from the study, as they are extremely rare and definitely associated with a poor outcome. According to our grading system; five knees were GI, 11 knees were GII and five knees were GIII (see Table 2). Seven infants had hip dislocation and five had foot deformities. Age at time of initial treatment ranged from 5 to 335 days, average 83 days. Follow-up ranged from 24 to 67 months, average 41 months. The initial treatment was serial casting in five knees, PQR in 12 knees and VYQ in four knees.
Patient details
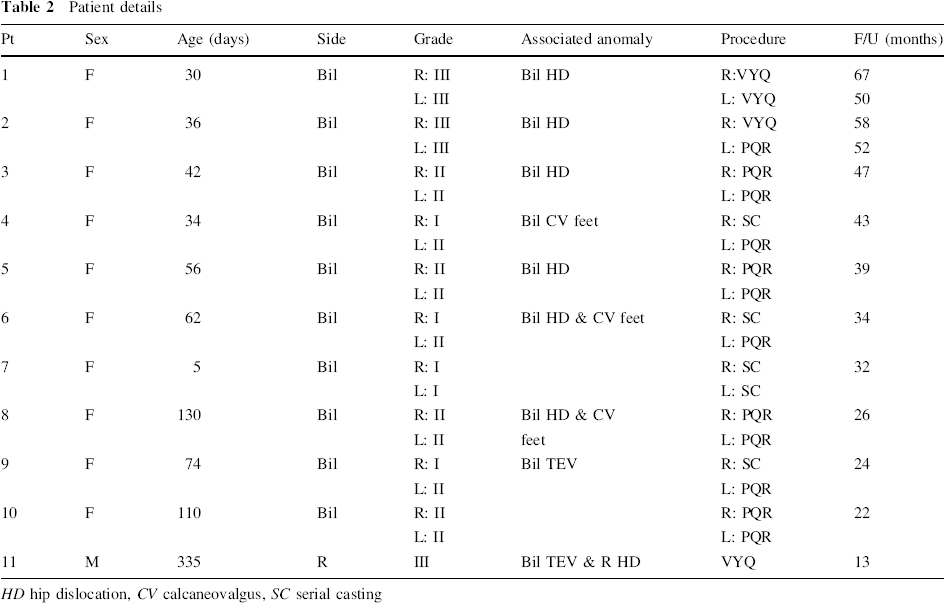
HD hip dislocation, CV calcaneovalgus, SC serial casting
At the beginning of our learning curve for management of this rare congenital anomaly we performed VYQ and PQR interchangeably, as there were no clear recommendations by the authors in their original articles as to which procedure to perform in relation to the degree and severity of the condition.
As we were disappointed initially by VYQ due to wound breakdown and infection in the first two knees and the amount of bleeding encountered in the first three knees we operated upon, we decided to perform PQR in our 4th knee although it was GIII. Unfortunately, we could not reduce the knee after the PQR, and a VYQ at a later date was mandatory.
Following this, and starting from the 3rd patient (5th knee) in the series, we developed our grading system, and the following protocol of management was set: serial casting is performed in patients with GI, PQR in patients with GII, and VYQ in patients with GIII.
PQR was performed as described by Roy and Crawford: [13]
An assistant holds the leg with the knee maintained in maximum achievable flexion.
A transverse incision is made one patella length superior to the patella in the midline.
The fascia over the rectus femoris is divided. Medial and lateral stab incisions are made at the superior border of the patella to divide the medial and lateral quadriceps and retinaculum. The knee is then forced into flexion, with the fingers applying direct forward pressure on the femoral condyles. The reduction is felt.
VYQ was performed as described by Curtis and Fischer: [2]
A long anterolateral incision is made. The central portion of the quadriceps tendon is incised in a fashion to allow V–Y advancement. The iliotibial band is released. The anterior capsule of the knee is divided transversely as far as the collateral ligaments, and the quadriceps muscle is mobilised. The knee is then reduced and flexed to 90°. The lengthened quadriceps is resutured with the knee held at 30°.
Regardless of the technique of quadricepsplasty, an above-knee cast was applied in a modified fashion. We developed this technique after having difficulty in applying the cast and maintaining knee flexion in the cast, especially in infants less than 4 months old, as the usual above-knee cast often resulted in redislocation of the knee because the volume of plaster in the popliteal fossa simply re-extended the knee. Our technique involved applying extremely good but non-bulky padding from toe to groin, and then we applied two plaster slabs; one anterior from toe to groin and the other wrapped transversely around the thigh and leg, holding the knee in maximum flexion. A crepe bandage was then wrapped around the leg. In this way, no plaster was applied in the popliteal fossa.
A PO X-ray was ordered (starting from patient # 4). The cast was removed at 6 weeks PO. No splints or physiotherapy were advised. Patients were then reviewed at 3-month intervals during the first year, then twice a year thereafter. The patients were examined to determine the range of knee movement, stability, power of extension, and functional ability. X-rays were taken at the time of cast removal, and then at every follow-up.
To evaluate our results we described a modification of the scoring system for knee function described by Ferris and Aichroth [9], as illustrated in Table 3.
Modified knee function scoring system

E Excellent, G Good, F Fair, P Poor
Mild/gross depends on whether the activities of daily living are affected or not
To qualify for a certain grade, all four criteria need to be fulfilled. If any single criterion was not fulfilled, the result was downgraded according to this criterion
Any associated hip dislocation or foot deformity was treated only after successful reduction of the dislocated knee joint.
Results
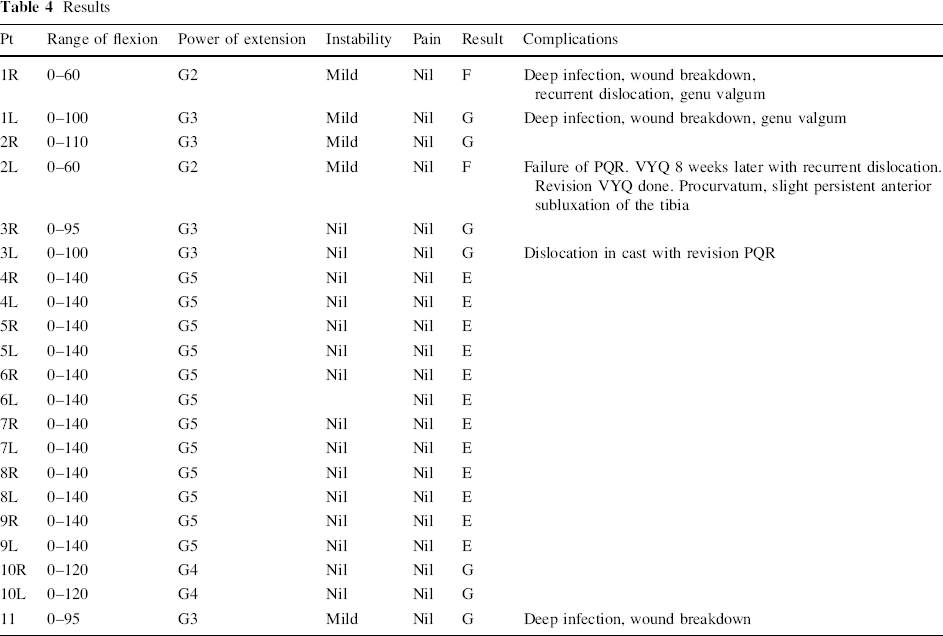
All children were able to walk independently before the age of 20 months, and all parents were satisfied with the outcome. Satisfaction was measured by asking the parent(s) to grade their child's condition at the final follow-up on a scale of zero to five; with “zero” meaning totally unsatisfied and “five” meaning extremely satisfied. Parent(s) who graded their child at “three or more” were considered satisfied. Twelve knees achieved excellent results, seven knees achieved good results and two knees achieved fair results (Table 4 and Figs. 1, 2). All knees that achieved excellent results were GI/II and had been treated by serial casting or PQR. The only knee that underwent PQR and had a fair outcome was GIII, and apparently the decision to perform the PQR was wrong.
Results
Child with an excellent result following bilateral PQR.

Child with a fair result following VYQ.
There were no skin or wound complications in children who underwent PQR.
One knee (pt # 1, R) that underwent VYQ developed wound breakdown and deep infection as well as a recurrence of the dislocation. Two debridements were needed, then a revision VYQ was performed 6 weeks later and a K wire was used to hold the reduction, as it was unstable even in 140° flexion. One knee (pt #1, L) that underwent VYQ developed wound breakdown and infection that responded to four (twice weekly) dressings and change of cast under GA.
This child developed valgus deformity of both knees that was treated by a supracondylar lateral opening wedge osteotomy. The idea of the open wedge was to achieve some lengthening that would tensionize the lax medial structures and hence stabilize the knee. The valgus was corrected. This child had a fair result in her right knee and a good result in her left knee.
One knee (pt #2, L) initially underwent PQR. Unfortunately, at surgery the knee was irreducible and a VYQ was mandatory. Because of the transverse incision, it was impossible to proceed directly to a VYQ, so the wound was closed, no cast was applied and a VYQ performed 8 weeks later. The VYQ was more difficult than in primary cases, and although at the end of the procedure the reduction was satisfactory and 140° flexion had been achieved, recurrence of the dislocation occurred again. A revision VYQ was performed 8 weeks later, and this maintained the reduction till the final follow-up. This knee developed an angulated greenstick fracture of the proximal tibia that resulted in slight procurvatum and slight persistent anterior subluxation of the tibia. This child had a good result in her right knee and a fair result in her left knee.
One knee (pt #3, L) that underwent PQR redislocated in the plaster. As routine PO X-rays were not initially ordered; the condition was only noticed at the time of POP removal. A revision of the PQR was performed, and the cast was applied using the newly described technique. Since that incident, routine PO X-rays were introduced to our protocol of management.
One knee (pt #11) that underwent VYQ developed wound breakdown and infection that responded to four (twice weekly) dressings and change of cast under GA. This child had a good result.
Because CDK is a rare condition; the number of patients included, as well as the study design, was too small to apply statistical studies. However, it can be concluded that CDK that is not part of a generalised musculoskeletal syndrome or a result of spinal dysraphism can be treated successfully. GI/II usually have excellent/good results, while GIII may have good results, although wound breakdown and deep infection are common complications.
Discussion
Patients with untreated CDK develop stiff, unstable knees. A successful surgical result is achieved with quadriceps lengthening. If the quadriceps tendon and the anterior cruciate ligament are divided, then only fair results are achieved [9].
Treatment options include serial casting, PQR [13], and VYQ [2]. Compared to PQR; VYQ is associated with increased morbidity due to a long incision with scarring, adhesions, and wound breakdown, as well as blood loss; however, it is more successful in achieving and maintaining reduction in severe and resistant cases. Laurence mentioned that the prognosis of CDK was adversely affected by delay in treatment and by the presence of other musculoskeletal deformities [7]. Most authors recommend that the knee be treated first. A good hip position cannot be maintained as long as the knee cannot be sufficiently flexed. It is also difficult to correct the equinovarus deformity of the foot caused by tension on the gastrocnemius when the knee cannot be flexed sufficiently [14]. Many modalities can be used for conservative treatment, including the use of serial casting to increase knee flexion, the Pavlik harness for posturing of the knee in further flexion, skin traction, and skeletal traction [6, 9, 15]. Haga et al. suggest that it is advisable to wait 1 month for spontaneous reduction of CDK in cases not associated with clubfoot, AMC, or Larsen's syndrome [5]. These different opinions make the treatment of CDK confusing.
Injury of the proximal tibial physis is a recorded complication of forceful manipulation in CDK. This might result in premature closure of the posterior part of the physis, with resultant tibial procurvatum [1, 5]. Genu valgum is a common complication of CDK, especially with severe grades that have been treated by VYQ. It is disabling, and is best treated by an opening wedge supracondylar osteotomy [16].
In a study by Bensahel et al. [17], 56 CDK were studied. Leveuf classification was used (GI = simple hyperextension, GII = subluxation, GIII = complete dislocation). Six knees were GI, 21 knees were GII and 29 knees were GIII. Twenty-four knees were treated conservatively (three GI, 6 GII, 15 GIII). VYQ was performed on 32 knees (three GI, 15 GII, and 14 GIII).The study concluded that there was no strict parallelism between the amount of joint displacement at onset and the operative indication. Indeed, 50% of GI knees, 71.4% of GII knees and 48.2% of GIII knees needed VYQ. In the group treated conservatively, the amount of flexion ranged from 80 to 140°; two knees were unstable and had 20° hyperextension. In the group treated surgically, the amount of flexion ranged from 80° to 160°; one knee was unstable, two knees lacked 5° extension, and two knees had 10° hyperextension.
In a study by Bell et al. [18], nine cases of CDK were included in the study. It was not possible in any case to flex the knee beyond zero degrees of extension. All knees demonstrated at least 45° hyperextension deformity. All knees had failed to respond to conservative measures (serial manipulations and plasters). All knees underwent VYQ. Excessively vigorous attempts to correct the dislocations were felt to be inadvisable because of the danger of damaging the epiphyses or the articular surfaces [1]. The patients were examined to determine the range of knee movement, stability, power of extension, and functional ability. The mean follow-up was for 24 months. All the patients were able to walk. An extensor lag of up to 30° was present in all patients except one. All the knees were stable, except one which had a positive anterior drawer sign. The quadriceps power in all cases was Grade 4 or greater. Flexion of 75° or more was achieved in eight of the nine knees.
In a study by Mehrafshan et al. [19], 45 patients with 68 CDK were treated. Conservative treatment was initially performed. If failed VYQ was undertaken. Final outcome was excellent/good in 90% and fair in 10% in group I (reducible). In group II (recalcitrant), 70% had good, 12% had fair, and 18% had poor results. In group III (resistant), 36% had fair and 64% had poor results. They concluded that the absence of anterior skin fold, knee flexion <50°, irreducible dislocation at first physical examination, and positive family history are predictive factors for poor results.
Based on the results of this study as well as the results of previous authors, particularly that of Bensahel et al. [17] on 56 CDK, it seems justified to mention that a classification based on the passive ROM is better in decision-making than the standard classification accepted worldwide. It also seems quite logical to treat GI CDK with serial casting. In GII CDK in neonates, it is worth trying serial casting. If the range of flexion exceeds 90°, serial casting is continued; if it remains <90° it is necessary to proceed to PQR. This is similar to Achilles tenotomy as an intrinsic part of Ponseti's technique in management of club feet. In GIII CDK we learnt the hard way and we had many failures of PQR, although the original authors had not restricted PQR to GII CDK. Contrary to the conclusion of Roy & Crawford [13], who advise that VYQ should be reserved for cases that fail after PQR, we recommend the following:
(1) Serial casting is performed in patients with GI CDK. (2) In GII CDK in neonates (babies up to the age of 1 month) serial casting is started. A maximum of four weekly manipulations and castings are attempted. If a range of flexion >90° is achieved, serial casting is continued; if range of flexion remains <90°, it is necessary to proceed to PQR. (3) In babies older than 1 month when first seen; PQR is performed from the start. (4) VYQ is indicated in patients with GIII CDK or in recurrent cases.
We agree with previous authors that reduction of the dislocated knee is essential prior to any attempt to treat any associated hip dislocation or foot deformity.