
Abstract
Purpose
Instability of the knee is a common finding in patients with congenital limb deficiency. The instability can be attributed to soft tissue abnormalities, frontal, sagittal or rotational deformity of the lower limb and bony dysplasia of the patella or of the femoral condyles. In most of the cases, these pathomorphologic changes stay asymptomatic in daily activity. However, instability can appear during deformity correction and bone-lengthening procedures, leading to flexion contracture or subluxation of the knee.
Methods
A review of pediatric orthopaedic literature on different factors of knee instability, state-of-the-art treatment options in congenital limb deficiency and in cases of lengthening-related knee subluxation is presented and the authors’ preferred treatment methods are described.
Results
Leg lengthening and deformity correction in patients with congenital limb deficiencies can be achieved with various techniques, such as guided growth, monolateral or circular external fixation and intramedullary lengthening nails. Radiographic assessment and clinical examination of the knee stability are obligatory to estimate the grade of instability prior to surgical procedures. Preparatory surgery, as well as preventive measures such as bracing, bridging of the knee and intensive physical therapy, can help to avoid subluxation during lengthening in unstable knees.
Conclusions
Adequate surgical techniques, preventive measures and early detection of signs of subluxation can lead to good functional results in patients with congenital limb deficiency.
Introduction
An unstable knee can be observed in various congenital deformities and appears to be one of biggest challenges in deformity correction and lengthening.
Congenital deformities which result in knee instability are longitudinal deficiencies such as congenital femoral deficiency (CFD) and fibular hemimelia (FH) or tibial hemimelia. Depending on the severity of the deficiency, the instability can be detected in early infancy or later during life, sometimes without clinical significance.
The correction of axial malalignment and leg length discrepancy is crucial in the treatment of patients with congenital longitudinal deficiencies. Severe deformities such as valgus or varus deviations, as well as rotational malalignment, can exaggerate knee instability and maltracking of the patella.
Children with severe CFD and FH may need multiple deformity correction or lengthening procedures during growth to reduce axial malalignment and leg length discrepancy. Various methods such as monolateral fixators, circular hexapod fixators and intramedullary lengthening nails have been developed. However, irrespective of the applied lengthening method, knee instability in congenital limb deficiency can unmask and can lead to knee subluxation as a severe complication.
Prevention of subluxation during lengthening in patients with congenital knee instability can be achieved with bridging of the knee with monolateral or circular fixators. Intensive physical therapy and bracing may prevent knee subluxation during lengthening using intramedullary nails.
As mild knee subluxation can easily go unrecognised on X-rays [1], clinical examination and accurate radiographic analysis during bone lengthening is necessary to detect signs of subluxation of adjacent joints as early as possible. Knee stability as well as early detection and treatment of knee subluxation has the highest priority in lengthening procedures in all patients with CFD and/or FH.
Knee pathoanatomy
Common classifications of congenital limb deficiency are the classifications according to Paley and Standard [2] and Pappas [3] for CFD and the classification of Achterman and Kalamchi [4] for FH.
In CFD and FH, specific pathomorphologic changes of the knee have been described [5]. Potential anomalies are hypoplasia or aplasia of the anterior cruciate ligament (ACL), the posterior cruciate ligament (PCL), meniscoid changes, hypoplasia of the lateral condyle and the tibial spine and patella hypoplasia. According to the main pathology, the instability can affect the sagittal, frontal or rotational plane of the knee.
Some authors estimate that 95% of FH have an absent ACL [6]. Abnormalities of the cruciate ligaments have been verified by magnetic resonance imaging (MRI) studies [7–10] and by arthroscopy [7, 11].
Manner et al. [9] developed a classification to assess the aplasia of cruciate ligaments by tunnel view knee radiographs in patients with congenital limb deficiency. They found three types of patterns of ACL/PCL involvement in MRI and radiographs analysing the lateral and medial tibial spine and the notch width and height. The ACL was affected in all (34) knees. Hypoplasia of the ACL in combination with a normal PCL occurred in 15% and aplasia of the ACL with a normal PCL in 41%. Aplasia of the ACL and hypoplasia of the PCL was seen in 21% and total absence of both cruciate ligaments was observed in 24% [9].
Other authors made similar findings regarding the ACL and PCL changes in CFD and FH [8, 10].
Besides these pathomophologic changes within the knee, the knee stability is also influenced by axial malalignment with severe valgus deformity increasing maltracking of the patella and hyperlaxity of the overused medial collateral ligaments.
Knee function
It remains unclear which patients with CFD or FH suffer from knee instability in daily activity or mild sports activity. Despite the pathoanatomy and signs of instability in physical examination, many authors conclude that there might be no or only insignificant instability in
Others state that the
There is not much data on functional outcome in daily activity or in sports participation of patients with congenital limb deficiency. Crawford et al. [6] presented the long-term results of 23 patients with fibular hemimelia and associated cruciate deficiency with a mean follow up of 18.6 years. They observed that patients with fibular hemimelia and cruciate deficiency can live active lives and many are able to participate in sports such as skiing, football or baseball similar to an age-matched control group. The authors state that, compared to outcome reports of traumatic ACL ruptures, patients with congenital ACL deficiency have less instability.
However, depending on the severity of the knee instability in congenital deformity, different problems can occur:
Instability in daily activity or sports. Knee pain, meniscal damage or degenerative changes. Complications during bone lengthening or deformity correction (flexion contracture or knee subluxation). Recurrence of axial malalignment after deformity correction [13].
Treatment of knee instability in congenital limb deficiency
Arthroscopic ACL reconstruction
Reports on arthroscopic
Gabos et al. [14] described the results of ACL reconstruction with allograft in four adolescents with congenital limb deficiency. The mean age at operation was 15.8 years. All four patients had prior limb alignment procedures and were symptomatic with instability with walking, despite of the use of an ACL brace and intensive physical therapy with muscle strengthening. The authors conclude that, with appropriate patient selection, ACL reconstruction can be an effective procedure.
Figueroa et al. [15] presented a case report of a 16-year-old patient with FH with a knee subluxation combined with a valgus and recurvatum deformity after tibial lengthening. They performed a corrective osteotomy for angular deformity correction with tibial and femoral osteotomies and simultaneous arthroscopic ACL reconstruction and observed good function at 12 months follow up.
As severe knee instability is treated with comprehensive knee reconstruction in early childhood (superknee procedure, preparatory surgery), the indication for arthroscopic ACL repair in congenital cases is rare. In the older child with symptomatic knee instability, other reasons for instability such as axial malalignment have to be corrected before considering a cruciate ligament repair.
Preparatory surgery for lengthening procedures
Knee stability can be reconstructed in early age with complex reconstruction surgery of the knee to achieve good stability for daily activity and for future lengthening procedures. This
A multitude of soft tissue procedures to reconstruct knee stability have been developed.
The most comprehensive procedure in congenital knee instability is the

This patient with congenital femoral deficiency (CFD) and fibular hemimelia (FH) with severe genu valgum and an unstable knee and hip (
External fixation
Various
Grill and Dungl [17] reported on 37 patients with congenital short femur which were treated with femoral lengthening with the Ilizarov frame (Smith and Nephew, Memphis, TN, USA) or Orthofix (Orthofix, Verona, Italy) monolateral lengthening device. Complications and knee subluxation occurred in 21%.
The safest way of lengthening is, therefore, the preventive
The long-term results of Ilizarov or TSF lengthening in children with mild to moderate fibular hemimelia showed good results and patient satisfaction at a mean follow up of 15 years. The authors extended the frame above the knee if the knee was clinically unstable [20].
Knee subluxation can occur during bone lengthening with different devices: monolateral fixator with double osteotomy and without bridging of the knee with persistent knee subluxation (treatment performed elsewhere) (
Femoral lengthening of mild and moderate CFD with clinical stable knee joints with monolateral external fixator showed good results and high function and satisfaction (PODCI score). Knee subluxation occurred in 13% and bridging of the knee and the use of an articulated external fixator was recommended [21].
Especially in the most severe knee deformity with aplasia of the cruciate ligament and ball and socket joint configuration, the frontal plane instability can lead to recurrence of axial malalignment after deformity correction [13].
Intramedullary lengthening nails
In moderate deformities with no or mild clinical instability,
The nails show faster rehabilitation with higher knee range of motion, better callus formation and less complications compared to external fixation [22].
The development of new motorised intramedullary lengthening nails enables deformity correction and limb lengthening with higher patient satisfaction and comfort than with external fixators [23].
The use in congenital limb deficiency has been described for the FITBONE nail (Wittenstein Intens GmbH, Igersheim, Germany) [22, 24–26], the PRECICE nail (NuVasive, San Diego, CA, USA) [16, 27–29] and the Phenix nail (Phenix Medical, Paris, France) [30].
The limitations of lengthening nails should be kept in mind, as severe cruciate aplasia and joint incongruity (ball and socket joint) can lead to subluxation. Cases of subluxation during lengthening with motorised intramedullary lengthening nails have been reported [16, 28].
Shabtai et al. [16] presented the results of 21 patients with congenital leg length discrepancy treated with the PRECICE lengthening nail and a preventive brace. Three of the 21 patients had prior complex knee reconstruction as preparation for further lengthening procedures. One patient had a subluxation of the knee during lengthening.
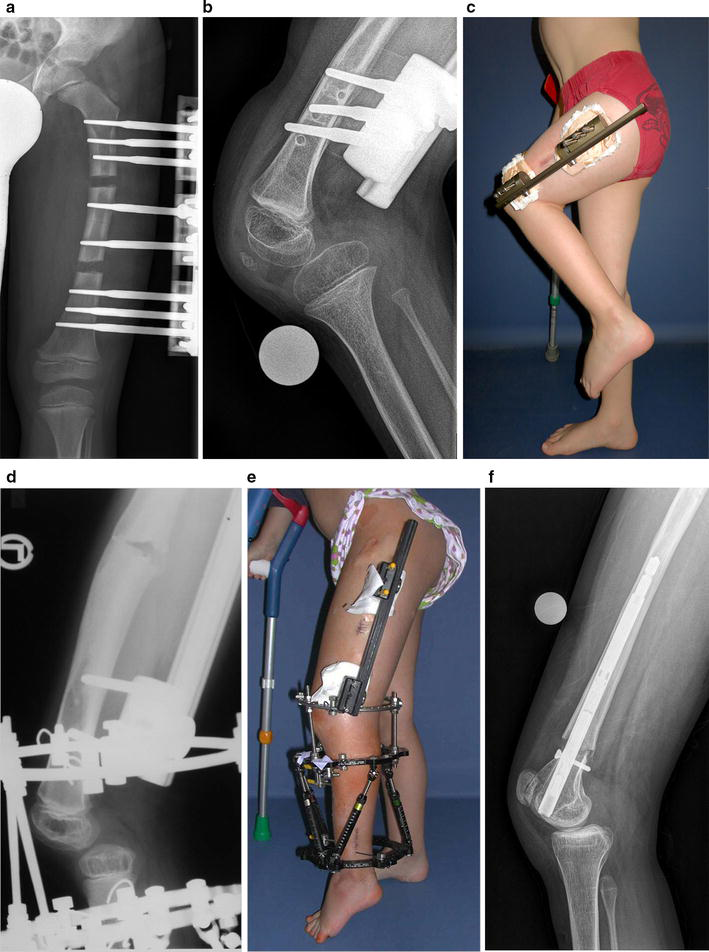
We use the PRECICE nail in congenital deformity without or with minor instability in combination with an above-knee orthosis (Fig. 3c) and weekly radiographic follow up. Since 2013, a total of 57 PRECICE nails have been implanted in 54 patients. Eight of these patients had CFD and/or FH with leg length discrepancy. One patient had early subluxation of the knee despite the use of a knee extension brace (Fig. 2f).

This 16-year-old female patient with CFD and FH had multiple prior surgical procedures for deformity correction and hip and knee stability. The remaining growth potential was successfully used for guided growth (
A noteworthy disadvantage of the PRECICE nail is high hardware costs. However, the nail gives various options such as retro- or antegrade femoral approach, trochanteric or piriformis femoral entry point and is available in different diameters and nail lengths. Therefore, it enables us to choose an optimal nail and surgical approach for each case.
Nevertheless, knee instability remains a huge concern in lengthening with nails. We recommend day- and night-time use of an extension brace during lengthening with an intramedullary lengthening nail. However, there are no studies on the effectiveness, optimal type (inclusion of ankle joint or pelvis) and wearing time of these braces. In the presence of significant knee instability in lower limb deficiency, lengthening with external fixation and bridging of the knee remains the gold standard of treatment.
In case of lengthening-related subluxation
The prediction of an individual's risk for subluxation in patients with CFD/FH remains difficult or impossible. It is necessary to detect
Knee range of motion during lengthening procedures of the femur with external fixation is limited during treatment and needs several months to recover [31].
In the case of severe flexion deformity or subluxation, it is advisable to temporarily
Motorised nails such as the PRECICE [16] and Phenix nails [30], as well as most of the external fixators, allow controlled
Furthermore, various
Conclusion
Knee joints of patients with congenital limb deficiencies show individually highly variable grades of instability. The knee function in daily activity seems to be nearly normal, even with knee abnormalities such as cruciate ligament aplasia and dysplasia of the joint surfaces. The instability might be relevant in sports activity, but further studies on this topic are needed. However, special attention is necessary prior to lengthening and deformity correction. Preoperative radiographic assessment is essential and clinical assessment of instability is obligatory. The development of new lengthening devices enabled us to correct congenital limb deficiencies with higher patient satisfaction and comfort. Irrespective of the applied method, high functional outcome can only be achieved by obeying the general rules of leg lengthening, with the highest aim of preventing the joint sustaining any damage during the lengthening procedure. In cases of severe flexion contracture or knee subluxation during lengthening, we recommend to stop lengthening or transiently shorten the bone to protect the knee joint from further damage. Intensive physical therapy and the use of a knee extension brace can help to prevent and treat subluxation. Adequate surgical techniques, preventive measures and early detection of signs of subluxation can lead to good functional results in patients with congenital limb deficiency.