
Abstract
Osteochondritis dissecans of the knee is an idiopathic, focal, subchondral-bone abnormality that can cause instability or detachment of a bone fragment and overlying articular cartilage, with subsequent progression to osteoarthritis. The degree of lesion instability is best assessed by magnetic resonance imaging. Unstable lesions require operative management with fragment fixation.
Introduction
Osteochondritis dissecans (OCD) of the knee is an idiopathic, focal, subchondral-bone abnormality that can cause instability or detachment of a bone fragment (or progeny) and overlying articular cartilage, with subsequent progression to osteoarthritis. A histological study evaluated osteochondral plugs from the center of OCD lesions. 1 A cleft was visible between the progeny and the surrounding (parent) trabecular bone. Interestingly, the progeny had not always been rated as unstable at arthroscopy despite being clearly separated from the parent bone. Thus, arthroscopic instability may be a delayed finding compared to the natural course of the condition. The subchondral bone was fractured and the progeny necrotic, although which of these two abnormalities occurred first was unclear. The progeny either undergoes reossification followed by incorporation or remains separated, as in a non-union, and eventually becomes loose.
Despite advances in our understanding of this condition, many issues remain unresolved; particularly the pathophysiology, indications for magnetic resonance imaging (MRI), and MRI signs of instability. 2
Radiographs
An antero-posterior view, a lateral view, and a notch view of the knee should be obtained. A skyline view is required if an OCD lesion of the patella or trochlea is suspected.
A simple radiographic three-stage classification was suggested at the 2005 SoFCOT (Société Française de Chirurgie Orthopédique & Traumatologique) symposium. The stages are focal lucency, attached fragment, and detached fragment, defined based on the bone trabecula abnormalities, irrespective of the condition of the overlying cartilage and viability of the fragment. 3 The Cahill and Berg classification separates the antero-posterior view into five segments, from medial to lateral. 4 On the lateral view, the Harding’s classification distinguishes anterior (A), middle (B), and posterior (C) sites, based on the Blumensaat line and on the tangent to the posterior femoral cortex. 5 The surface widespread availability of digitized imaging systems. Finally, skeletal maturity should be assessed, and the patient classified as having open, closing, or closed physes.6,7
OCD must be differentiated from simple irregularity of the posterior femoral condyle contours, which is a normal variant seen in patients with open physes, between 6 and 10 years of age. In contrast to OCD, there is no surrounding sclerotic rim and it attenuates over time.
Standard radiographs ensure the diagnosis of OCD and are useful for monitoring the healing of the lesion. However, several parameters cannot be assessed, including the condition of the overlying cartilage, and of the interface with the parent bone, defining instability. Moreover, poor reliability was demonstrated for the radiographic evaluation of the radiodensity of the lesion. 7
MRI
MRI is the most informative investigation in OCD, provided specific sequences are obtained. MRI is not performed systematically. Small volume cases with open physes do not require first-line imaging studies other than radiographs. Criteria for MRI are surface area greater than 350 mm² or closed physes and symptoms persisting after 6 months of sports restriction.
Technical considerations
Depending on the location of the lesion, images are acquired in at least two planes. T1-weighted sequences should be obtained with good tissue resolution to allow a detailed analysis of the bone signal. T2-weighted sequences with fat signal suppression are preferable over proton density-weighted sequences, which are less specific for detecting fluid at the epiphyseal bone interface. Three-dimensional gradient echo sequences with various fat suppression techniques provide a detailed assessment of the cartilage and differentiate the epiphyseal cartilage from the surface cartilage by showing a thin low-signal line between the layers (Figure 1). With T2* mapping, this type of sequence shows whether the fragment is composed of cartilage or bone. 8 High magnetic field (1.5 T and above) offers high-resolution imaging and high diagnostic accuracy; however, there are no clear advantages of using 3T as compared to 1.5-T MRI in children with OCD.9,10

MRI, coronal view, gradient echo sequence with fat signal suppression: thin line of low signal between the epiphyseal cartilage and the surface cartilage.
MRI signs
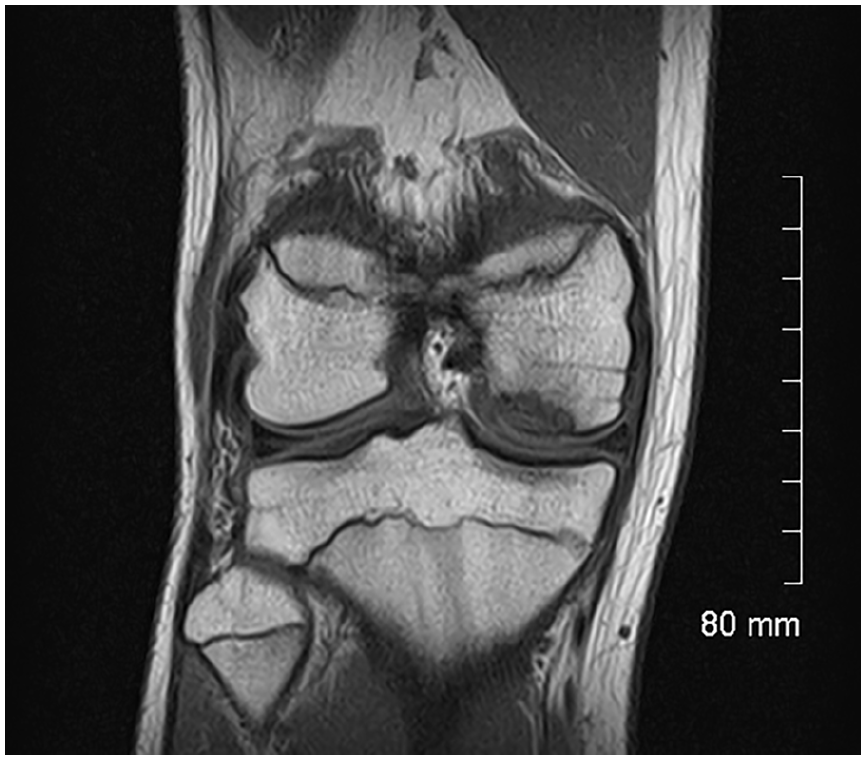
The progeny is usually hypointense on T1 images (Figure 2) and heterogeneous on T2 images (Figure 3). MRI provides a better assessment of volume and may show an osteochondral fragment extending beyond the normal epiphyseal contour, a defect at the site that shed the fragment, or loose fragments within the joint cavity (Figure 4). The Oreo cookie sign is represented by a curvilinear hyperintense T2 signal at the interface of the progeny and the parent (cookie cream), sandwiched between two layers of hypointense–hypointense signal (cookie wafers) (Figure 5). The presence of focal cysts at the interface between progeny and parent bone suggests chronicity.
MRI, coronal view, T1-weighted sequence: low-signal fragment within the subchondral bone.

MRI, sagittal view, proton density sequence with fat signal suppression: heterogeneous low signal from the fragment within the subchondral bone on the T2 image.

MRI, coronal view, proton density sequence with fat signal suppression: fragment protruding beyond the epiphyseal contour with the disappearance of the overlying surface cartilage.
Oreo cookie sign: curvilinear hyperintense T2 signal at the interface of the progeny and the parent, sandwiched between two layers of hypointense–hypointense signal.
In doubtful cases, MRI differentiates OCD from a simple irregular ossification. In this last case, there is no extension to the notch, and neither is there any intraosseous edema. Other findings include a jigsaw-puzzle appearance of the subchondral bone and spicules (secondary ossification centers). The surface of the overlying cartilage appears normal (Figure 6).

Irregular ossification of the lateral condyle. Differential diagnosis of OCD.
Prognosis
An abnormal surface cartilage is recognized as a factor of adverse prognostic significance. 11 It is normally thin, regular, and pale gray. The cartilage overlying an OCD lesion may be thicker and may generate a lower intensity and more heterogeneous signal, indicating chondral edema. At a more advanced stage, cracks may develop, generating flaps or defects.
An assessment of the interface between progeny and parent bone is crucial, as it indicates whether the course is progressing toward separation or reintegration of the fragment. Normal signal from the basal side suggests reintegration. In contrast, a high-signal rim on T2 images indicates either granulation tissue or synovial fluid.
Instability
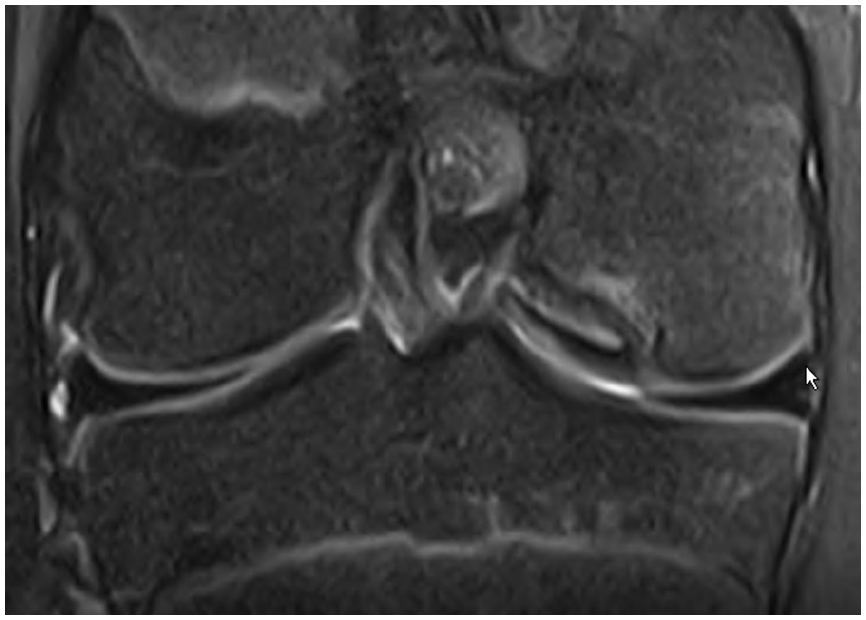
Instability is the key factor governing the prognosis and treatment decisions. De Smet et al. 11 first defined instability based on four criteria evaluated on T2 images: (1) high signal intensity line beneath the lesion, (2) cystic area beneath the lesion, (3) high signal intensity line through the articular cartilage, and (4) focal articular defect. These criteria were established using arthroscopy findings as the gold standard, with instability defined as a break in the articular cartilage or a mobile flap detected using the arthroscopic probe. Both signs had 100% sensitivity and specificity in patients with closed physes and 100% sensitivity with only 11% specificity in those with open physes. 12 In this last group, however, specificity reached 100% in patients meeting the following MRI criteria: intensity of the high-signal line beneath the lesion identical to that of the adjacent joint fluid, second outer rim of low signal intensity (Figure 7), and multiple breaks in the subchondral bone plate. Cysts indicate instability when multiple or larger than 5 mm in diameter 12 (Figure 8).

MRI, coronal view, T2-weighted sequence with fat signal suppression: double line with an internal high-signal line of fluid intensity rimmed by a low-signal line, indicating instability.

MRI, sagittal view, T2-weighted sequence with fat signal suppression: two cysts around the fragment.
The low specificity of MRI in patients with open physes may be explained by the inverse relationship between the thickness of the epiphyseal cartilage and age. In young patients, cracks or mobility may be absent due to the thick cartilage layer overlying the progeny, even if the latter is mobile. Arthroscopic signs of instability would then arise later than MRI signs. The above-mentioned histological findings support this hypothesis.
Older age predicts instability. In a study of 119 patients (68% of boys) by Siegall et al., 13 MRI instability was extremely uncommon in patients younger than 13 years of age (2/71, 3%) but was consistently present in those older than 17 years of age (7/7, 100%).
A recent multicenter study by Fabricant and the Research in OsteoChondritis of the Knee (ROCK) Study group have reported a significant inter-observer variability regarding interface characteristics, progeny, and parent bone measurements and qualities, with reliability being moderate at best. 14
Classification
Novel Kocher three-grade classification considers instability criteria (grade III) and proved reliable and simpler than the classic Hefti classification.15,16 It has substantial inter-rater reliability and strong correlation with arthroscopic findings (Figure 9). 17
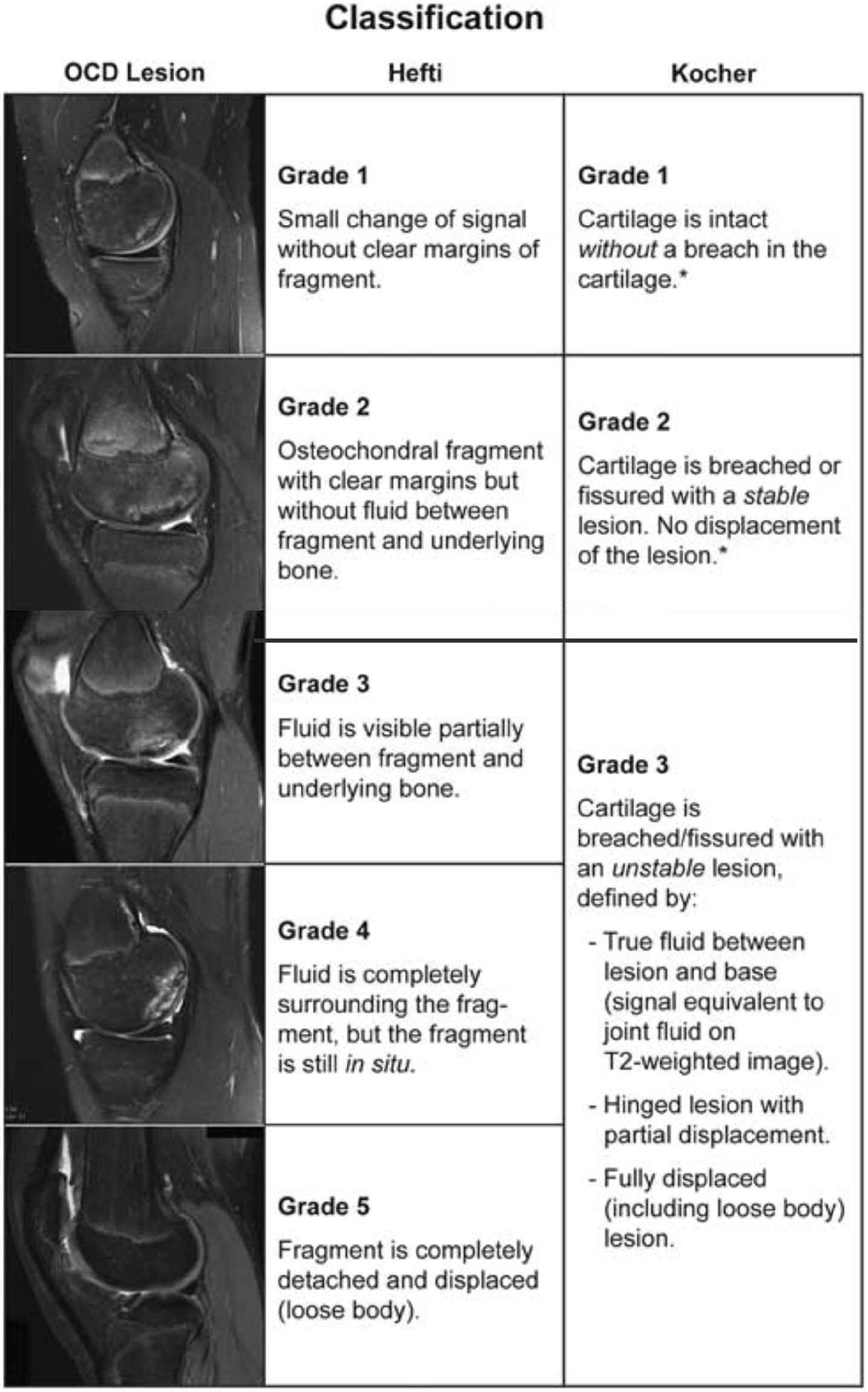
Kocher MRI classification.
Treatment considerations
Arthroscopy is currently the reference standard for assessing instability. As indicated above, however, we advocate the use of MRI as the reference standard, given its greater sensitivity. Instability requires fixation as simple drilling would be insufficient and would likely fail to provide healing. This concept is emphasized in a case example. A 13-year-old girl was complaining of left knee pain with positive Wilson test despite 6 months of sports restriction. MRI displayed instability signs (Kocher grade III) (Video 1). Arthroscopy showed a shadow sign with no sign of instability (cleft or ballotable progeny) according to the Rock classification (Video 2). It was decided to proceed with a biologic fixation using an Osteochondral Autograft Transfer (OAT), based on MRI criteria rather than arthroscopic findings. Probing of the progeny through the recipient site demonstrated actual mobility of the progeny. The autograft was placed and transarticular drilling was performed, providing complete healing (Figure 10).
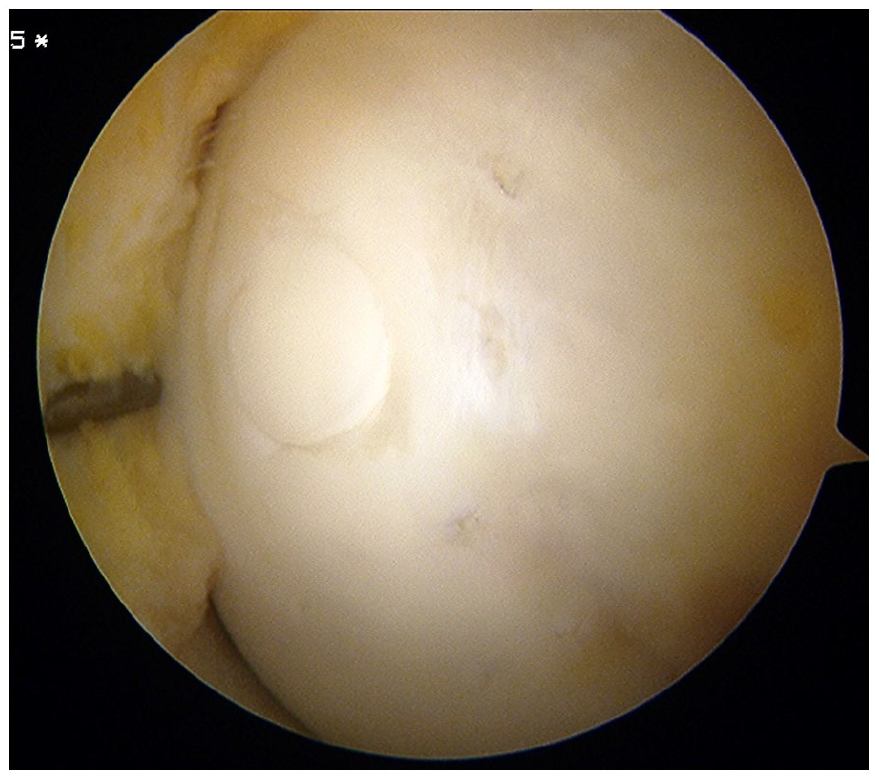
Case example. Arthroscopic view after OAT and transarticular drilling.
Some authors have also recommended suturing the anterior horn of the meniscus (“meniscopexy”) to prevent a door stop phenomenon onto the femoral condyle, occurring in knee extension. 18
Conclusion
The MRI signs of instability have been redefined. The line beneath the fragment should have the same high-signal intensity as the adjacent joint fluid. A low-signal outer rim surrounding the high-signal line should be visible, and multiple breaks in the subchondral bone. Cysts indicate instability if they are multiple or larger than 5 mm in diameter. The treatment should be determined based on the stage of the lesion. Fixation is required if the lesion is unstable by MRI or arthroscopy. Mosaic osteochondral transplantation is a technique of choice. Follow-up must be provided until complete radiographic healing of the lesion.
Footnotes
Author contributions
F.A., M.S.K., and M.T. contributed in the study design; M.S.K. and F.A. participated in data collection; M.T., F.A., and M.S.K. participated in data analysis and interpretation; F.A. and M.S.K. drafted the article; M.T., F.A., and M.S.K. participated in final revision of the article. All authors approved the final version of article for submission.
Compliance with ethical standards
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
The informed consent from all participants/their parents/carers was waived due to the retrospective nature of this study.
Submission declaration
This article has not been published previously and is not under consideration for publication elsewhere. The publication of this article has been approved by all authors and by the responsible authorities where the work was carried out. We declare that, if accepted, this article will not be published elsewhere, including electronically in the same form, in English or in any other language, without the written consent of the copyright holder.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.