
Abstract
Background:
Patellofemoral instability is a frequent cause of referral in pediatric sports medicine. Isolated medial patellofemoral ligament reconstruction is widely used and provides satisfactory outcomes with a low failure rate. Given the success of this surgical technique, the literature on medial patellofemoral ligament reconstruction failures in the pediatric population is limited. Moreover, given the multifactorial nature of patellofemoral instability, the heterogeneity of the current literature, and the paucity of pediatric studies, medial patellofemoral ligament reconstruction failures are often difficult to analyze.
Methods:
The purpose of this study was to retrospectively review the associated risk factors, surgical management, and the clinical outcomes at 2-year follow-up of skeletally immature patients that presented to our clinic with a failed medial patellofemoral ligament reconstruction.
Results:
Of the 181 cases in 155 patients included in this study, treatment failed in 12 (7%). All 12 patients presented with at least one risk factor for patellofemoral instability, the most common being trochlear dysplasia and a high-grade J sign.
Conclusions:
We conclude that isolated medial patellofemoral ligament reconstruction for patellofemoral instability in children has a low failure rate. Clinicians must assess pre-operative risk factors before surgical treatment is considered. A high-grade J sign and high-grade trochlear dysplasia were associated with medial patellofemoral ligament reconstruction failure in this cohort. Tailoring treatment to patients’ associated risk factors selection may improve outcomes.
Introduction
Patellofemoral instability (PFI) is a frequent cause of referral in pediatric sports medicine. Although most patients are managed successfully non-operatively with physiotherapy and knee bracing, many are treated operatively. 1 Isolated medial patellofemoral ligament (MPFL) reconstruction is widely used and provides satisfactory outcomes with a low failure rate.2–5
Given the success of this surgical technique, the literature on MPFL reconstruction (MPFLR) failures in the pediatric population is limited. In their 2013 and 2018 studies, that included 46 pediatric cases combined, Nelitz et al.6,7 reported a 0% MPFL failure rate at 2-year follow-up when using MPFLR technique that maintained the distal femoral growth plate and a pedicled superficial quadriceps tendon graft. However, a 2016 study by Lind et al., describing an MPFL technique with a gracilis tendon autograft and soft tissue fixation in 24 pediatric cases, reported an MPFL failure rate of 21%. They discussed that this could result from soft tissue fixation versus bone tunnel fixation, as it could provide insufficient dynamic biomechanical stability. 8 Moreover, in a study including 54 skeletally immature knees that underwent an MPFLR with hamstring graft and short patellar and femoral sockets with tenodesis screws for fixation, Uppstrom et al. 9 reported an MPFL failure rate of 9.3%.
Failures are difficult to analyze given the multifactorial nature of PFI and the relatively low failure rate, reported between 0% and 16.6% (mean 4.3), according to a recent systematic literature review. 10 Moreover, there is a paucity in the literature regarding the risk factors and treatment of failed MPFLR. The purpose of this study was to retrospectively review the associated risk factors, surgical management, and the clinical outcomes at 2-year follow-up of skeletally immature patients that presented to our clinic with a failed MPFLR.
Material and methods
Study cohort
We retrospectively reviewed the records of all pediatric patients treated operatively in Toulouse University Children Hospital with primary isolated MPFLR for recurrent PFI from 2010 to 2020, with a minimum clinical follow-up of 2 years. All cases of surgical revision for failure were isolated. Preoperative risk factors for PFI, and surgical technique of both primary and revision procedures were considered. Descriptive statistics were performed.
Surgical technique
The procedure was performed as a day-case surgery under general anesthesia and after a Ropivacaine adductor canal nerve block. This is a multi-surgeon series including two MPFLR techniques. The most common was performed according to Chassaing and Trémoulet. 11 A free gracilis tendon autograft is looped around the soft tissues between layers 2 and 3, from the level of the medial epicondyle to a superiosteal tunnel at the superior and medial aspect of the patella and stitched to itself at 30° knee flexion (Figure 1). The medial retinaculum is plicated over the graft. A variant consisted of a bone tunnel fixation at the Schöttle’s point with an absorbable interference screw. This latter technique was only performed in skeletally mature individuals. 12 Lateral retinaculum was released arthroscopically only when considered tight. Patients were encouraged to bear weight immediately with an extension knee brace maintained for 4 weeks before starting physiotherapy including range of motion (ROM) and muscle strengthening. Sports activities were resumed gradually after 3 months, provided functional recovery was deemed sufficient by the attending surgeon.
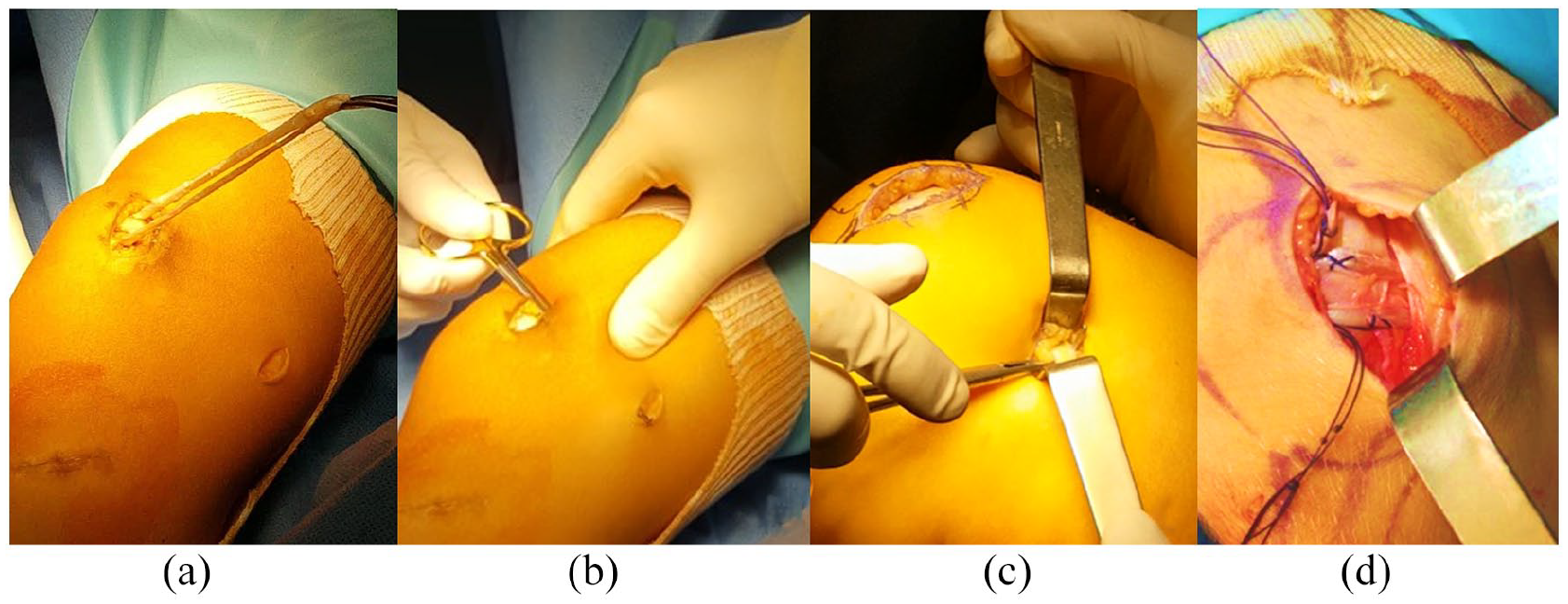
MPFLR technique according to Chassaing et al. (a and b) Subperiosteal loop at the superior and medial aspect of the patella. (c) Soft tissue loop at the medial femoral epicondyle. (d) The graft is tightened and stitched to itself at 30° knee flexion.
Results
A total of 181 primary isolated MPFLR procedures were performed in 155 patients (97 left, 58 right, 26 bilateral). There were 107 girls and 48 boys, whose mean age at the time of surgery was 14.3 years (range 8–18). Treatment failed in 12 patients (7%). All 12 patients presented at least one risk factor for PFI, trochlear dysplasia and high-grade J sign being the most common (Table 1). Mean time to revision surgery was 30 months (range of 6–96). All but one revision combined several surgical techniques, the most common being redo MPFLR using semi-tendinosus autograft and tibial tuberosity osteotomy (TTO).
Failures of isolated MPFLR for patella femoral instability.
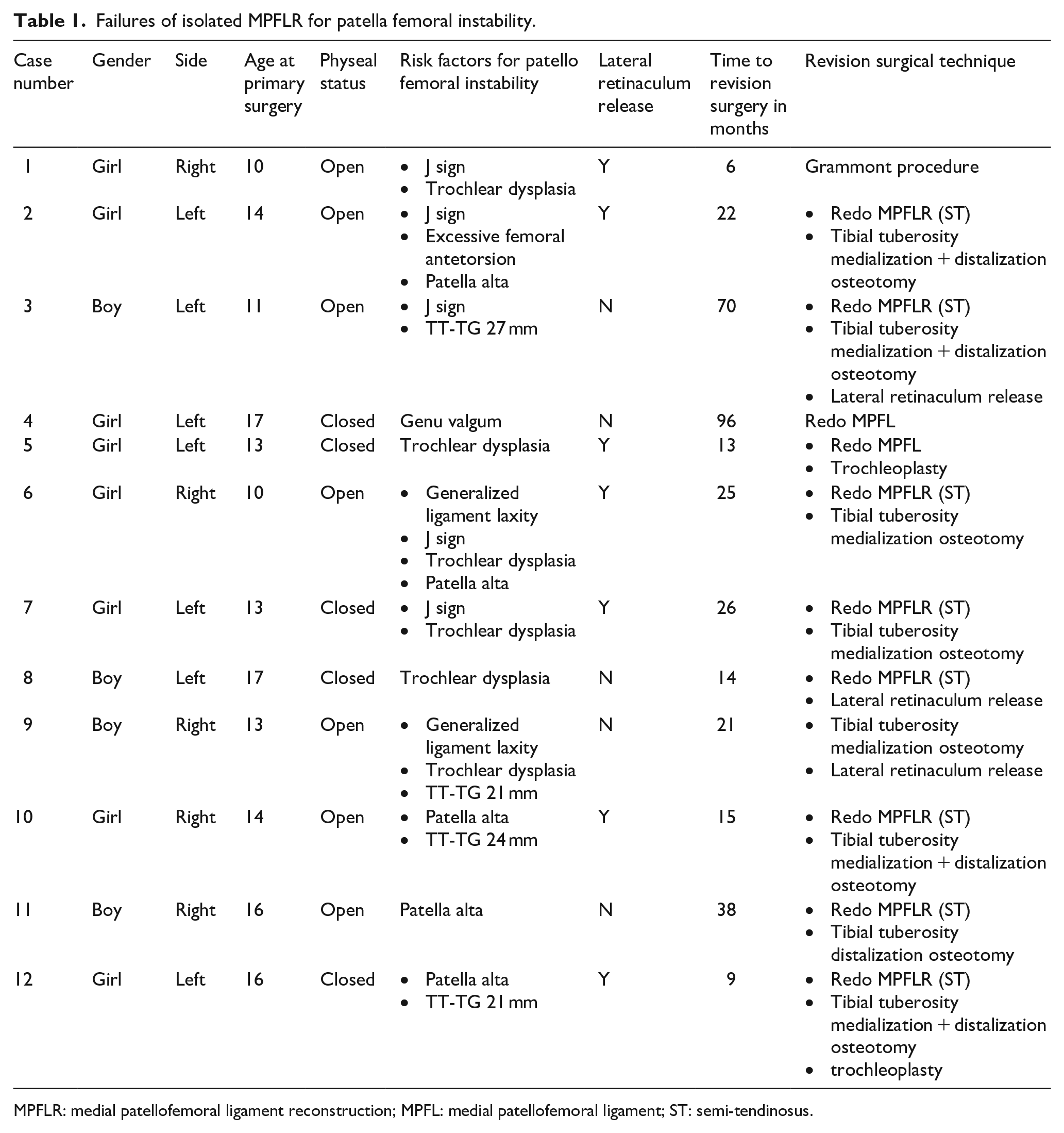
MPFLR: medial patellofemoral ligament reconstruction; MPFL: medial patellofemoral ligament; ST: semi-tendinosus.
Discussion
We confirm, according to the recent literature and our own experience, the relative low failure rate of primary isolated MPFLR for PFI in children. This treatment option is supported by the fact that MPFL is torn in nearly all cases of acute patellar dislocation, and medial MPFL deficiency is present in all cases of recurrent patellar dislocation. MPFLR is a soft tissue procedure that fails to address the underlying bony pathologic conditions that contribute to PFI. However, it can restore satisfactory patellar tracking and successfully prevent patellar dislocation (Figure 2). This procedure is simple and avoids added operative time and potential morbidity of additional procedures such as osteotomies. 5
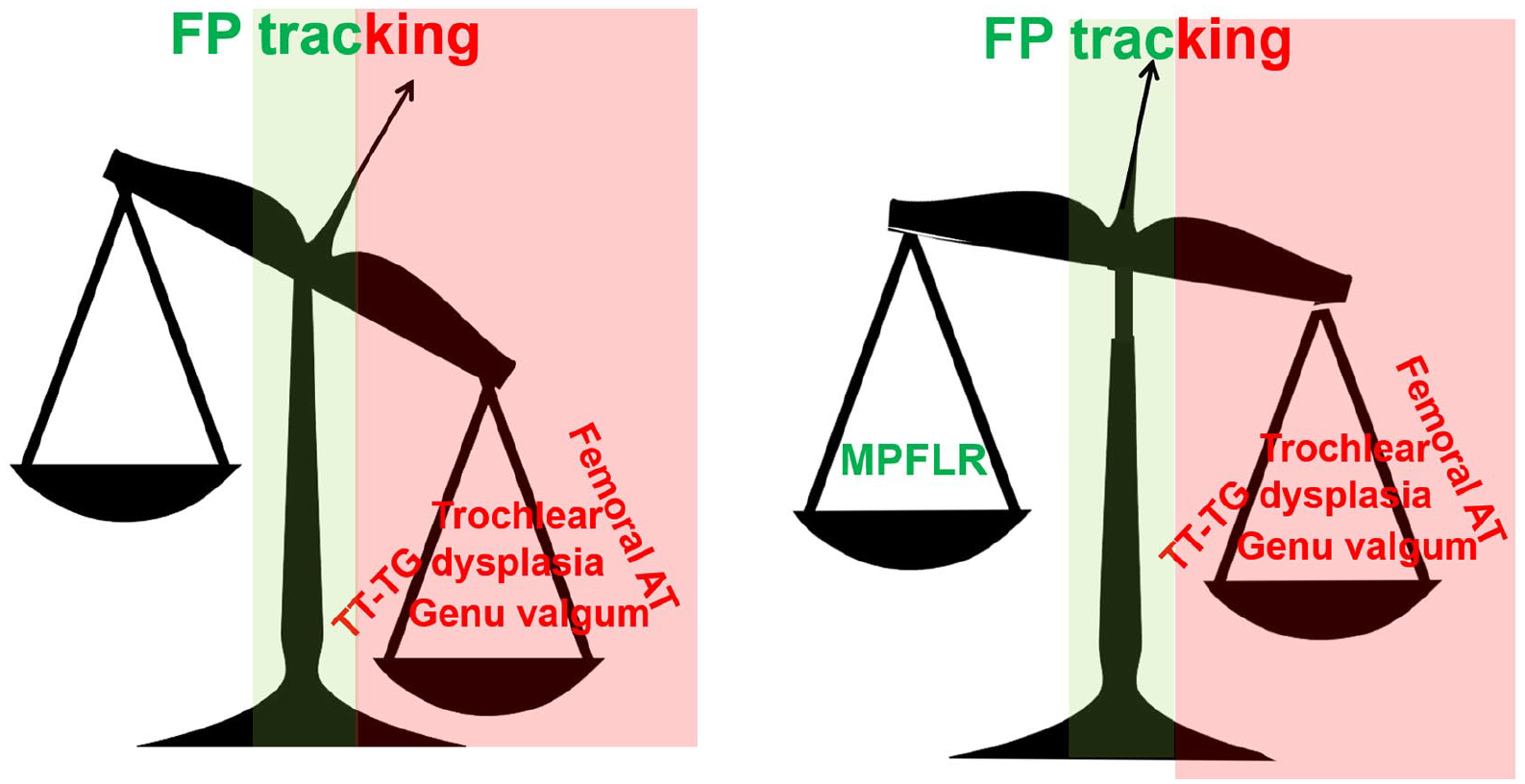
Treatment concept of improving patellar tracking and preventing patellar dislocation with MPFLR in isolation, despite its multifactorial origin.
Management of failed MPFLR starts with investigating the reasons for failure. One should inquire whether physiotherapy has been followed as planned, including vastus medialis strengthening, proprioception, and assisted return to sport, at least for 2 months. Clinical examination may reveal muscle wasting. In this situation, surgical revision is not systematically warranted, and adequate physiotherapy is indicated first. In case primary MPFLR has been performed using a femoral bone fixation, the correct placement should be checked on a lateral view radiograph and/or magnetic resonance imaging (MRI). Femoral tunnel malposition is reported as a technical cause of failure when the center of the tunnel is > 10 mm from Schottle’s point, or even when > 5 mm.13–15 Moreover, all predisposing factors for PFI need to be assessed, including but not limited to elevated tibial tubercle to trochlear groove distance (TT-TG), femoral anteversion, trochlear dysplasia, and patella alta.16,17
Although TT-TG distance is a measurement that has been scrutinized in the literature due to its multiple limitations, it remains as one of the most common anatomical risk factor for PFI.18–20 As described by Dickens et al., 21 when treating skeletally immature patients, TT-TG should be evaluated utilizing an age-based approach. In a study including 44 knees of adolescents and young adults, Kita et al. 22 found that trochlear dysplasia and increased TT-TG were associated with failed MPFLR. However, in a 2018 study including 27 knees, Pesenti et al. 23 reported no association between TT-TG and clinical outcomes following isolated MPFLR in pediatric patients.
In addition, rotational malalignment in the form of femoral anteversion has been extensively described as an anatomical risk factor for recurrent PFI.11,24,25 A 2020 study by Zhang et al. 26 that included 70 knees reported that patients with high femoral anteversion (>30°) had lower post-operative clinical outcomes following MPFLR and combined TTO.
Similarly, trochlear dysplasia is one of the leading causes of PFI. 27 Described as flat or prominent trochlea, trochlear dysplasia can present with varying severity Type A displaying a shallow trochlea to Type D showing asymmetry of trochlear facets and a vertical join and cliff pattern. 28 Trochlear Dysplasia is often treated with a trochleoplasty, however, given that it may compromise bone growth of the distal femur, clinicians should defer this procedure until skeletal maturity. 29
Patella Alta, defined as a patella that is displaced proximally in the trochlear groove, has been found to increase the likelihood of recurrent patellar dislocations.17,30 Previous studies have shown that an isolated MPFLR can decrease patella alta in patients with PFI. In a study by Fabricant et al. 31 that included 27 pediatric patients, patellar height significantly reduced (p < 0.001) after MPFLR reconstruction without a distal realignment procedure. Moreover, in a study that included 38 pediatric patients, Lykissas et al. 32 observed similar outcomes when comparing pre-operative and post-MPFL reconstruction patellar height using lateral knee radiographs.
It is unclear what threshold is deemed ‘‘critical’’ for each established risk factor in isolation, let alone when risk factors are present in combination. Based on the multifactorial nature of PFI, the heterogeneity of the current literature, and the paucity of pediatric studies, it is difficult to draw distinct conclusions. Several recent studies have reported conflicting conclusions regarding the value of each risk factor and its role in leading to failure after isolated MPFLR.10,30,33 However, the most important risk factors for failure emerging from the literature and our own experience are severe trochlear dysplasia (Dejour B and D) and malposition of femoral tunnel.2,10 When a predisposing factor is present and grossly abnormal, that is TT-TG > 25°, excessive femoral anteversion > 30°, patella alta with caton-deschamos index > 1.4, it is recommended to address PFI by more extensive procedures than MPFLR in isolation.26,34
Revision for failed primary MPFLR should be tailored to the failure analysis. It generally includes revision MPFLR combined with one or several other procedures. Various grafts are available for revision MPFLR: gracilis or ST, quadriceps tendon or tendon allograft. TTO (medialization and/or distalization) is the most associated procedure. 35 In case the patient is not yet skeletally mature, soft tissue transfer is indicated according to the Grammont technique. 36 Trochleoplasties should also be deferred until skeletal maturity. Zimmermann et al. 37 have reported on 28 MPFLR revisions (16 for recurrent instability, 12 for patella femoral pain or limited ROM) performed in young adults on average 31.2 months (range 6–72) from the primary surgery. Revision procedures performed included redo MPFLR, TTO, release of the MPFLR, deepening trochleoplasty and femoral de-rotation or varization osteotomy. Tailored revision surgery for failed MPFLR yielded significant improvements in the patient reported outcome measures. In addition, the patients who underwent a revision surgery due to recurrent PFI achieved higher quality of life score values than the patients who underwent a surgical revision due to patella femoral pain and/or limited knee joint ROM. Recurrent patellar dislocations were not observed during the follow-up, but three patients complained of temporary patellar subluxations. 37
The current series bears several obvious weaknesses linked to its retrospective and record-based nature and the absence of patient-reported outcome measure questionnaires. Failure rate may have been underestimated as recurrence may have occurred after the 2-year minimum follow-up threshold. Definition of failure was based on surgical revision for recurrence only, which is restrictive. Some studies have also considered residual pain or knee stiffness as failure. MPFLR was performed according to the Chassaing technique. Alternatively, MPFLR can be performed in skeletally immature patients according to the Green method. 38 The two ends of a free hamstring autograft are docked in the superior-medial patella using short sockets, and the femoral attachment socket is placed just distal to the physis.
Conclusion
Isolated MPFLR for PFI in children has a low failure rate. Preoperative risk factors are high-grade J sign and high-grade trochlear dysplasia. Optimizing patients’ selection and may further improve the results.
Footnotes
Author contributions
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: F.A. is a paid consultant for Zimmer Biomet. D.W.G. is a paid consultant for Arthrex and has royalties or licenses with Arthrex and Pega Medical.
Ethical approval
This research involved strictly human participants. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained in each case from both the patient and the parents.