
Abstract
The treatment of Legg-Calvé-Perthes disease remains controversial. The aim of this survey was to ascertain the current management strategies of this condition amongst UK paediatric orthopaedic surgeons, with particular regard to containment procedures in the fragmentation phase. Questionnaires were distributed at the January 2006 meeting of the British Society for Children's Orthopaedic Surgery (BSCOS) and was posted to all absent members. The results showed a great deal of variability not only in the treatment of Perthes disease, but also in the decision-making processes. Consideration must now be given to a carefully constructed national multi-centre prospective randomised controlled study into the optimum management of this disease
Introduction
Legg-Calvé-Perthes disease is a childhood hip disorder occurring most commonly in the age range of 4–8 years [1]. It was first described in 1910 by Legg, Calvé, Perthes and Waldenstrom, and is characterised by transient avascularity of the femoral head. Eventually, the head revascularises, dead bone is replaced and remodelling occurs. The outcome in terms of the resultant shape of the femoral head is difficult to predict, as it varies from patient to patient and depends partly on age at presentation, the proportion of the head involved and the severity of the disease. It is, therefore, difficult to formulate individual patient treatments. Also, most studies of current treatment methods lack interrater and intrarater reliability of classifications of the extent of epiphyseal involvement and outcome measures, and all lack control groups. These factors make it difficult to support a “best” method of treatment.
The primary goals in the treatment of Legg-Calvé-Perthes syndrome are to prevent deformity, growth disturbance and resultant degenerative joint disease. During the early years, Legg, Calvé and Waldenstrom concluded that surgical treatment had little effect on outcome. Treatment methods were based on those used to treat tuberculosis of the hip, which included spica cast immobilisation, bed-rest, traction and weight-relieving caliper. The cornerstone of treatment for Legg-Calvé-Perthes syndrome is referred to as “containment.” This concept was originally described by Harrison and Menon [2] and Eyre-Brook [3].
The essence of containment is that, to prevent deformity of the diseased epiphysis, the femoral head must be contained within the depths of the acetabulum in order to equalise the pressure on the head and subject it to the moulding action of the acetabulum [4]. This may be achieved by operative or non-operative methods. Arthrography may be a useful adjunct in determining whether the head actually can be contained and, if so, in what position this is best accomplished [1, 5]. Rab [6], however, questioned the containment concept, and believes that femoral head reorientation (osteotomy) may improve femoral head stability when necrosis is limited, but is unlikely to reduce subluxation or collapse when extensive necrosis is present.
Some authors have reported satisfactory results with non-operative treatment, such as bracing and cast immobilisation [7, 8], but others disagree, stating that it is no better than no treatment at all [9].
Many investigators have reported good results with femoral varus osteotomies [10–12]. Others have recommended the Salter innominate osteotomy as an effective treatment alternative [10, 13, 14, 15]. Still, some follow more complex surgical interventions [16, 17, 18, 19].
However, some authors have shown no change in clinical results following femoral varus osteotomies or innominate osteotomies [20] and others found that the outcome was similar in both operative and non-operative management [12]. There is no clear universally accepted treatment strategy for Perthes disease, as evident from the above available studies.
Materials and methods
Questionnaires were designed with the help of the English South West Paediatric Orthopaedic group and a statistician (see Appendix). These were distributed at the January 2006 meeting of the British Society for Children's Orthopaedic Surgery (BSCOS) and was posted to all absent members.
There are 179 BSCOS members. Forty questionnaires were collected at the meeting and 48 questionnaires were returned by post, giving a 49% return. Eleven had retired and chose not to participate. This left 77 questionnaires for analysis.
Results
There was a wide variation in opinion about the management of Perthes disease. Regarding conservative management, 26% used abduction braces on occasion, while petri casts were used by 43% of members and the majority advised physiotherapy (90%).
Of the 77 members, three never performed surgery for early Perthes disease. Of the remaining 74 members who did perform surgery, nine (11%) felt that arthrogram was not required and, therefore, did not perform one prior to surgical procedure.
The need for an arthrogram was determined by several factors, which came under three headings in the questionnaire: history, examination and radiological features. Severity of symptoms, age, duration of symptoms and gender were considered to be factors on occasion by all surgeons, while on clinical examination, loss of abduction in extension was always considered to be a determining factor for the need for arthrogram by all of those who perform arthrograms. The other clinical indications were loss of hip flexion, loss of internal rotation in flexion, loss of adduction in flexion and limp, in descending order of importance. Obesity was considered as a very minimal determent for the need for arthrogram.
The radiographic signs were lateral subluxation, involvement of proximal head, lateral pillar height, calcification lateral to the epiphysis, metaphyseal reaction, horizontal growth plate, degree of fragmentation and subchondral fracture, in decreasing order of importance.
Forty-two surgeons (56%) performed 1–5 osteotomies per year, 15 surgeons (28%) performed 6–10 osteotomies and three (4%) performed more than 10 osteotomies per year (Fig. 1).
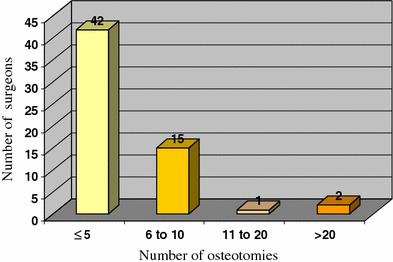
Number of osteotomies performed each year
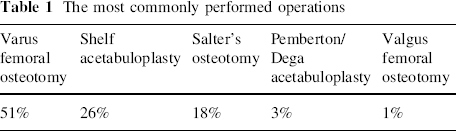
Fifty-one percent (51%) of surgeons intimated that varus femoral osteotomies are their most commonly performed operation. For shelf acetabuloplasty, Salter's osteotomy, Pemberton/Dega and valgus osteotomies, the figures were 26%, 18%, 3% and 1%, respectively (Table 1).
The most commonly performed operations
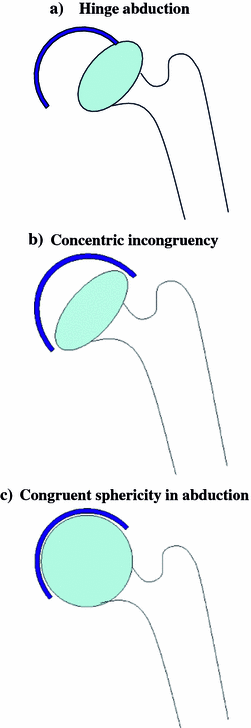
Contraindications to containment surgery were as follows: preoperative loss of abduction in extension (<30°) was an absolute contraindication for 24% of surgeons, 38% believed it would be contraindicated in more than half of all cases and 24% in less than half of all cases. Fourteen percent (14%) of surgeons considered the age of the patient to be a factor. Hinge abduction (Fig. 2a) was considered to be an absolute contraindication to containment surgery for 49% of those performing surgery, 8% never considered it a contraindication, while 11% sometimes considered it as a contraindication. Concentric incongruency (Fig. 2b) in abduction was considered as a contraindication to surgery by 12%, 16% believed it never to be a contraindication and 39% sometimes felt it to be a contraindication to containment surgery. One stated that this is the indication for containment. Thirty-one percent (31%) of surgeons followed a Herring philosophy, taking patients’ age and height of the lateral pillar into consideration. Three percent (3%) used a Caterall management strategy in addition. Others used some but not all of the “head at risk” signs to decide on intervention.
Discussion
As evident from the above survey, there is a wide variation of opinion regarding the management of Perthes disease amongst the paediatric orthopaedic surgeons of Britain. This reflects the confusion which exists in the literature on the subject. There is only one prospective multi-centre study on the effect of treatment on outcome in the literature [9]. Herring et al. [9] concluded in his prospective multi-centre study that the lateral pillar classification and the age at the time of onset of the disease strongly correlate with the outcome in patients with Legg-Calvé-Perthes disease. He showed that patients over the age of 8 years at the time of onset and with lateral pillar B group or B/C border group have a better outcome with surgical treatment than they do with non-operative treatment [9]. No such study has been carried out in the UK.
Consideration must now be given to a carefully constructed national multi-centre prospective randomised controlled study into the optimum management of this disease.