
Abstract
Purpose
Compare conservative and operative treatment in the most severely affected Legg-Perthes disease patients.
Methods
29 patients (14 conservative and 15 operative) with 32 affected hips (16 conservative and 16 operative) were evaluated, all Catterall 3 or 4. The conservative group, with a median age-at-onset of 4.8 (range, 2.5–9.5) years, was treated by a rigorous regime of traction in abduction for an average of two years. Follow-up was performed at a median of 28.6 (range, 17.4–31.6) years with a median patient age of 34.1 (range, 19.9–39.3) years. The operative group, with a median age-at-onset of 4.7 (range, 2.0–7.8) years, was treated by femoral varus derotation osteotomy. Follow-up was performed at a median of 14 (range, 8–21.4) years, with a median patient age of 20.7 (range, 12.8–28) years.
Results
Median age-at-onset (P = 0.16) and Catterall classification (P = 0.29) were comparable. No differences could be found for the Stulberg classification (P = 0.83), functional parameters (Harris Hip score and Merle d'Aubigné and Postel), and leg–length differences. Career choices were similar for both patient groups, as well.
Conclusions
Given methodological issues, femoral varus derotation osteotomy did not show apparent better results than the conservative containment regime in Catterall 3 and 4 patients with a median age-at-onset around 4.8 years. This result is fairly similar to recent literature suggesting a conservative approach in most severely affected patients with a young age-at-onset. However, based on unacceptable socioeconomic issues, the conservative regime evaluated in the present study cannot be justified, nowadays.
Introduction
In spite of extensive literature pertaining to Legg-Calvé-Perthes disease (LCPD) [1–3] the “best” treatment remains controversial. A recent study, evaluating the preferred treatment among paediatric orthopaedic surgeons, illustrated the disagreement in treatment choice [4]. Factors contributing to difficulties in evaluating the optimal treatment choice include diversity in patient inclusion, treatment type, and evaluation methods [5–9].
Optimal treatment choice is especially discussed in the most severely affected patients, i.e., Catterall 3 and 4 [10] or Lateral pillar grade C [11] and possibly the recently proposed B/C border group [12, 13], as these patients are associated with a poor long-term prognosis [9, 10, 14, 15]. Conservative and operative containment methods have been described extensively for these patients. Specifically, bed rest and abduction (with or without various periods of traction or casts) was one of the earliest containment methods employing weight-bearing relief until the femoral head had re-ossified [16–18]. This would prevent mechanical deformation of the femoral head and, hence, early osteoarthritis changes. This type of containment treatment was abandoned for various reasons, including questioned long-term efficacy, muscle disuse atrophy, high hospital costs and negative psychosocial effects related to prolonged treatment time [17, 19–23].
In the 1980s, operative methods (femoral and innominate osteotomy) to offer containment became more popular for these patient groups. Advocates of femoral varus osteotomy refer to the 70–90% satisfactory results [24–32]. Limited studies compare conservative treatment regime(s) with femoral varus osteotomy and report variable results [13, 14, 17, 20, 33–39].
The question of this retrospective study is: does femoral varus derotation osteotomy (femoral VDO) give better long-term results (radiological and functional) compared with prolonged traction in abduction for Catterall 3 and 4 patients. The abduction traction regime can be of particular interest, both from historical and follow-up perspective (median follow-up of 28.6 years).
Materials and methods
Study groups demographics and inclusion criteria
Two consecutive historical cohorts were included, i.e., a conservative (abduction traction) and operative (femoral VDO) group. Treatment choice was based on the Catterall classification [10] being the single accepted classification system at the time. Based on this classification and treatment protocol in our hospital, traction in abduction was prescribed for every Catterall 3 or 4 LCPD patient presenting between 1973 and 1985. From 1985, the treatment choice in our hospital changed to surgical treatment. The Catterall 3 and 4 patients included in this operative group were operated upon between 1985 and 1996. The disease was in its initial stage (fragmentation), and no patient had any of the exclusion criteria as described by Herring et al. [13].
The original population included 46 patients with 50 affected hips (22 conservative and 28 operative). Seventeen patients were lost to follow-up. Twelve of these patients (six conservative and six operative) could not be traced or did not reply to our repeated request for the follow-up visit at the outpatient clinic. Of the remaining five patients (all operative), one had passed away and four declined participation for various reasons not evidently related to the LCPD. Thus, a total of 29 patients (14 conservative and 15 operative) with 32 affected hips (16 conservative and 16 operative) were available for evaluation. For the conservative group, all but three patients had an age-at-onset less than 6 years (two patients 9.5 years, of which one was bilaterally affected, and one 7.3 years). In the operative group, all but two patients had an age-at-onset less than 6 years (both 7.8 years). Other characteristics of both study groups are described in Table 1. Both authors evaluated the Catterall classification for the patients in these two groups separately. Using Cohen's Kappa, a good agreement between both authors was measured (Cohen's Kappa of 0.73).
Patient demographics
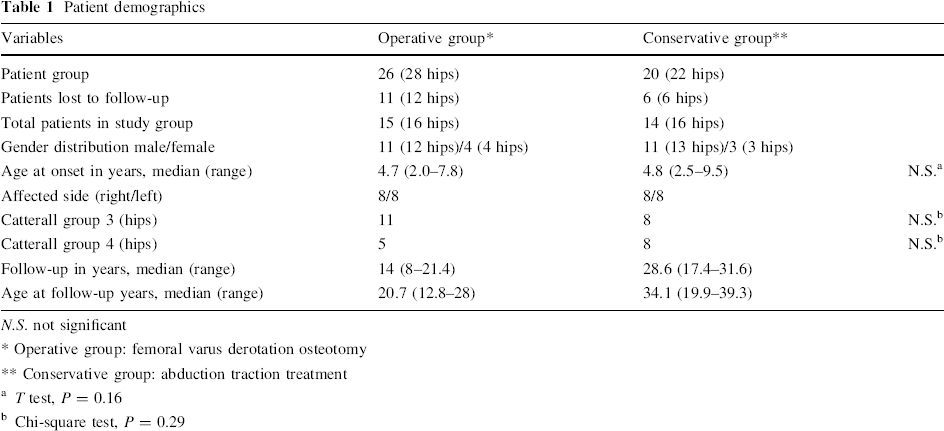
N.S. not significant
Operative group: femoral varus derotation osteotomy
Conservative group: abduction traction treatment
T test, P = 0.16
Chi-square test, P = 0.29
Conservative group
All patients were treated by a rigorous regime of traction in abduction. Treatment was performed in the Roessingh rehabilitation centre, Enschede, the Netherlands. Hip range of motion was recorded and pelvic anteroposterior and frog-leg lateral radiographs were made at about half-year intervals. Treatment was ceased when radiographs showed a reparative stage (Waldenström stage 3, i.e., re-ossification phase) [40]. In clinical practice this resulted in a treatment duration of about 2 years. During this period patients lived in the rehabilitation centre, including a school and all necessary living and social arrangements. No patient dropped out of the treatment because of patient or parental non-compliance.
Operative group
Femoral VDO was performed at the lesser trochanter level using blade-plate fixation. Surgical aim was a neck-shaft angle of 110° to 115° with a 30° endorotational change. Following surgery a 6 weeks traction regime was applied in all patients as part of standard postoperative treatment. After this period, partial weight bearing was allowed until osteotomy consolidation.
Radiological parameters
At follow-up, most recent anteroposterior and frog-leg lateral radiographs were reviewed and classified according to the Stulberg classification [41] as the primary outcome parameter. Presence of osteoarthritis signs was recorded as a secondary outcome parameter. Both independent authors, one experienced and the other fairly experienced, performed the radiological evaluation separately. In case of disagreement, re-evaluation was performed together to achieve mutual agreement. A reliability analysis of the Stulberg classification would be beyond the scope of the present study and thus was not performed. Wiig et al. [42] evaluated this issue, including a literature review, and found acceptable reliability when assessment is carried out by experienced examiners.
Clinical parameters
Harris Hip Score (HHS) [43] and modified scoring system of Merle d'Aubigné and Postel [44] were recorded. Furthermore, any leg length difference and choice of career was recorded. Several independent orthopaedic residents and orthopaedic surgeons performed clinical follow-up evaluation at the outpatient clinic. Prior to follow-up, the study was explained and informed consent obtained.
Statistics
To evaluate whether both study groups were comparable for age-at-onset and Catterall classification the independent T test and Chi-square test were performed, respectively. At follow-up, differences between both study groups regarding the Stulberg classification was evaluated using the Mann–Whitney U test. A P-value < 0.05 was considered significant.
Results
Radiological parameters
Catterall groups (i.e., 3 and 4) showed comparable results with regards to all studied parameters. Results are presented in Table 2. In the conservative group, 13 hips healed with Stulberg class II or I (nine class II and five class I), i.e., spherical congruency. Aspherical congruency was found in three, i.e., two Stulberg class III hips and one Stulberg IV hip. The only Stulberg IV case was a conservatively treated bilaterally affected male with an age-at-onset of 9.5 years. His contralateral side resulted in a Stulberg II. Clinically, at a follow-up of 27 years (patient age of 36.5 years), he scored maximum points on both the HSS and Merle d'Aubigné score. Two other patients with an age-at-onset above 6 years (9.5 and 7.3 years) healed in a Stulberg class III. No Stulberg class V (aspherical incongruity) was recorded in the conservative group.
Radiological and functional results at follow-up
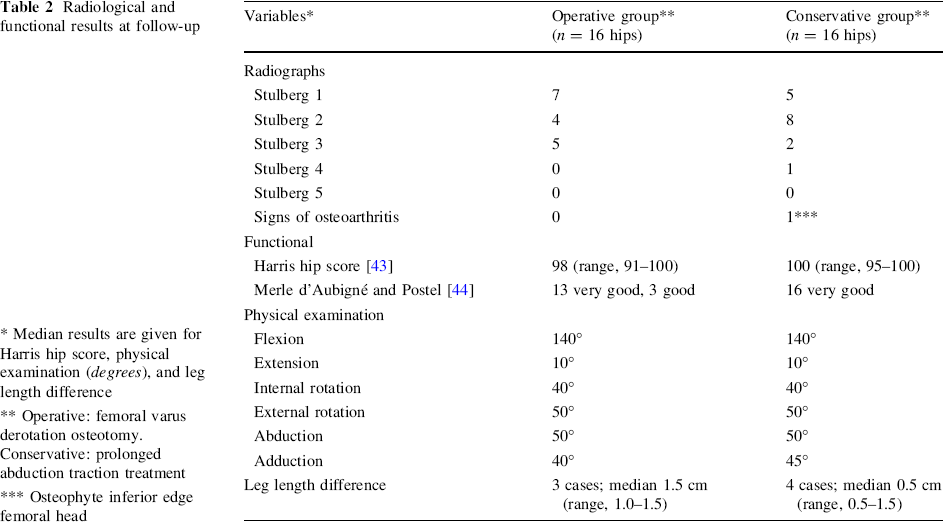
Median results are given for Harris hip score, physical examination (degrees), and leg length difference
Operative: femoral varus derotation osteotomy. Conservative: prolonged abduction traction treatment
Osteophyte inferior edge femoral head
In the operative group, 11 hips healed in a Stulberg class II or I (four class II and seven class I). Five Stulberg class III hips and no Stulberg IV or V were recorded. All but two of the operated patients had an age-at-onset less than 6 years (both 7.8 years). The hip of one of these patients healed in a Stulberg class I, the other hip in a Stulberg II. No statistical difference could be found between the two study groups regarding the Stulberg classification (Mann–Whitney U test, P = 0.83).
Osteoarthritis signs were found in one conservative hip showing a osteophyte at the inferior edge of the femoral head. No osteoarthritis changes were recorded in the operative group.
Clinical parameters
Results are presented in Table 2. The HSS [43] in the conservative group showed maximum score (100 points) in 14 out of the 16 hips. The remaining two hips scored slightly less (95 and 98). In the operative group, seven patients scored the maximum 100 points. The remaining nine hips scored between 91 and 99 points, still rated as good. Merle d'Aubigné and Postel [44] score in the conservative group showed an excellent score (18 points) in 13 and good score in three hips. In the operative group, 10 hips showed excellent score and six hips a good score.
Physical examination revealed no apparent differences between both groups, as well. Only minor, clinically asymptomatic, leg-length discrepancies (LLD) were recorded in both groups. The operative group showed three LLD in total, two Catterall 3 and one Catterall 4 patients, with a mean LLD of 1.0 (range, 1.0–1.5) cm. The conservative group showed five LLD, three Catterall 3 and two Catterall 4 patients, with a mean LLD of 0.5 (range, 0.5–1.5) cm. Maximum recorded LLD was 1.5 cm, present in one hip in both treatment groups. Finally, the career choices ranged widely from student, heavy-duty welder, electro technician, and mechanic to corporate executive and manager. Career choice was not recorded in one patient.
Discussion
In the present study, femoral VDO did not show better results as compared to our conservative containment treatment (prolonged traction in abduction) for the studied Catterall 3 and 4 patients with a median age-at-onset around 4.8 years.
Before discussing the results of the present study some remarks should be put forward. The difficulties in reviewing and comparing the literature in LCPD are extensively specified in literature. These include large differences in—or lack of—information on classification methods, inclusion criteria, age groups, treatment selection, evaluation criteria, incomplete data and other factors [9, 13, 45, 46]. Furthermore, few reports describe the true natural history of the disease [9, 41, 47] and even fewer prospective studies [13, 34, 48] are available. This makes drawing conclusions difficult, if not impossible, and any statements that follow should be read with these remarks in mind.
The conservative containment regime evaluated in the present study has been described in literature to some extent, with varying results [16–18, 49]. These regimes used bed rest or immobilization on a frame with or without abduction, casts, or various periods of traction. Eventually, these conservative regimes were abandoned due to the questioned long-term efficacy, disuse muscle atrophy, osteopenia, high hospital costs, and supposed negative social and psychological effects [17, 19–23]. Most other literature describing bed rest and traction in abduction treatment used it as part of a treatment regime including other treatments, e.g., a short period of abduction in traction to overcome hip irritability and regain range of motion followed by another type of (non)operative containment method [15, 47, 50–56].
The Stulberg classification showed no statistical difference between the conservative and operative groups in the present study. No Stulberg V and only one Stulberg IV hip were recorded, i.e., a conservatively treated bilaterally affected male patient with an age-at-onset of 9.5 years. Besides this apparently favourable outcome for both study groups, only one sign of osteoarthritis was found and functional scores were very good, as well. The fact that median age-at-onset was less than 5 years can certainly play a role in this favorable outcome for both groups. Younger patients have more time for remodeling of the femoral head in the acetabulum and thus a better chance to develop a spherical congruent hip. Numerous authors have previously reported on the importance of age-at-onset [13–15, 34, 45].
No analogous study could be found comparing bed rest and prolonged traction in abduction treatment with femoral VDO. An objective comparison is therefore not possible. Several reports do compare conservative containment treatment to femoral osteotomy, even though all report on other conservative containment regimens (e.g., abduction plasters, abduction orthosis or weight relieving calipers). Furthermore, most studies include less severely affected patients (i.e., Catterall 1 and 2), use other operative methods as well and/or use divers classification and outcome parameters [13, 14, 17, 20, 33–39]. Some of these studies report better results for conservative regime [17] or femoral osteotomy [37, 38]. Others could not find any differences in treatment [20, 33, 35, 36, 39, 48] or suggest decision making based on disease severity and/or age-at-onset [12, 14, 34, 57]. Herring et al. [13] could not find any apparent treatment effect (no treatment, orthosis, range-of-motion exercises, femoral osteotomy, and innominate osteotomy) on outcome in patients with an age-at-onset of 8 years or less, regardless of the severity. More recently, Wiig et al. [34] reported no differences in treatment outcome (physiotherapy, orthosis or femoral osteotomy) in patients less than 6 years at time of diagnosis. The results from the present study are analogous to these recent studies [13, 34], with no differences in outcome between the containment treatment types. In contrast, other studies illustrated the not always favorable prognosis in LCPD patients with onset before five to 6 years of age [57–59].
Follow-up period remains short in the present study, particularly for the operative group, as these patients are probably too young to show radiological degenerative changes. Still, the older conservative patients (median age at follow-up of 32.1 years) revealed similar radiographic and functional scores. Lecuire [60] reported analogous results in a study including 51 hips at much longer follow-up (mean 50.2 years) following conservative treatment. This treatment comprised hospitalization and bed rest, with or without traction, for an average period of 21 (range, 3–45) months. Excellent to very good results were recorded in 24 of the 26 patients with normal or flattened spherical heads, the other two patients had a total hip arthroplasty. Weinstein [61] reported active and pain-free patients with generally good function in 70–90% at 20–40 year follow-up despite the fact that few patients had normal-appearing radiographs. Stulberg [41] showed that after 30 years osteoarthritis developed in 0% in the first three Stulberg classes and in 40 and 86% in the Stulberg IV and V classes, respectively. Other literature is less optimistic [15, 62]. Ippolito et al. [15] performed a 25-year follow-up study evaluating short periods of traction in bed followed by plaster immobilization with weight-relieving caliper for an average of 23 months. In the 36 Catterall 3 and 4 patients included, a Stulberg II or I was found in 30.6%, Stulberg III in 47.2%, and Stulberg IV in 8.3%. Osteoarthritis signs were recorded in 37% of Catterall 3 and 70% of Catterall 4 patients aged between 30 and 40 years old. Yrjönen [47] performed a meta-analysis reviewing the long-term prognosis of LCPD with and without treatment. Even though radiologic results appear to worsen significantly when LCPD patients reach their 40s, the prognosis of untreated patients remains unknown and difficult to predict. In follow-up studies beyond 40 years, reporting patients aged 50–60 years old and older, degenerative disease usually develops in the majority of patients [47]. No convincing reports are available on the long-term outcome of operative treatment on osteoarthritis [47].
Patients’ career choices ranged widely from heavy-duty welder, electro technician, and mechanic to corporate executive and manager. Several authors have put forward psychosocial issues arising from prolonged conservative methods including weight-relief and/or containment methods (brace wearing or traction) [17, 19–23]. Hinzmann and Dahmen [22] concluded that immediate surgical treatment showed psychosocial advantages over conservative treatment. As part of his dissertation, Maathuis [63] evaluated the same patients subjected to the conservative regime of the present study, specifically focusing on the psychological impact on the families of these patients. Surprisingly, the clinical admission period was considered a burden, particularly to the parents. In general this could not be observed in the children. However, nowadays, this conservative regimen cannot be justified due to high hospitalisation and rehabilitation care costs.
Several marginal notes should be put forward. Apart from its retrospective character, as in most LCPD studies, the small size of the study groups is obvious. Limited incidence of LCPD and substantial amount of patients lost to follow-up (36%) are contributing factors. The latter is a problem related to the difficulties in keeping track of these young patients as also mentioned by other long-term studies [13]. Comparison of results between both study groups is complicated by differences in follow-up period, the operative group having a 12.1-year shorter follow-up resulting in a difference in median patient age of 15.8 years. Furthermore, the patients are probably too young to show signs of degenerative disease, the operative group in particular. This will affect radiological and clinical results regarding degenerative changes. Surprisingly good scores were measured for range-of-motion, HHS [43], and modified scoring system of Merle d'Aubigné and Postel [44]. This is probably due to the very few Stulberg classes IV and V, which is more optimistic than other literature. As both scores were evaluated only once by one examiner at follow-up, determination of the intra or inter-rater agreement is not possible. However, both scores have been proven to be reliable evaluation parameters [64].
In conclusion, given the methodological issues, this retrospective study comparing Catterall 3 and 4 patients with a median age-at-onset around 4.8 years showed no apparent differences in outcome at a median follow-up of 14 years for femoral VDO and 28.6 years for prolonged traction in abduction treatment. Apparently, a rigorous prolonged period of traction in abduction can show comparable results to operative treatment. This result is in line with recent literature suggesting a conservative approach in the most severely affected patients with a young age-at-onset. Nevertheless, discussion remains as to which treatment method gives the best long-term outcome. In our opinion, based on unacceptable socioeconomic issues, the specific conservative regime as evaluated in the present study cannot be justified, nowadays.
Footnotes
Acknowledgments
We would like to thank E. de Visser PhD, orthopaedic pediatric surgeon, for his helpful comments during the writing phase of the article.