
Abstract
Abstract
Purpose
Perthes disease may result in deformity of the proximal femoral epiphysis and incongruity of the hip, and shelf acetabuloplasty has been frequently used for treatment. The aim of this study was to review the published articles about the outcome of shelf acetabuloplasty as a containment or reconstruction–salvage procedure in Perthes disease.
Methods
We utilized the PubMed online database for peer review articles using the following search terms: shelf arthroplasty, acetabuloplasty, and Perthes. To be included in this meta-analysis, we isolated studies on children with Perthes disease who received shelf acetabuloplasty as a treatment, conducted in any geographic location with the Stulberg classification outcome. Twenty articles were identified for a qualitative systematic review. The fixed effect and random effect meta-analysis were performed as appropriate for the summary pool estimate following the heterogeneity test. The meta-analysis was performed on 11 articles in three categories: all articles, articles for shelf arthroplasty in the early stages of Perthes disease, and in the late stages.
Results
Overall, shelf acetabuloplasty provided 84 % good outcome of Stulberg classes I, II, and III. Shelf acetabuloplasty performed in early stages for containment provided good outcome in 85 %, while only 69 % good outcome was achieved when shelf acetabuloplasty was performed in late stages for reconstruction–salvage.
Conclusion
Shelf acetabuloplasty provides a good or fair Stulberg outcome when performed in early Perthes stages (Waldenström stages I and II) as a containment surgery, but less favorable outcomes were observed when shelf surgery was used for reconstructive–salvage purposes in late Perthes disease stages (Waldenström stages III and IV). Caution is advised in performing the shelf procedure in children over 10–11 years of age.
Introduction
Legg–Calvé–Perthes disease is a condition of unknown etiology in children resulting from necrosis of the capital epiphysis and physis of the proximal femur. This condition affects boys more than girls (4:1 ratio), with mean onset of 6 years of age, ranging from 2 years to maturity [1, 2]. The disease course is prolonged, involving four stages described by Waldenström [3]. During the initial stage, which usually lasts for 6 months, there is necrosis in the capital epiphysis. Subsequently, in the next stage, fragmentation begins as neovascularization, which removes the necrotic bone that appears radiographically as lucencies. This second stage lasts an additional 6 months, during which trabecular collapse, subchondral fracture, and femoral head lateralization may occur. New bone formation initiates the third stage (reossification) and may last for more than 3 years. In the final stage (residual), a growth disturbance in the proximal femoral physis may cause shortening of the femoral neck, relative overgrowth of the greater trochanter, and limb length discrepancy [4, 5]. A deformity of the femoral head predisposes the hip to arthritis in adulthood, and prognosis can be graded using the Stulberg classification, which is based on the femoral head shape and congruency of the joint [6]. Stulberg type I is a normal femoral head, whereas type II is a spherical femoral head with associated short femoral neck or “steep acetabulum.” Type III is an elliptical femoral head, and type IV is a flattened femoral head. If the acetabulum is incongruent with the femoral head, the hip is graded as type V.
The goals of treatment in Perthes disease are to prevent the deformity of the femoral head or to restore congruency of a deformed femoral head. From the necrosis stage until reossification of the lateral femoral head, common containment methods include abduction/internal rotation casting or bracing [7], femoral varus osteotomy [8], or pelvic osteotomies (Salter, shelf) [9]. If the hip is deformed after reossification, a reconstruction–salvage procedure may be utilized to delay the onset of hip arthritis in adulthood, which may consist of either femoral valgus osteotomy [1], shelf acetabuloplasty [10], Chiari osteotomy [11], femoral head cheilectomy [12], or the removal of loose osteochondral fragments [13].
Shelf acetabuloplasty has been used for containment in the necrosis and fragmentation stages of Perthes disease [14–21], and also as a reconstruction–salvage procedure in the reossification and remodeling stages [10, 22]. The aim of this current study was to examine published articles referenced in PubMed about Perthes disease treated with a shelf acetabuloplasty, with the purpose of assessing the effectiveness as determined by Stulberg outcome of shelf acetabuloplasty performed for containment during early stages (necrosis and fragmentation) or for reconstruction–salvage performed during the reossification and residual stages. A qualitative systematic review and meta-analysis were performed. We hypothesized that the shelf acetabuloplasty procedure in Perthes disease is effective in obtaining a good or fair Stulberg outcome when performed as a containment operation in the early stages, and has a less favorable outcome when used as a reconstructive–salvage operation in the later stages.
Materials and methods
Search technique
The studies for this systematic review were identified using the following search terms: Perthes, shelf operation, shelf acetabuloplasty, Perthes and shelf operation, Perthes and shelf acetabuloplasty, and Perthes and shelf augmentation. The main data source was PubMed, and included studies researched between 1966 and early 2012 (Fig. 1).
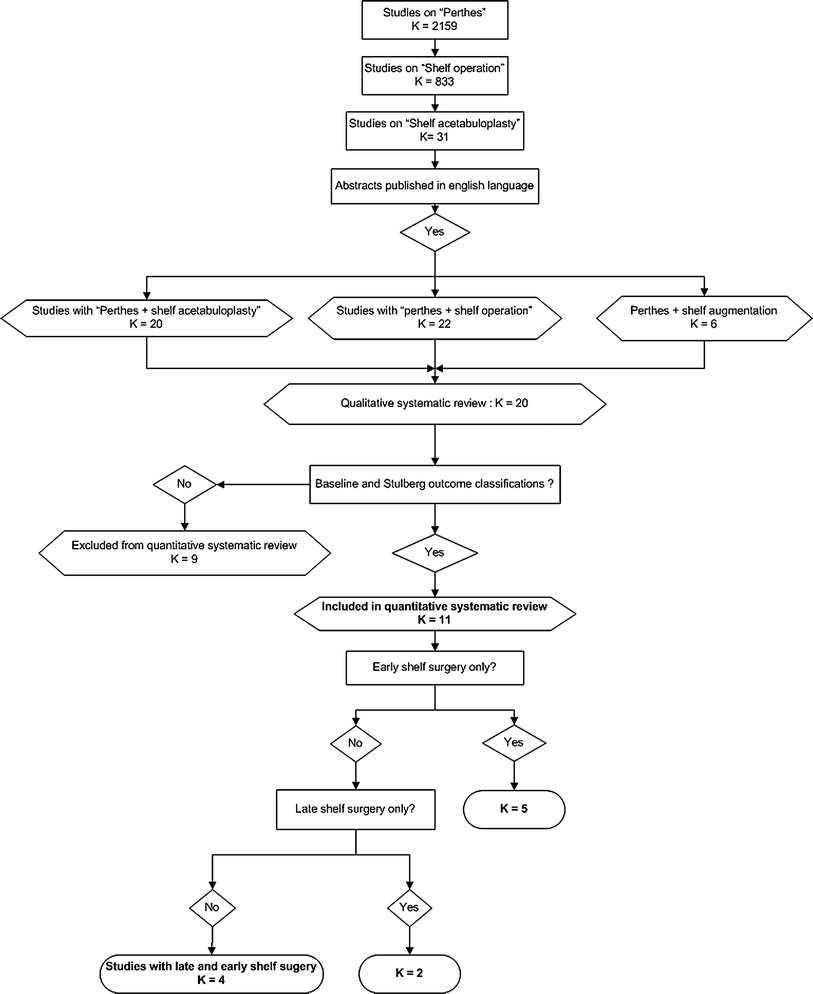
Study schema illustrating studies selected for the systematic review
Eligibility criteria
Studies that met the following criteria were eligible for inclusion in this systematic review: (a) studies on children with Perthes disease who received shelf acetabuloplasty as a treatment; (b) studies conducted in any geographic location; (c) studies with abstracts published in English; (d) studies with a sample size equal to or greater than 10 patients; (e) studies with available baseline Perthes staging and classification; and (f) studies with available Stulberg outcome classification.
As an exclusion criterion, we excluded from our quantitative systematic review (meta-analysis) any study conducted in the same institution using the same patient sample. In this case, we utilized the latest publication for inclusion.
Study quality assessment
The studies included in this systematic review were assessed for: (a) outcome measure; (b) patient selection to determine whether consecutive patients were selected; (c) sample size to assess whether studies estimated the sample size and had enough power to examine the outcome of surgery; (d) confounding factors to assess whether the studies presented factual results; (e) bias to assess studies for selection, information, and misclassification biases; (f) study objectivity to assess the studies to determine whether the aims or the purposes of the papers were clearly stated; (g) design to include only retrospectively conducted studies; and (h) adequate statistical analysis to assess how the outcome measures were determined by examining the statistical tests used.
Study variables
Study sources indicating the authors, the year of publication, and the geographic location were examined. In addition, study populations were stratified by gender and the number of hips with Perthes disease by side. The patient characteristics examined included age at diagnosis, age at surgery, delay time before surgery, and follow up time. Radiographic characteristics included Waldenström staging of Perthes disease, Catterall classification, and Stulberg classification. We also considered the technique of shelf acetabuloplasty including abductor muscle stripping from the ilium [23, 24] versus the minimally invasive/iliac splitting technique [14, 25], as well as the utilization of autologous bone graft or allograft.
Sample size and power estimation
Twenty articles published between 1991 and 2011 (17 retrospective cohort studies [15–22, 26–34] and three retrospective comparative studies [10, 14, 35]) were identified for the qualitative systematic review.
The number of studies included in the quantitative systematic review aspect of this paper is represented by K = 11. The combination of study sizes (sample size) that constitute this meta-analysis (quantitative systematic review) is represented by n = 275. We used 95 % confidence interval (CI; 5 % error), effect size of 20 % (0.2), and a random effect meta-analytic technique (DerSimonian and Laird). With these parameters, and with the combined sample sizes from the individual studies (n), we obtained a sufficient power to detect a difference between good versus poor outcomes in terms of the Stulberg outcome classification.
Statistical analysis
Both descriptive and inferential statistics were performed. The descriptive statistics used were the mean, standard deviation (SD), median, range, and interquartile range for the continuous variables. Frequency and percentages were also used to summarize the categorical data into proportion, assessing the good and poor outcomes. To test the specific hypothesis as the expected outcome determined by the Stulberg classification is better when shelf acetabuloplasty is performed in early stages compared with late stages, we used both the fixed effect method of Peto and Mantel–Haenszel, as well as the random effect meta-analytic technique. The fixed effect method was applicable to the summary point estimate when the studies that constituted the meta-analysis were assessed to be homogenous. This implies that, unless the homogeneity test is performed, the fixed method is inapplicable. The random effect method of DerSimonian and Laird was effective when the homogeneity assumption was not met, implying that this method adjusted for variability between the studies that constituted the meta-analysis.
The significance level for homogeneity was 0.02, but it was 0.05 for summary or pool estimate of the effect of shelf acetabuloplasty on Perthes disease. All tests were two-tailed and all analyses were performed using STATA 12.0 (StataCorp LP, College Station, TX, USA).
Results
Twenty articles were identified for the qualitative systematic review and they are presented in Table 1. There were two studies performed at the same institution utilizing the same time frame and inclusion criteria for their patient sample selection [15, 19]; therefore, the most recent article was included in the quantitative systematic review [15]. Five studies were also performed in the same institution [10, 14, 17, 28, 29]; two articles were included in the systematic review [10, 14], and the remaining studies were excluded due to the possibility of utilizing the same patient sample. Two other papers were also published from the same institution [20, 21], and they utilized patients from the same time frame. The latest article was excluded [21] because it had an ambidirectional design with a smaller sample size. There were an additional two studies performed in the same institution during the same time frame [32, 33], and the latest one was excluded [33] because it did not characterize the baseline stages and classification of the patient sample. Three other articles were excluded because the patients were not identified in terms of outcome of treatment using the Stulberg classification [26, 27, 34]. One of these papers examined two groups of patients [31]; one group was treated with shelf acetabuloplasty only and the other group was treated with shelf acetabuloplasty with femoral varus osteotomy. Therefore, we included the patients who received shelf acetabuloplasty only in the quantitative systematic review.
Characteristics of studies included in the systematic review
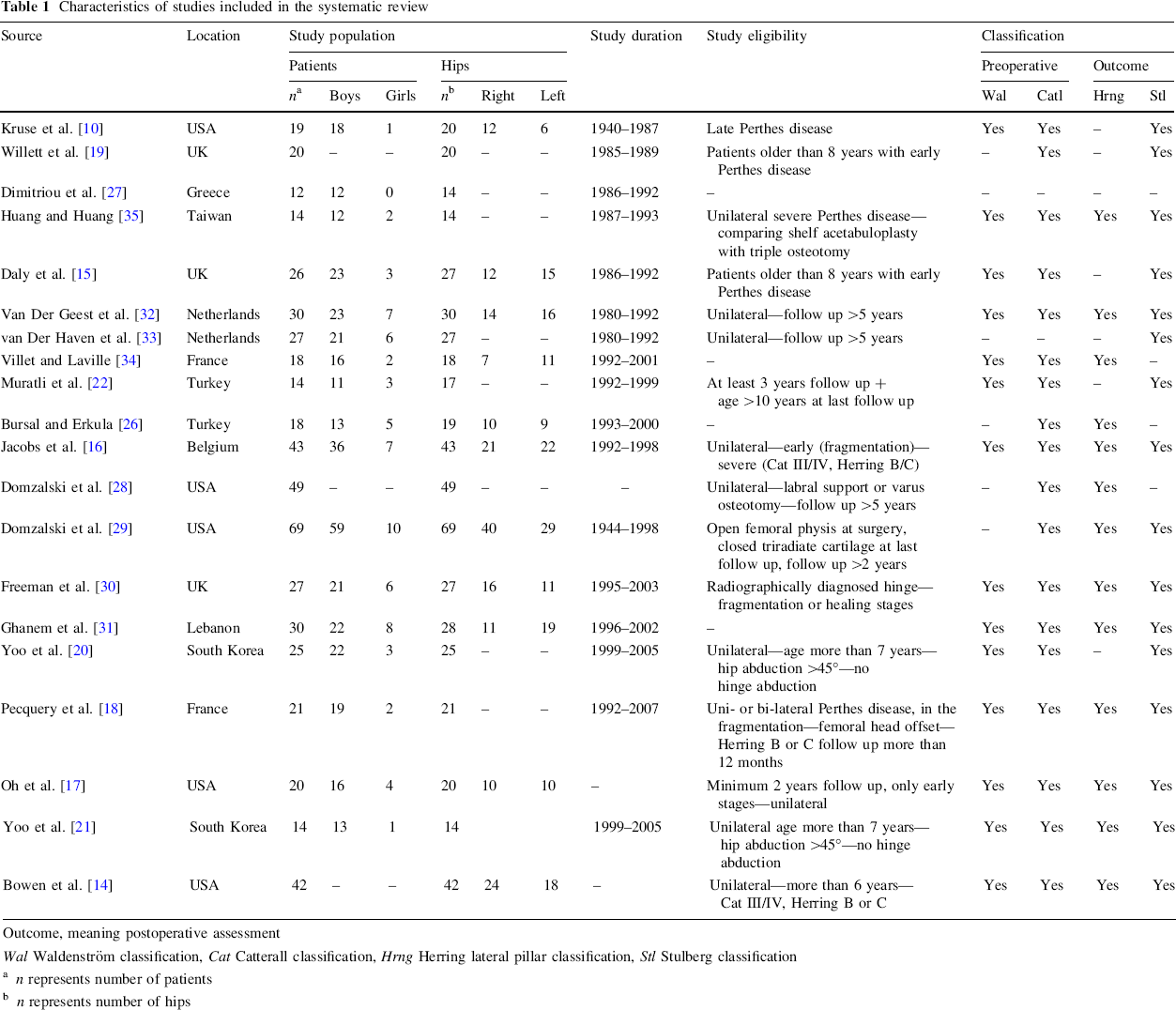
Outcome, meaning postoperative assessment
Wal Waldenström classification, Cat Catterall classification, Hrng Herring lateral pillar classification, Stl Stulberg classification
n represents number of patients
n represents number of hips
After these exclusions, 11 articles remained for systematic review [10, 14–16, 18, 20, 22, 30–32, 35] (Table 2). These 11 studies generated 275 patients with 280 hips. The mean age at diagnosis was 7.5 years, SD = 1.0 years, range from 6.4 to 9.8 (two studies did not provide information on the age at diagnosis of Perthes disease [20, 35]). The mean age at surgery was 8.9 years, SD = 1.1 years, range from 7.3 to 11 (one study did not provide data on age at surgery [32]). The mean follow up was 7.2 years, ranging from 3 to 19 years (two studies did not provide follow up for their patients [15, 31]).
Study demographics and classification systems
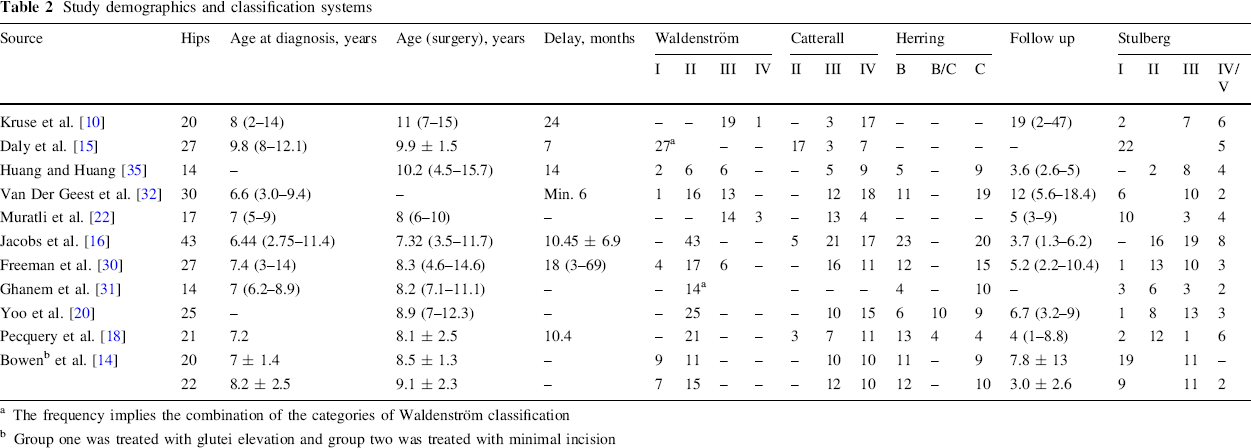
The frequency implies the combination of the categories of Waldenström classification
Group one was treated with glutei elevation and group two was treated with minimal incision
Based on the Waldenström classification, 204 hips were in the early stages, while 62 hips were in the late stages (one study did not provide precise Waldenström classification [31]). Based on the Catterall classification, 25 hips were in class II, 112 hips were in class III, and 129 hips were in class IV (one article did not provide Catterall classification [31]).
Type of surgery
Most of the articles in this quantitative systematic review described the outcome of shelf acetabuloplasty using the conventional technique involving elevation of the glutei muscles from the outer surface of the ilium [10, 15, 16, 18, 22, 30–32, 35]. Yoo et al. [20] performed shelf acetabuloplasty with the avoidance of abductor muscle stripping from the ilium. Bowen et al. [14] compared the results of the labral support procedure, which was performed through a minimal incision with the utilization of arthroscopy and allograft, with the conventional shelf technique with glutei elevation from the ilium.
Patients with poor outcome
Some of the studies included in this meta-analysis described patients with poor outcomes. Daly et al. [15] reported five patients who had poor outcomes after shelf acetabuloplasty with a mean age at surgery of 11.7 years. Bowen et al. [14] described two patients who were older than 11 years at the time of surgery and developed poor outcome after shelf acetabuloplasty. Pecquery et al. [18] reported six patients with poor outcome (Stulberg IV/V), two of whom were less than 6 years of age at surgery, and three were older than 10 years. Jacobs et al. [16] also reported eight patients with Stulberg IV hips whose mean age at surgery was 9.1 years. Freeman et al. [30] reported two patients with Stulberg IV hips (ages at surgery were 8.5 and 10 years, respectively) and one patient with Stulberg V hip who had surgery at age 14 years. Muratli et al. [22] reported two patients with Stulberg IV (ages at surgery were 8 and 9 years, respectively) and two patients with Stulberg V hips (ages at surgery were 9 and 10 years, respectively).
Quantitative systematic review
Table 3 illustrates the percentages, 95 % CI, and the contribution of individual studies (weight) of good outcomes (Stulberg I/II/III) in the studies that constituted this meta-analysis. The combination of all studies in the meta-analysis clearly indicated a statistically significant improvement of hips in the patients with Perthes disease after shelf surgery. The summary or pool estimate after the heterogeneity test was 84.2, 95 % CI (78.4–89.9), p < 0.05. Four studies contributed significantly to the meta-analysis [14, 16, 20, 30], as they demonstrated substantial good outcomes (Fig. 2). These studies were slightly heterogeneous and the pool estimate reported here is the random effect meta-analysis, I2 = 43.4 %, p = 0.06.
The point estimate by percentage and pool estimate of individual studies
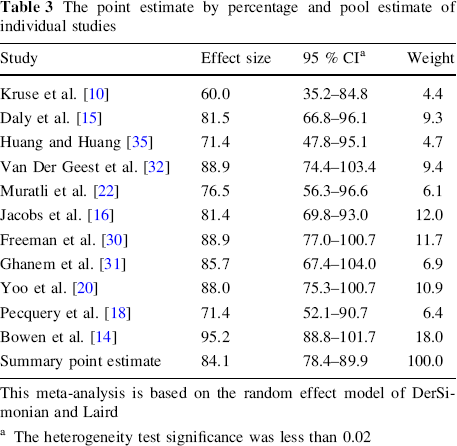
This meta-analysis is based on the random effect model of DerSimonian and Laird
The heterogeneity test significance was less than 0.02
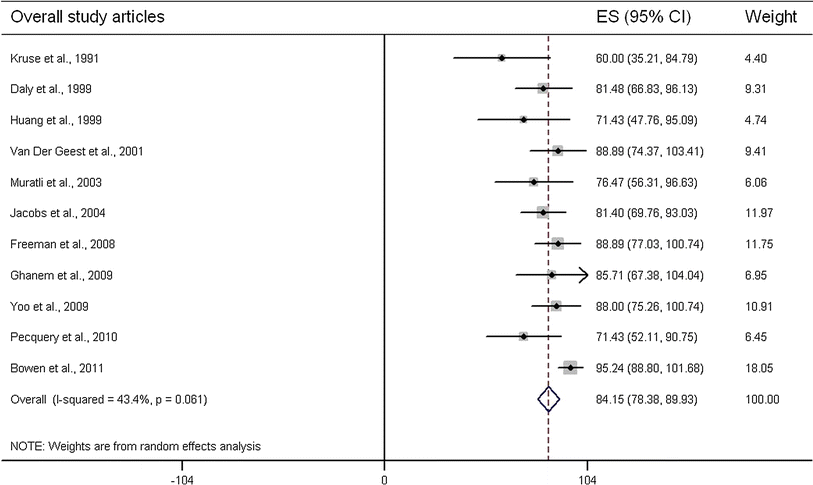
Forest plot illustrating the effect sizes (ES) and 95 % confidence interval (CI); pool estimate of the overall studies is illustrated by the diamond. Heterogeneity is measured by I2. The statistical significance is less than 0.02
Table 4 presents the percentage, 95 % CI for percentage, and the weights of the studies that examined the outcome of shelf acetabuloplasty in the early stages of Perthes disease. There were 158 hips, the mean age at diagnosis was 7.8 years, SD = 1.4, range from 6.4 to 9.8 years, and the age at surgery was 8.6 years, SD = 0.9, range from 7.3 to 9.9 years. The overall summary point estimate showed a good outcome following surgery, 85.6, 95 % CI (77.4–93.9), p < 0.05 (vs. 14.4 % poor outcome). The heterogeneity test indicated variability in the studies that constituted this subgroup meta-analysis, I2 = 57.7 %, p = 0.05. Therefore, random effect meta-analysis was also used in this subgroup meta-analysis (Fig. 3).
The point estimate in percent of individual studies (shelf acetabuloplasty during early Perthes disease) and pool estimate
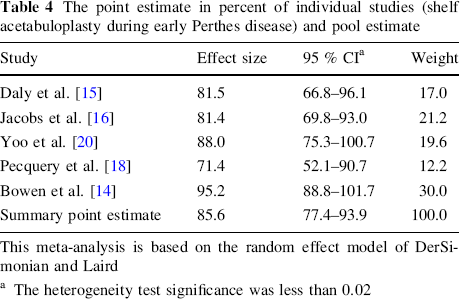
This meta-analysis is based on the random effect model of DerSimonian and Laird
The heterogeneity test significance was less than 0.02
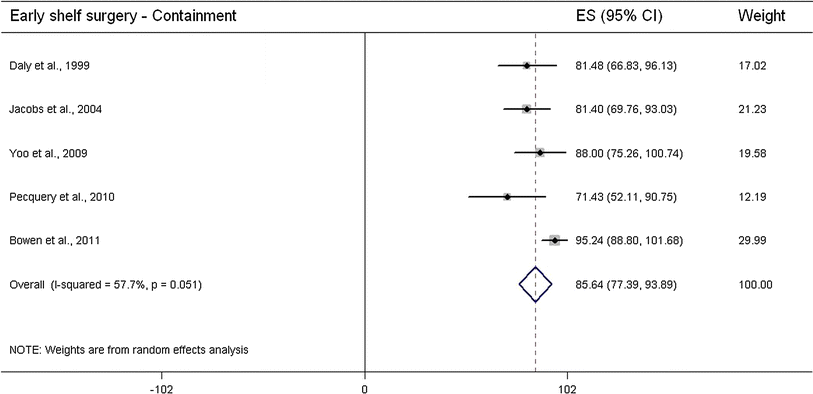
Forest plot illustrating the effect sizes (ES) and 95 % confidence interval (CI); pool estimate for the studies on shelf acetabuloplasty during early stages is illustrated by the diamond. Heterogeneity is measured by I2. The statistical significance is less than 0.02
Table 5 presents the percentages, 95 % CI for percentage, and the weights of the studies that examined the outcome of shelf acetabuloplasty in the late stages of Perthes disease. There were 37 hips, the mean age at diagnosis was 7.5 years, SD = 0.7, range from 7 to 8 years, and the age at surgery was 9.5 years, SD = 2.1, range from 8 to 11 years. The overall summary point estimate showed a good outcome following surgery of 69.9, 95 % CI (55.3–85.5), p < 0.05 (vs. 31.1 % poor outcome). The heterogeneity test indicated no variability, implying homogeneity of the studies, I2 = 2.0 %, p = 0.31. Therefore, we used the fixed effect meta-analysis of Peto and Mantel–Haenszel in this subgroup meta-analysis (Fig. 4). Finally, Fig. 5 presents the Forest plot visualizing the overall data alongside early and late shelf procedure data.
The point estimate in percent of individual studies (shelf acetabuloplasty during late Perthes disease) and pool estimate

This meta-analysis is based on the fixed effect model of Peto and Mantel–Haenszel
The heterogeneity test significance was less than 0.02
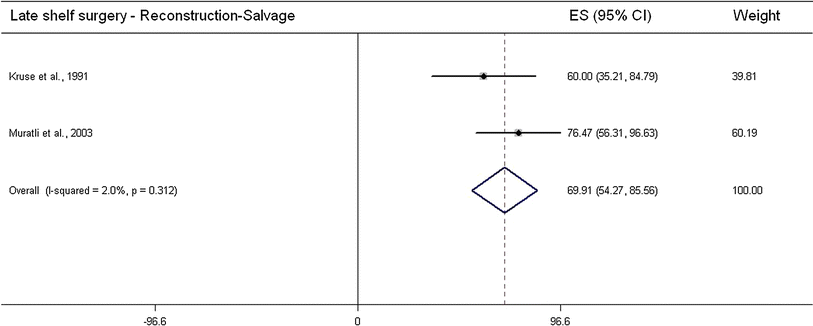
Forest plot illustrating the effect sizes (ES) and 95 % confidence interval (CI); pool estimate for the studies on shelf acetabuloplasty during late stages is illustrated by the diamond. Heterogeneity is measured by I2. The statistical significance is less than 0.02
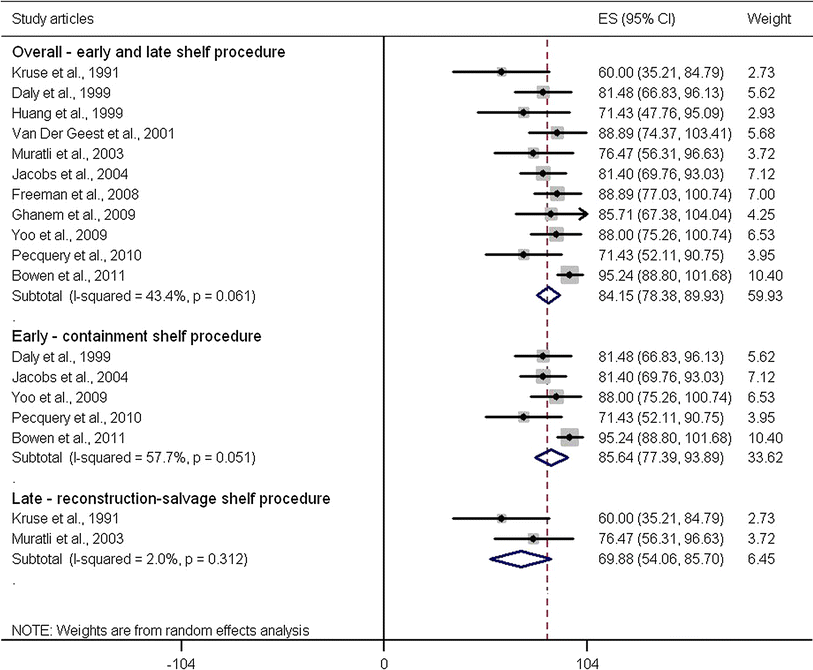
Forest plot illustrating the effect sizes (ES) and 95 % confidence interval (CI); pool estimate for overall, early shelf acetabuloplasty, and late shelf acetabuloplasty studies are illustrated by the diamonds. Heterogeneity is measured by I2. The statistical significance is less than 0.02
Discussion
Perthes disease involves necrosis of the proximal femoral epiphysis and physis. Containment of the necrotic epiphysis within the acetabulum is a common treatment in the early phases of the disease, including: abduction casting, femoral osteotomy, pelvic osteotomy, or shelf acetabuloplasty. After the femoral epiphysis reossifies, some hips have an aspherical and incongruent femoral epiphysis, and several reconstructive–salvage treatments have been reported, including shelf acetabuloplasty, femoral osteotomy, cheilectomy, femoral head reduction, and pelvic osteotomy. Since the shelf acetabuloplasty is used as both a containment procedure and a reconstructive–salvage procedure, we were not clear about the reported outcomes of its usage. The aim of this meta-analysis was to examine published articles referenced in PubMed about Perthes disease treated with shelf acetabuloplasty, with the intent to assess its effectiveness as measured by the Stulberg classification when performed during the early stages of necrosis or fragmentation (i.e., containment procedure) or during reossification or residual stages (i.e., a reconstructive–salvage procedure).
Predictors of outcome of the treatment of Perthes disease include age at onset, extent of epiphyseal necrosis, degree of epiphyseal or hip deformity, and stage of disease at treatment (i.e., containment vs. reconstruction–salvage). Children with Perthes disease who are older than 9 years of age have been shown to have poor outcome compared with younger children [36–38]. Children under 6 years of age tend to have good results; however, some hips in young patients may develop severe femoral head deformity [39]. Fabry et al. [40], in their systematic review, observed that patients younger than 6 years of age may have poor outcome. Pecquery et al. [18] found two patients with poor outcome who had shelf acetabuloplasty at less than 6 years of age. Schoenecker et al. [41] indicated that children younger than 6 years of age may have poor outcome when more than 50 % of the femoral head is involved. In our systematic review, age at the onset of disease was not reported adequately enough to allow a quantitative systematic review. However, poor outcomes (Stulberg IV and V) were reported more commonly in cases in which the shelf acetabuloplasty was performed at an age older than about 10–11 years.
The extent of femoral head involvement in Perthes disease has been shown to be a significant predictor of outcome [42, 43]. Catterall [43] described four groups of Perthes disease based on the epiphyseal sequestrum and collapse. Favorable outcomes were expected when less than 50 % of the femoral head was affected by the disease [41–43]; total epiphyseal necrosis has the worst prognosis. In our meta-analysis, most cases treated with shelf acetabuloplasty were classified as Catterall III or IV and had substantial necrosis prior to treatment. The degree of epiphyseal or acetabular deformity has been measured by multiple processes including several radiographic indices, including lateral femoral head translation [15, 16, 18], acetabular coverage [14–16, 30–32], and acetabular angle (Sharp angle) [15, 16, 20, 31]. We selected the Stulberg classification as the outcome variable.
A qualitative systematic review on the effect of shelf acetabuloplasty in improving hip coverage and decreasing hip symptoms was recently published [44]. Our meta-analysis revealed that the shelf acetabuloplasty procedure used as containment (performed during Waldenström stages of necrosis or fragmentation) provided a significant, 85 % good Stulberg outcome (classes I, II, or III). However, the shelf acetabuloplasty procedures used as reconstruction–salvage (performed during Waldenström stages of reossification or residual) offered a significant, 69 % good Stulberg outcome (classes I, II, or III). In this meta-analysis, we examined heterogeneity and considered the studies to be homogeneous at a significance level of 2 % (type 1 error tolerance). The random effect meta-analysis is conducted if significant heterogeneity is observed among studies that constitute the meta-analysis. With this approach, it is unlikely that variability between studies will affect our findings. The heterogeneity of studies is one of the most important considerations in meta-analysis. The overall meta-analysis was affected by heterogeneity, which resulted in the use of the random effect meta-analysis of DerSimonian and Laird. The subgroup meta-analysis observing the outcome of shelf acetabuloplasty in early stages of Perthes disease also was affected by heterogeneity, and we utilized random effect meta-analysis in this subgroup as well. Our subgroup meta-analysis that observed outcomes in later stages showed significant homogeneity, and we reported our pool estimate with the fixed effect meta-analysis of Peto and Mantel–Haenszel. The fixed effect meta-analysis is used when there is marginalized variability between studies.
There are a few limitations in this meta-analysis. We used a pool estimate in drawing the inference regarding the outcome of Perthes disease following shelf acetabuloplasty. Like every meta-analysis, heterogeneity remains a limitation of our study. Secondly, because we included only retrospective studies in this meta-analysis, it is possible that our findings may be affected by selection and misclassification biases of the original articles. For example, several studies used the Stulberg classification differently, which has a tendency of introducing selection bias into the original studies and, subsequently, into our meta-analysis. General consensus remains in the application of the Stulberg classification. In terms of reliability, the Stulberg classification has been examined and the level of experience may affect the detection of flattening of the femoral head (i.e., class III vs. class II) [45]. However, this classification model is widely used and conveys some level of reliability of substantial nature. There is a tendency to classify Stulberg I/II as good outcome, III as fair, and IV and V as poor outcomes. In contrast, I/II/III have also been classified as good, while IV and V have been classified as poor outcome. In our meta-analysis, we applied a classification model that considers I to III as good and IV and V as poor. This classification was applied to all studies equally without any form of misclassification bias. Because the reliability of meta-analysis is contingent on the internal and external validities of the studies selected for the meta-analysis, possibly the lack of confounding adjustment and bias minimization may influence the findings in this meta-analysis. Therefore, to overcome this bias, we used the random effect meta-analysis.
In addition, our meta-analysis is limited because substantial parameters used to assess the outcome of Perthes disease were not available in some of the studies, rendering the pool estimate impossible to compute. Outcomes were appropriate when assessed with a similar instrument used for the baseline.
Conclusion
In summary, shelf acetabuloplasty is effective in obtaining a good or fair Stulberg outcome of 85 % when performed in the early stages of Perthes disease (Waldenström stages I and II) and has a less favorable outcome of 69 % when used as a reconstructive–salvage operation when performed in the late stages of Perthes disease (Waldenström stages III and IV). These findings suggest that shelf acetabuloplasty is favorable in early Perthes disease and is a reasonable containment approach to manage Perthes disease, although caution is advised with its use as a reconstruction–salvage procedure.
Footnotes
None.