
Abstract
Background:
Typical sequelae of Perthes disease and Perthes-like deformities comprise a short femoral neck, aspherical femoral head, and greater trochanteric overgrowth. Morscher’s osteotomy aims at restoring the normal extra-articular anatomy, but incapable of restoring a normal head-neck contour with residual impingement. Femoral neck lengthening osteotomy combined with osteochondroplasty through surgical hip dislocation approach was not previously described in the literature. We hypothesized that this technique is capable of near-normal restoration of the proximal femoral anatomy, increasing limb length, restoring abductor power, and simultaneous management of intra-articular chondro-labral disease.
Methods:
A prospective series of 21 consecutive patients with sequelae of Perthes disease and Perthes-like deformity (Stulberg II and III) were treated by Morscher’s osteotomy through surgical hip dislocation approach. The mean age was 14.9 years (9–30 years) and the mean follow-up was 4.5 years (2–8 years).
Results:
The mean Harris hip score improved significantly from 66.5 to 89.5 points (p < 0.001), and the mean limb length discrepancy improved from 2.5 to 0.6 cm (p < 0.001). The mean alpha angle improved from 81.8° to 49.5°, the mean neck-shaft angle increased from 117.8° to 129.8°, and the articulo-trochanteric distance has improved from −6.7 to 20.8 mm. Six out of 21 patients required staged periacetabular osteotomy for residual acetabular dysplasia. No cases of chondrolysis or osteonecrosis were identified.
Conclusion:
Femoral neck lengthening osteotomy through surgical hip dislocation appraoch has proven to be safe and effective for preservation of symptomatic hips with Perthes and Perthes-like deformities and mild to moderate femoral head deformities (Stulberg II and III). A staged periacetabular osteotomy may be required in those patients with significant acetabular dysplasia.
Level of evidence:
Level IV.
Keywords
Introduction
Sequelae of Perthes disease and other childhood hip disorders are common and result from premature closure of the femoral neck physis, with unbalanced overgrowth of the greater trochanteric (GT) apophysis. 1 The term “Perthes-like” deformity2–5 has been designated by many authors to describe the common morphologic features, typical of Perthes disease and other hip conditions, including multiple epiphyseal dysplasia (MED), osteonecrosis secondary to infection, trauma, and treatment of developmental dysplasia of the hip (DDH).
The typical proximal femoral deformity comprises a large aspherical femoral head (FH), short femoral neck with GT overgrowth (coxa brevis).5,6 These structural changes negatively impact the hip biomechanics and frequently result in femoro-acetabular impingement (FAI), various intra-articular lesions, hip pain, reduced range of motion (ROM), and eventual osteoarthritis (OA). 7
The shortened femoral neck manifests clinically by limb length discrepancy (LLD) ranging from 1.5 to 3.0 cm.1,8 A decreased abductor lever arm results in abductor insufficiency which presents by abductor fatigue and Trendelenburg gait. The trochanteric overgrowth decreases the resting abductor muscle tension, further reducing the abductor power. In addition, a high overriding GT may abut against the lateral wall of the ilium, decreasing abduction. 9 Coxa brevis may also result in ischio-femoral impingement as the excessively medialized lesser trochanter impinges on the ischium, resulting in pain, snapping, decreased internal rotation, and/or decreased hip adduction. 10 In addition to the extra-articular deformity, intra-articular lesions are very common. Symptomatic hips with residual Perthes-like deformities commonly have cam and/or pincer impingement, chondral lesions, labral tears, osteochondral lesions, ligamentum teres (LT) ruptures, and loose bodies.5,10,11
Surgical treatment of these deformities is challenging and depends on the pathological features unique of each case. 12 The general goals of surgery are to relieve FAI, maintain hip stability, correct associated intra-articular lesions (labrum, articular cartilage, LT), and delay the onset of OA. Treatment options may include proximal femoral osteotomies (PFO),11,13 femoral osteochondroplasty,2,12 relative femoral neck lengthening (RFNL),3,12,14 trochanteric advancement,9,15 femoral head reduction osteotomy (FHRO),3,10 periacetabular osteotomy (PAO),2,12,16 and management of associated intra-articular abnormalities (labral, articular cartilage, and osteochondral lesions). 5 To date, no gold standard has been established for treatment of these characteristic deformities.
True femoral neck lengthening osteotomy with distalization of the GT was first described by Morscher in 1988. 17 The technique permits elongation of the neck length, correcting the LLD, and distal transfer of the overriding GT. A number of clinical studies17–19 evaluated this procedure and have shown a good clinical outcome. However, femoral neck lengthening alone is incapable of complete restoration of the anatomy of the proximal femur, particularly the head-neck junction, and management of intra-articular chondro-labral disease in presence of symptomatic FAI.
With improved understanding of the blood supply to the FH, and the ability to safely dislocate the hip, 20 surgical hip dislocation (SHD) approach has been recently utilized in treatment for symptomatic residual deformities in adolescent hips.2,12,13,18,21,22 It permits assessment and treatment of intra-articular FAI and related chondro-labral pathology, reshaping the head-neck contour through osteochondroplasty, as well as biomechanical restoration of the hip with various extra-articular procedures.11,23
However, the outcomes of surgical dislocation approach combined simultaneously with true femoral neck lengthening osteotomy are not well established. To the best of our knowledge, this is the first article describing this procedure at the time of design of this study. This study evaluates the efficacy and safety of femoral neck lengthening osteotomy performed through SHD approach in symptomatic hips with sequelae of Perthes and Perthes-like deformities. The presented technique is thought to provide a single procedure that can simultaneously address FAI with associated intra-articular lesions, correcting LLD, improving hip congruency, in addition to transfer of the GT to improve abductor power and gait.
Patients and methods
This prospective case series from a single institution included 21 consecutive patients (21 hips), conducted during the period from July 2014 to January 2018. The study included 11 males and 10 females. The mean age was 14.9 years (9–30 years). The right side was affected in 11 patients, and the left side in 10 patients. The preoperative diagnosis included osteonecrosis after femoral neck fracture (7), DDH complicated by osteonecrosis (5), Perthes disease (4), MED (3), and sequelae of septic hip arthritis (2). Fifteen patients had previous surgeries, including ilio-femoral distraction by Ilizarov fixator in one patient with Perthes disease, open reduction and femoral osteotomy in all five patients with DDH, and drainage of septic arthritis of the hip in two patients. All seven patients with post-traumatic osteonecrosis had previous pinning by cannulated screws for femoral neck fractures. The mean follow-up was 4.5 years (2–8 years). No patients were lost in the follow-up. Institutional review board approval was obtained prior to the start of the study. All patients have received a prior non-operative treatment for at least 6 months, including analgesics, physical therapy, and activity modifications, with persistent symptoms.
Surgery was indicated for children, adolescents, and young adults with symptomatic healed Perthes and Perthes-like deformities, with the typical morphologic features (coxa brevis, coxa magna, and high-riding GT) and symptomatic LLD. Hips with chondrolysis, marked incongruency from flattened FH (Stulberg classes IV and V), 24 osteonecrosis with collapsed FH, or advanced hip OA (Grade 2 or more according to Tönnis and Heinecke) 25 were excluded from our study.
Clinical evaluation
The preoperative clinical assessment focused on history, clinical examination, and Harris hip score (HHS) 26 was used as a functional score. The range of clinical features included groin pain, lateral hip pain (secondary to impingement and/or abductor fatigue), limited ROM, limp, and interference with daily activities. Examination focused on gait (antalgic/short limb/Trendelenburg gait), presence of positive Trendelenburg sign, and abductor muscle strength (M0–M5) 27 as compared to the contralateral normal side. Anterior and posterior impingement tests 28 were conducted to detect underlying cam, pincer, or labral pathology. Full goniometric hip ROM was assessed; the maximum motion without initiating pelvic rotation was measured. Hip internal/external rotation was recorded with the patient in the prone position. Amount of LLD was determined by computed full-length standing radiographs. Lower limb rotational profile was assessed according to Staheli et al. 29
Radiographic evaluation
Standard anteroposterior (AP) and frog-lateral radiographs of the pelvis and both hip joints were obtained and assessed for the following radiographic parameters: shape and congruency of the FH, 30 femoral neck-shaft angle (NSA), and medial proximal femoral angle (MPFA), 31 and both angles were compared to determine the presence of coxa vara, coxa brevis, or both. Articulo-trochanteric distance (ATD) 1 was used to quantify the relationship of the FH to the GT; negative values were assigned for measurements above the top of the FH. The lateral center-edge angle 30 (LCEA) and the alpha angle 32 were obtained as indices for hip dysplasia and FAI, respectively. Computed tomography was performed to assess the three-dimensional bone morphology, accurately determine FH dysmorphism and acetabular version, and for cam and pincer impingement.
Surgical technique
All cases were performed under general anesthesia and the preoperative dose of antibiotic was administered. The patient was positioned in the lateral position and the ipsilateral leg was draped free. In all cases, surgical dislocation approach was done as described by Ganz et al. 23 The duration of surgery (determined from the time of skin incision to the end of wound closure), blood loss, need for transfusion, and length of hospital stay were assessed. The technique was divided into four parts.
Trochanteric flip osteotomy
A 15-cm straight lateral skin incision, centered over the GT, was carried down through the subcutaneous fat and through the fascia lata using sharp dissection. The posterior border of the gluteus medius is identified, and a GT flip osteotomy was performed using an oscillating saw and completed with a straight osteotome. The osteotomy extended from just anterior to the posterior border of gluteus medius to the start of the intertrochanteric line anteriorly, with a maximal thickness of 1.5 cm. The gluteus medius and vastus lateralis are reflected anteriorly with the trochanteric fragment. The posterior interval between the gluteus minimus and piriformis was identified, and the gluteus minimus was reflected off the hip joint capsule up to the level of the supraacetabular ilium. The gluteus minimus insertion was transected off the trochanteric fragment and marked with stay sutures to facilitate subsequent mobilization of the GT.
The hip was then brought into external rotation; two Hohmann retractors were placed on the anterosuperior and anterior aspects of the acetabular rim to facilitate exposure of the entire anterosuperior, anterior, and posterosuperior hip capsule. A Z-shaped capsulotomy was then performed using a knife and sutures are placed in the flap corners. The longitudinal limb was carried along the neck axis ending medially at the perilabral recess, exposing but not injuring the labrum. The second limb extended posteriorly parallel to the labrum, stopping at the piriformis tendon. The third limb extended anteroinferiorly ending just anterior to the lesser trochanter. After transecting the LT, the FH was easily dislocated. Anterior hip sublaxation without transecting the LT was sufficient to expose the pathologic portions of the labrum and head-neck junction in a few patients.
Assessment and management of intra-articular disease
Once dislocated, the FH and acetabulum were examined for chondro-labral lesions. Intraoperative findings were documented, and the presence of labral tears and articular cartilage lesions was recorded (Table 1). Cam lesions were managed by osteochondroplasty using a 1-cm curved osteotome and high-speed burr to trim the aspherical portion of the FH, recontouring the head-neck offset (Figure 1). Care was taken to limit the extent of resection to less than one-third of the femoral neck width to avoid the risk of femoral neck fracture. Unstable labral tears or chondral flaps were debrided. Labral repair or refixation to the acetabular rim was performed using either mattress transosseous sutures or PushLock® 2.4-mm knotless anchors (Arthrex, Inc., FL, USA). Full-thickness chondral lesions were managed by microfracture 33 using an arthroscopic microfracture awl (Figure 2).
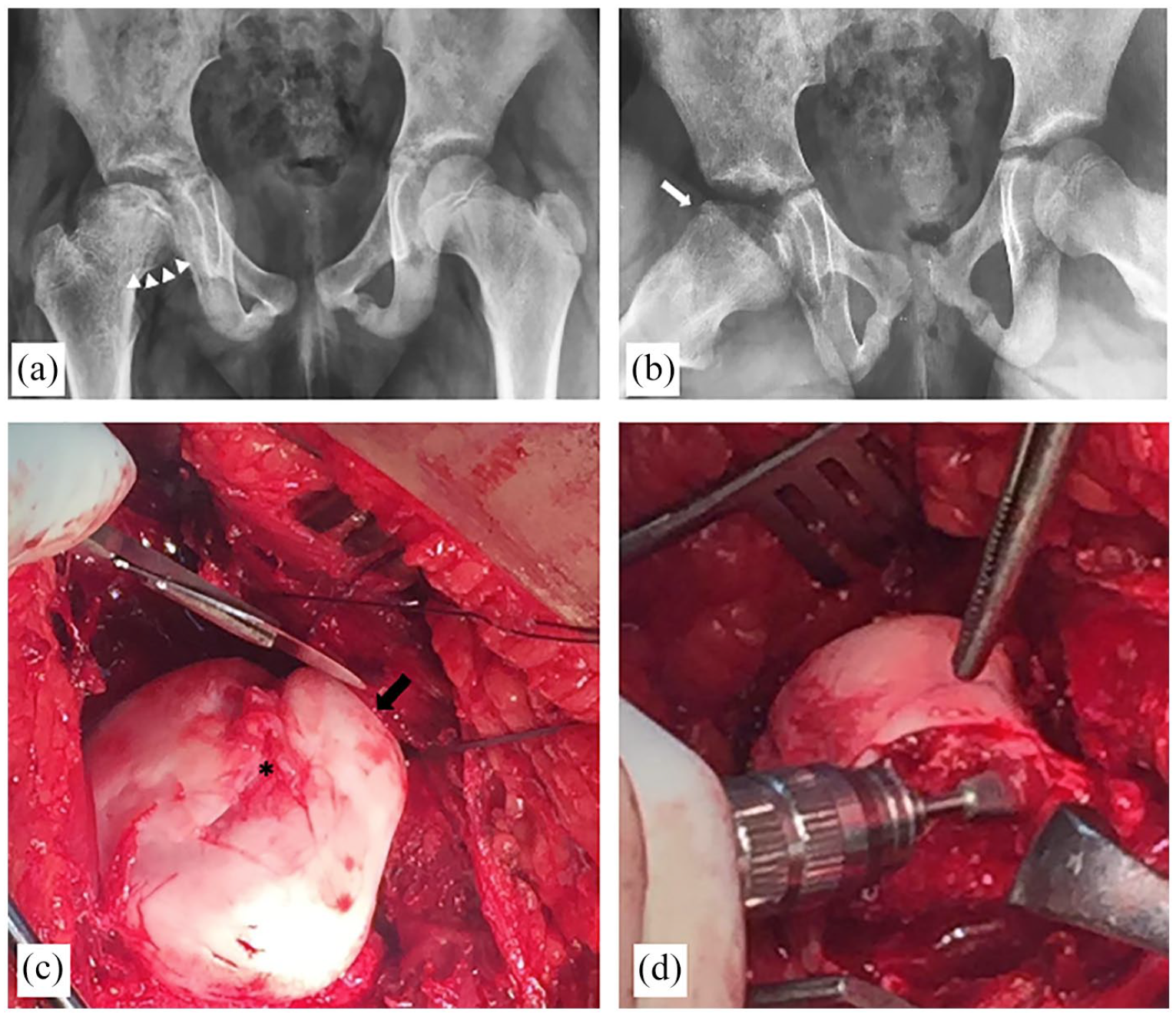
A 9-year-old girl with sequelae of Perthes disease. (a) AP pelvic radiograph; the right hip shows flattening of the FH with sagging rope sign denoting an anterior cam lesion (white arrow heads). (b) Frog-lateral radiograph; reduced anterior head-neck offset (white arrow). (c) Intraoperative photograph; extruded anterolateral head, anterior focal cam lesion, separated from the posteromedial head by a central necrotic segment devoid of articular cartilage with exposed subchondral bone (asterisk). (d) Restoring head-neck contour during osteochondroplasty.
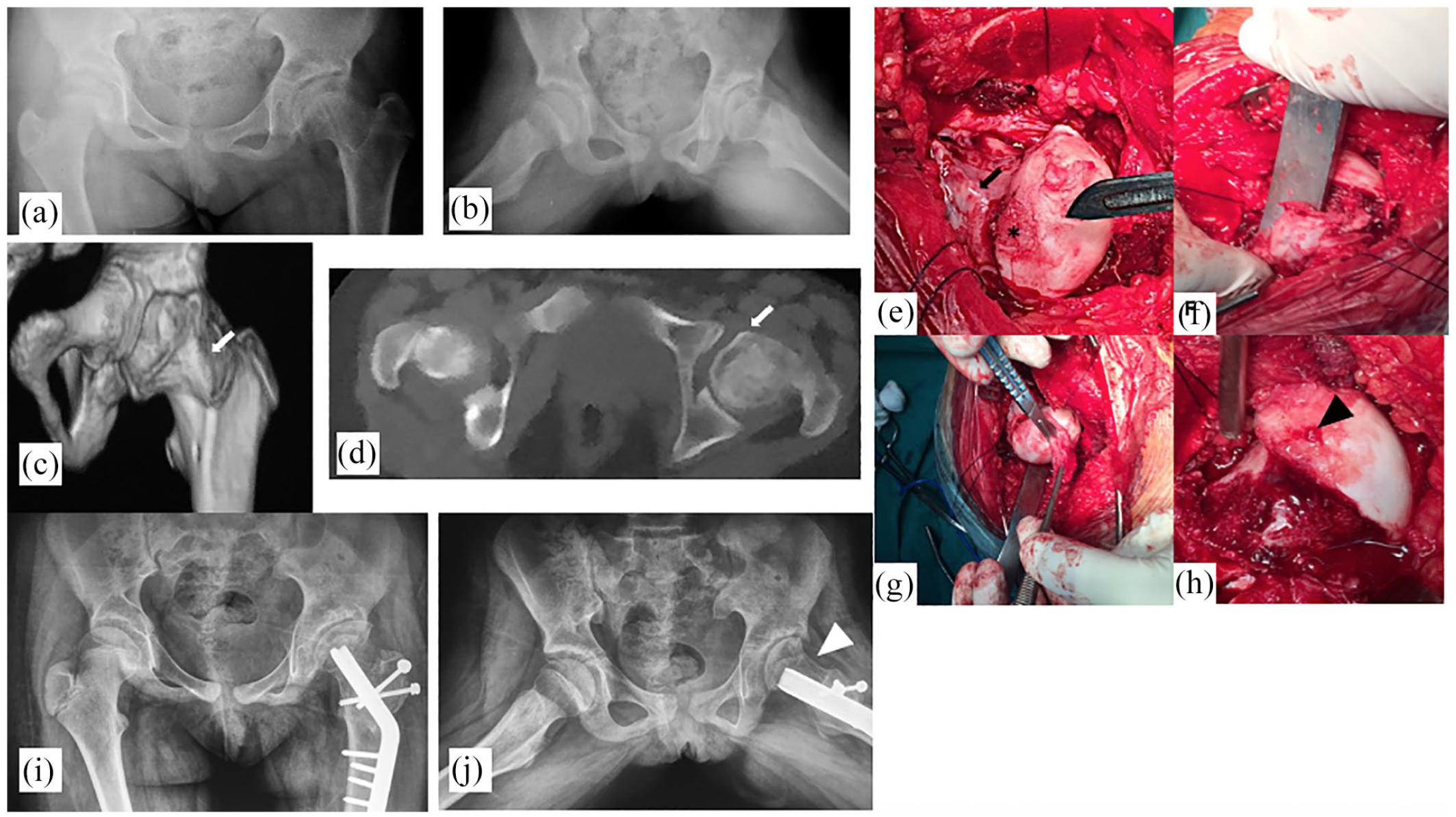
A 10-year-old girl with osteonecrosis secondary to DDH treatment. (a and b) Preoperative radiographs. The left hip shows signs of dysplasia with steep roof arc angle, and the femoral head is enlarged (coxa magna) and aspheric. (c and d) Preoperative CT scan; enlarged FH, a large cam lesion at the anterior head-neck junction (white arrow). (e) The intra-articular procedure. Examination revealed a large full-thickness chondral ulcer (asterisk), global FH chondromalacia, chondral flaps, and a large cam lesion (black arrow). (f) Osteochondroplasty recontouring head-neck junction. (g) Debridement of the hypertrophied ligamentum teres. (h) Microfracture of chondral ulcer (black arrow head). (i and j) Postoperative radiographs. Elongated femoral neck, distalized GT, and head-neck offset restored (white arrow head).
Summary of the intra-articular procedures.
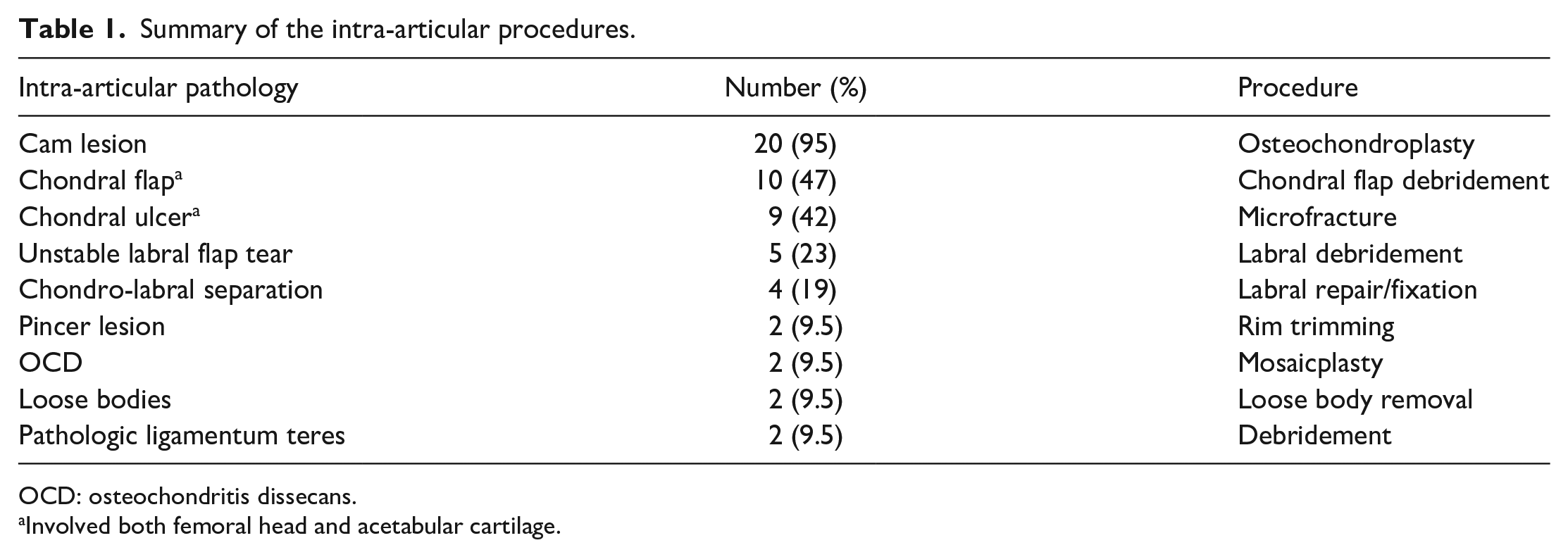
OCD: osteochondritis dissecans.
Involved both femoral head and acetabular cartilage.
Two hips with unstable, loose osteochondritis dissecans (OCD) lesions of the FH were diagnosed on the preoperative radiographs and confirmed intraoperatively. These were debrided and burred to bleeding bone and managed by osteoarticular autografting from the ipsilateral knee using the OATS® system (Arthrex, Inc.) (Figure 3). Trimming of the acetabular rim was performed in two hips with focal pincer lesions. The labrum was sharply transected off the rim in a bucket-handle fashion, followed by rim trimming back to normal articular cartilage with labral refixation. Functional fluoroscopic views were then repeated intraoperatively to determine head congruency, after head-neck recontouring.
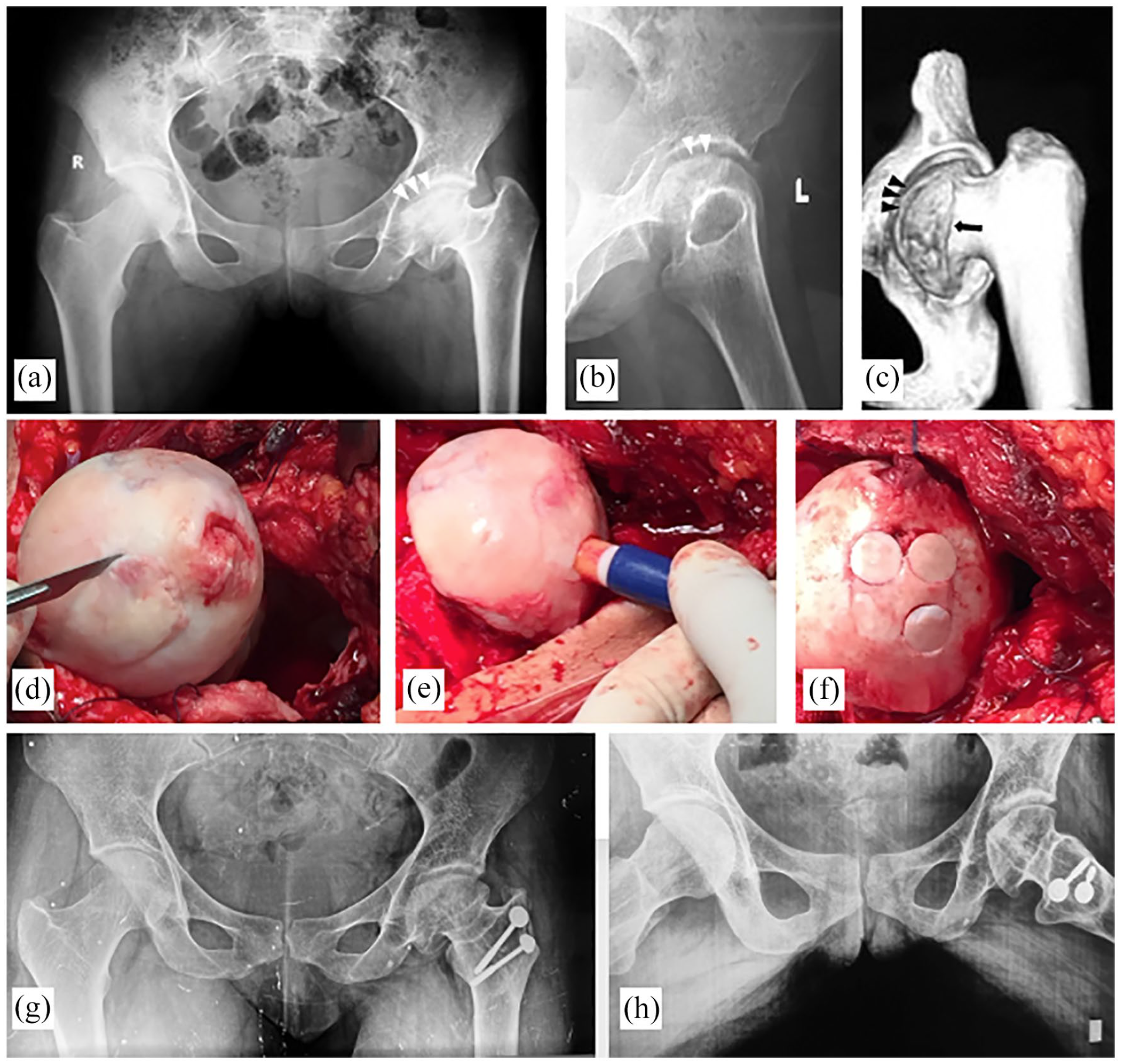
A 20-year-old female with post-traumatic osteonecrosis of the femoral head, presenting with progressive groin pain, locking of the hip during motion, shortening and limp. Preoperative radiographs. (a) The left FH is flattened in the superomedial part, a loose fragment (white arrow heads) can be seen, suggesting an OCD lesion. The femoral neck is shortened (coxa brevis), reduced NSA, and high-riding GT. (b) Lateral radiograph; flattened FH, anterior cam, and congruent joint. (c) Three-dimensional reconstruction CT scan showing an anterior cam lesion (arrow) and the separated intra-articular fragment (arrow heads). (d–f) Intraoperative photographs. A large OCD lesion (asterisk), managed by OATS® from the ipsilateral knee. Ruptured ligamentum teres, femoral head diffuse chondromalacia, labral fraying, synovitis, and a loose body were also recorded. (g, h) Eight-year follow-up radiographs. A more congruent joint compared to preoperative films, improved head sphericity, well-preserved cartilage space, and no progression of the OA grade. The femoral neck has been lengthened, more vertically aligned, and the GT has been distalized.
Intertrochanteric neck lengthening
The hip was then reduced and the next steps of neck lengthening were similar to the technique described by Hefti and Morscher. 17 A guide wire was inserted in the center of FH and neck, at an angle of 130° to match the angle of the blade plate and to create a normal NSA. This also avoids unwanted rotation of the head position within the acetabulum maintaining congruency. A second guide wire was inserted, parallel to the first, at the level of the superior neck. Since a trochanteric flip osteotomy has been performed as part of the approach, osteotomy along the second wire creates a free bone block that will be used later as a graft. A particular advantage of utilizing the SHD approach is identification and protection of the posterosuperior retinaculum and blood supply to the FH during the superior neck osteotomy, avoiding the risk of injury to the retinacular vessels and FH osteonecrosis compared to conventional blind osteotomy techniques through the superior neck. A third parallel guide wire was inserted at the level of the inferior neck to guide the inferior neck osteotomy (Figure 4).
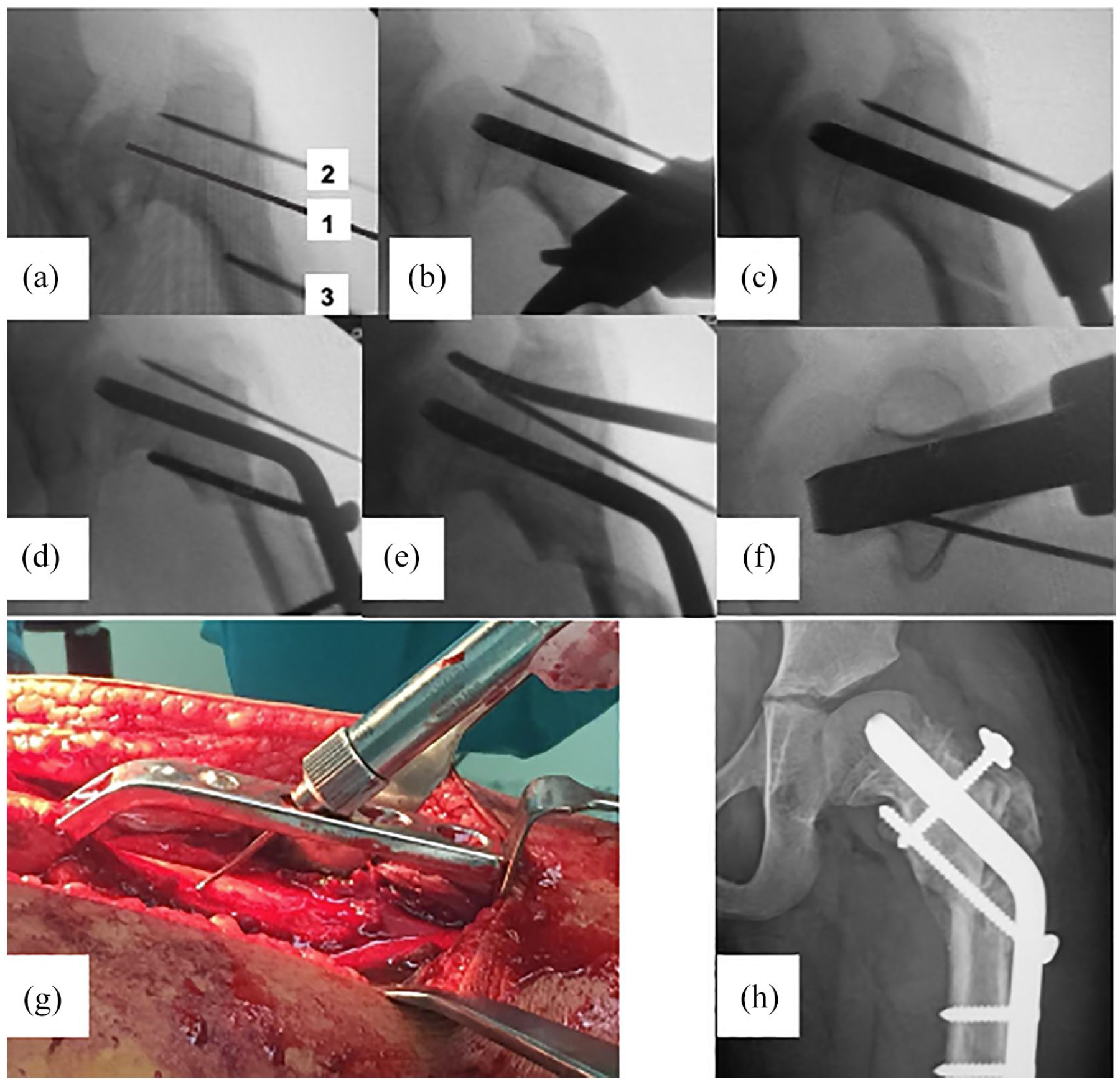
Steps of the neck lengthening osteotomy. (a) The first guide wire (1) inserted in the center of the femoral head and neck, at an angle of 130°. A second guide wire (2) inserted parallel to the first, at the level of the superior neck. A third parallel guide wire (3) inserted at the level of the inferior neck. (b) Seating chisel along the central guide pin. (c) Blade plate is inserted and inferior neck osteotomy is completed. (d) Shaft approximated to the plate creating neck lengthening. (e) Completion of the osteotomy along the superior neck guide pin, creating a free bone block. (f) Position of the blade in the lateral view. (g) For effective neck lengthening, the chosen blade length was greater than the measured length by 2 cm. (h) The final postoperative x-ray demonstrating neck lengthening and GT position.
The seating chisel was placed along the first guide wire. The length of the blade was determined such that the plate projects away from the head-neck fragment by a distance equal to half of the shaft diameter. This was estimated by adding 1.5–2.0 cm to measurement on the seating chisel. The length of the blade or screws left exposed will determine the amount of lateral translation at the inferior neck osteotomy. We relied on a 130° blade plate for fixation, as adopted in a number of studies.17,19 This has been shown to offer sufficient rigidity and effective lateralization of the shaft. Variable fixation methods have been employed, including locking proximal femoral plates 34 with a similar outcome.
The intertrochanteric osteotomy was then performed along the inferior wire by a large oscillating saw. A four-hole 130° angled blade plate was applied, transfixing the bone graft with the blade, and then inserting the blade into the head-neck fragment. The lateral translation lengthens the femoral neck, adding length to the limb, and corrects the mechanical axis of the lower limb. The plate was secured to the shaft with cortical screws.
According to the preoperative assessment, a prior decision was made to perform additional valgus or varus components. For cases with combined coxa brevis and coxa vara, neck lengthening and valgus osteotomies were performed. Changing the inclination of the seating chisel into the head-neck fragment in the AP plane can achieve the desired amounts of varus and valgus components of the osteotomy. If a derotation component is to be added, the amount of derotation is determined on clinical basis to fairly produce an equal range of internal and external rotation after completion of osteotomy (Suppl. Table 1, Figure 5).
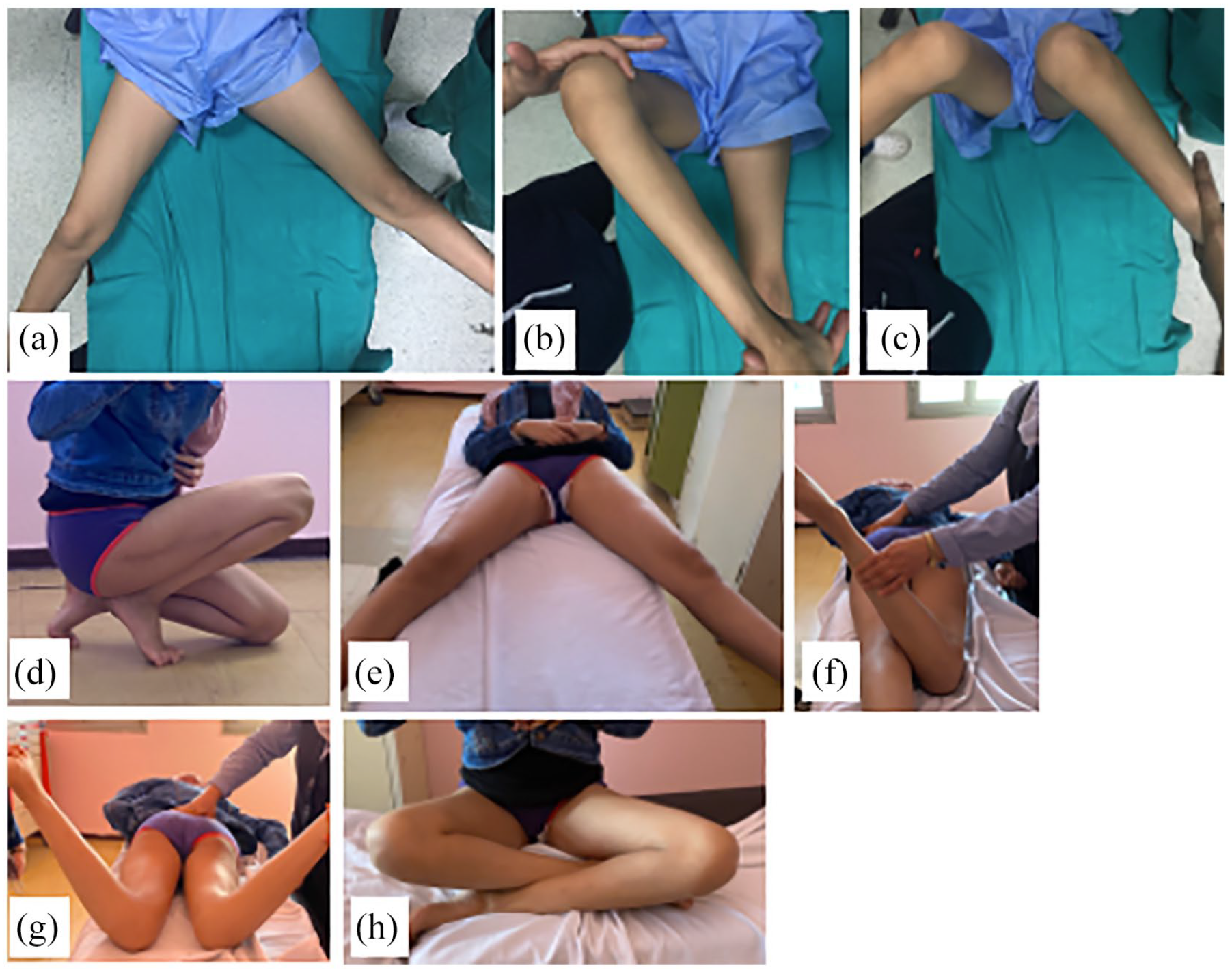
A 12-year-old child with a Perthes-like deformity of the right hip due to femoral head osteonecrosis complicating a femoral neck fracture (radiographs of the same patient are shown in Figure 6). Preoperative photographs showing (a) limited hip abduction, (b) limited hip external rotation in flexion, the child was not able to sit crossing legs, (c) excessive hip internal rotation in flexion compared to the left side. Three-year clinical follow-up, (d) impingement-free hip flexion, (e) symmetrical hip abduction, (f) external rotation in hip extension, (g) symmetrical internal rotation in extension, and (h) symmetrical external rotation in flexion, easy crossing of legs.
Fixation of the trochanteric flip
The capsular flaps were approximated without tension using interrupted absorbable suture, and the gluteus minimus tendon was repaired to the new trochanteric base under moderate tension. The GT fragment was advanced distally until the superior tip of the trochanter was located at the same level as of center of the FH and position confirmed under fluoroscopy. Fixation was done by two 4.5-mm cortical screws with washers. The fascia lata, subcutaneous, and skin were closed in layers (Figures 4 and 6).
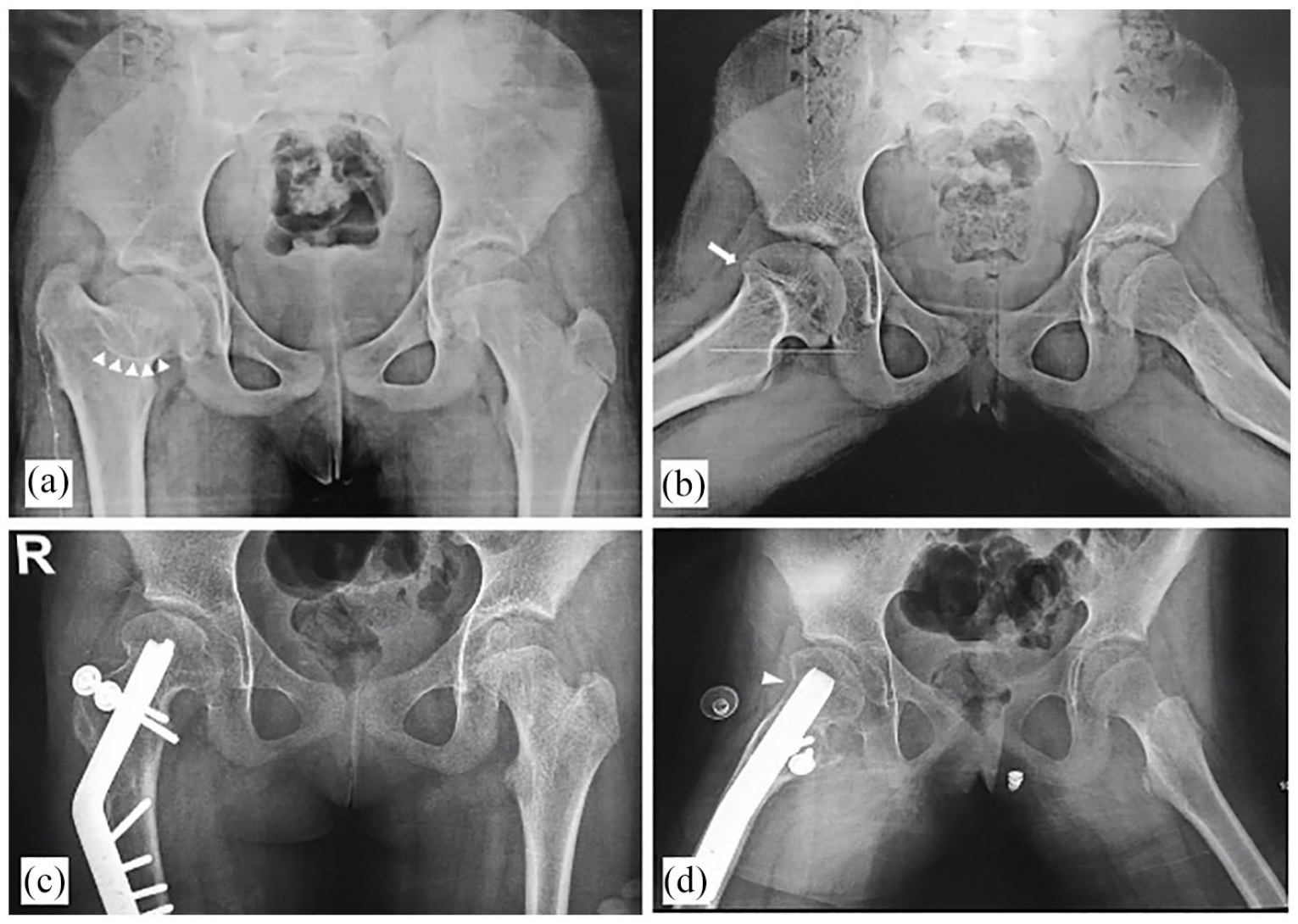
A typical Perthes-like deformity of the right hip complicating a femoral neck fracture at age of 4 years. (a and b) Preoperative radiographs showing short femoral neck length compared to the left side (coxa brevis), overriding GT compared to the level of the femoral head, aspherical femoral head with sagging rope sign (white arrow heads) denoting cam impingement, insufficient offset at the head-neck junction in the frog-lateral view (white arrow). The patient has a positive anterior impingement test. (c and d) Three-year follow-up after femoral neck lengthening, GT distal-lateral transfer, trochanteric reduction, derotation, and osteochondroplasty. The femoral neck length has been effectively increased, correcting the child’s LLD, the GT distalized in relation to the femoral head, a derotation component has been added to the intertrochanteric osteotomy correct excessive femoral anteversion shown in Figure 5. Restored offset at the head-neck junction after osteochondroplasty (white arrow head).
Additional procedures
Adductor tenotomy was performed in three patients. Retraction by the tight adductors may limit valgus correction of the distal fragment, with the risk of an oblique pelvis postoperatively. A Bernese PAO osteotomy was performed to improve congruency in six patients with CEA <15° associated with instability symptoms, but this was scheduled as a second-stage surgery 3–6 months after the index procedure.
Postoperative protocol
Patients were placed on a continuous passive motion during the first 3 days, adjusted to achieve passive hip flexion of 90°, at a rate of two cycles per minute. Partial weight-bearing was instructed during the first month. Stationary bike exercise was introduced at 1 month. Radiographs were repeated monthly to determine union of both trochanteric and intertrochanteric osteotomies. Thereafter, patients started full weight-bearing after union of the trochanteric osteotomy.
All patients were re-evaluated at 6-month intervals till the latest follow-up. This included clinical and functional assessment using the HHS and goniometric ROM measurements. Preoperative and postoperative values were compared for each case. Plain radiographs at the final follow-up included assessment of FH viability, union of trochanteric and intertrochanteric osteotomies, measurements of radiographic indices, and observation of any radiographic OA progression (increase in Tönnis grade). Results were analyzed using the Statistical Package for Social Science (SPSS 20; IBM corp. Armonk, New York, USA). Analytical statistics, the paired t test, and McNemar test were used to assess the statistical significance.
Results
Clinical parameters
The mean HHS improved from 66.5 to 89.5 points (p < 0.001). The mean LLD improved from 2.5 cm (range, 1.5–4.5 cm) to 0.6 cm (range, 0.2–1.5), with a mean improvement of 1.89 cm. The percentages of patients with a positive anterior impingement and Trendelenburg tests have shown significant improvement (Table 2). Fourteen patients have converted from a positive to a negative Trendelenburg test. The mean arcs of motion improved in all the measured directions (Figure 5). The mean abduction has increased from 26.5° ± 10.8 to 42.4° ± 8.86 (p < 0.001). The mean internal rotation range also demonstrated a significant improvement from 19.4° ± 17.59 to 32.4° ± 8.15 (p < 0.001). The mean blood loss was 195 ml (range, 130–350 ml), the mean duration of surgery was 118.5 min (95–170 min), and the mean length of hospital stay was 2.5 days (2–5 days).
Improvements in the clinical parameters and HHS.
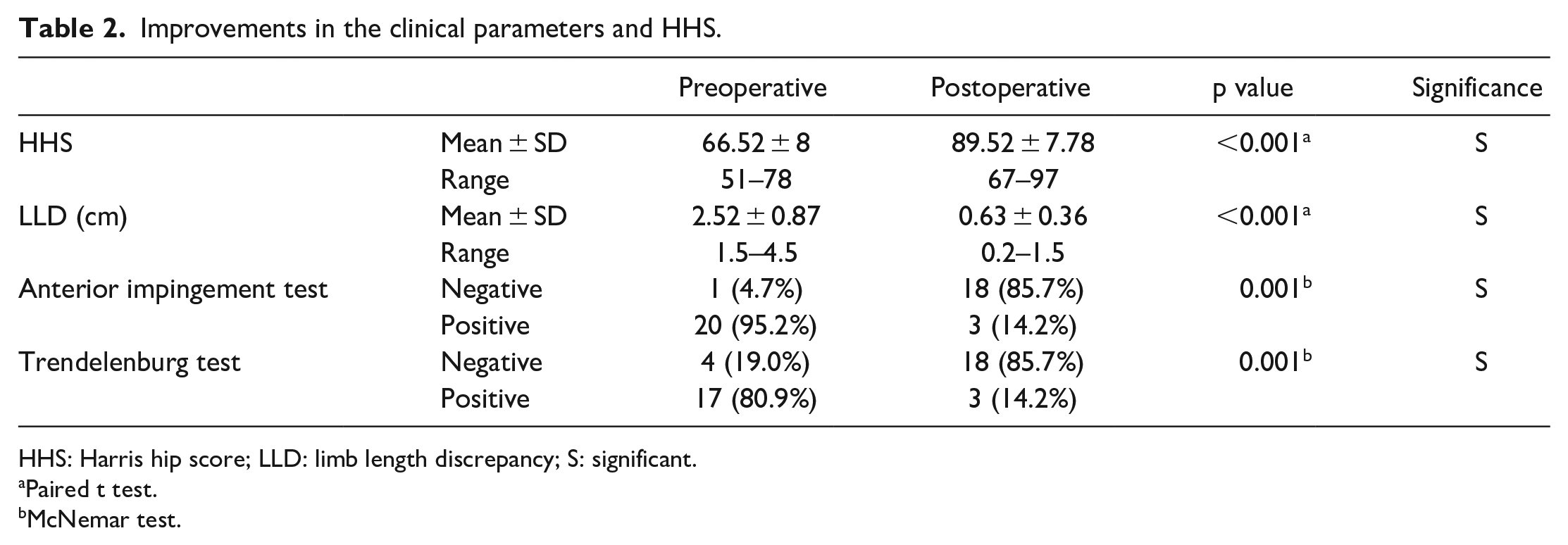
HHS: Harris hip score; LLD: limb length discrepancy; S: significant.
Paired t test.
McNemar test.
Radiographic parameters
All the radiographic indices of hip morphology have shown a significant improvement after the procedure (Table 3, Figure 6). The mean NSA has increased by 12°. The mean alpha angle has decreased from 81.8° to 49.5° (p < 0.001). The procedure effectively distalized the GT from a negative ATD of −6.7 mm to a mean postoperative ATD of 20.8 mm (p < 0.001). A PAO was performed to improve congruency in six patients with an initial CEA < 15°, scheduled as a second-stage surgery 3–6 months after the index procedure. The final mean CEA at the latest follow-up has increased from 16.6° to 26.2°.
Improvements in the radiographic parameters.
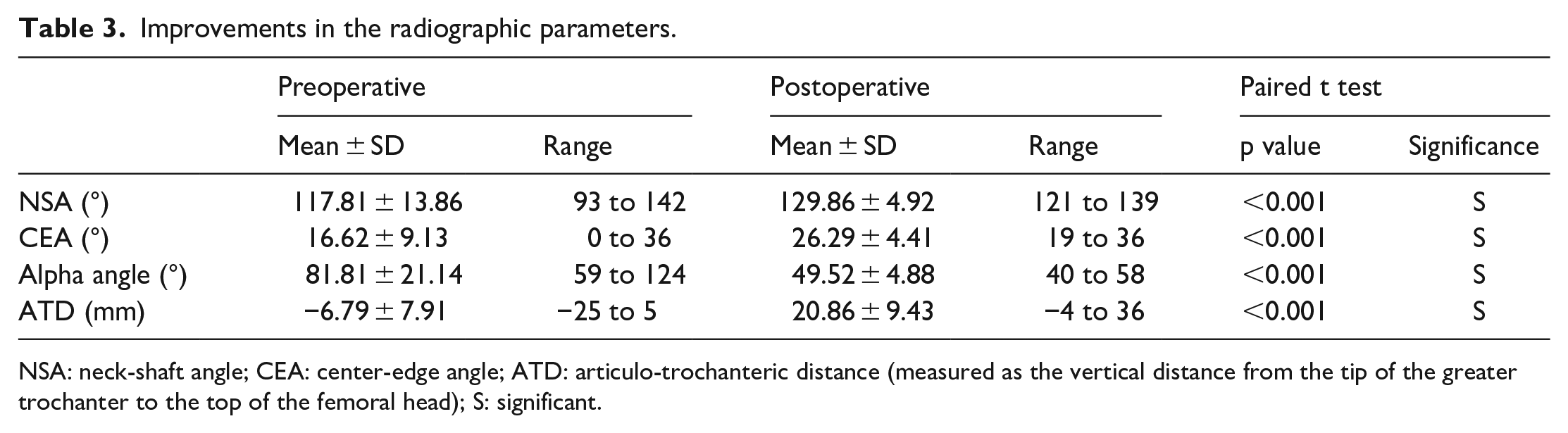
NSA: neck-shaft angle; CEA: center-edge angle; ATD: articulo-trochanteric distance (measured as the vertical distance from the tip of the greater trochanter to the top of the femoral head); S: significant.
Complications
One patient was a 10-year-old boy with MED developed an excessive keloid formation of the surgical scar, without any clinical significance regarding the hip function. He had an HHS of 95 points at 18-month follow-up. Another patient had radiographic progression of OA with an insufficient clinical outcome (HHS of 67 points). He was a 14-year-old boy with sequelae of septic arthritis of the hip, and a preoperative HHS of 62 points. Despite a good initial clinical outcome during the first year after the index procedure, he later developed occasional groin pain with upright activities. The radiographs at 5 years of follow-up showed narrowing of the cartilage space and subchondral cyst formation on the femoral side. The Tönnis grade in this patient has progressed from grade 1 to 2. No cases of infection, osteonecrosis, or chondrolysis were identified at the latest follow-up.
Discussion
This study demonstrated that utilizing the SHD approach for femoral neck lengthening combined with various intra-articular procedures has significantly improved the clinical and radiographic outcome in sequelae of childhood hip disorders. It provides a single procedure capable of correcting LLD, trochanteric overgrowth, and abductor insufficiency with few complications. In addition, it allows for simultaneous management of various intra-articular lesions.
In a study involving intra-articular lesions in Perthes and Perthes-like deformities, 5 labral disease was found in 76% of hips, acetabular chondromalacia in 59% of the hips, and FH chondromalacia in 81% of hips. Beck et al. 35 demonstrated a relationship between the shape of the hip and chondro-labral damage in 302 hips that underwent surgical dislocation for intra-articular disease. Anderson et al. 12 reviewed a series of 14 patients with sequelae of Perthes disease and reported OCD lesions of the FH in 28.5%.
Outcomes of combined SHD approach and extra-articular osteotomy for severe hip deformity were infrequently discussed in the literature. Rebello et al., 13 Shin et al., 36 and Albers et al. 37 have similarly utilized this approach, and reported its reliability in management of intra- and extra-articular sources of impingement by providing good exposure, performing osteochondroplasty, allowing dynamic testing of FAI, and addressing the intra-articular chondro-labral disease. However an extra-articular neck lengthening osteotomy was not utilized, and their data did not include assessment of LLD.
RFNL3,12,37,38 through SHD approach may be capable of GT transfer improving abductor function and FAI management, but does not permit simultaneous restoration of the horizontal offset of the proximal femur and correction of LLD. Reports of arthroscopic procedures in Perthes-like deformities have shown good short-term outcome.39–42 This included removal of loose bodies, treatment of chondral flap tears, OCD lesions, and debridement of labral tears and LT ruptures. However, many of the cases we encountered had severe deformities with a significant LLD, requiring complex reconstructions not amenable to arthroscopic or limited open approaches. Hence, a concomitant osteotomy may still be required.
In this study, SHD approach has been found to be beneficial in many aspects. It allowed optimum assessment and treatment of various intra-articular lesions, osteochondroplasty for cam impingement with recontouring of the head-neck junction, labral tears and chondro-labral separations, acetabular and femoral chondral lesions, osteochondral lesions, pathologic LT, and retrieval of loose bodies. The trochanteric flip osteotomy, the initial step of the approach, was utilized later in the procedure for subsequent distal-lateral trochanteric transfer, restoring both abductor tension and abductor lever arm. In addition, the approach optimized trochanteric reduction under direct vision after raising a retinacular flap, instead of a “blind” osteotomy at the head-neck junction. Trochanteric reduction is deemed necessary in many cases to relieve the trochanteric impingement and allows effective distalization of the GT without an excessive bony bump. The approach also provided adequate visualization for the sliding neck lengthening osteotomy at the intertrochanteric level.
The various intra-articular procedures that need to be undertaken should be guided by the patient’s symptoms and preoperative imaging. An anterior cam lesion and/or labral tear that corresponds to a positive anterior impingement test dictates the need for osteochondroplasty with or without labral repair. Similarly, an unstable OCD lesion with mechanical symptoms as locking, catching, or snapping requires intervention.
Regarding the extra-articular osteotomy, a detailed deformity analysis has to be done preoperatively1,31 to determine whether there is coxa vara, coxa brevis, or combined. A valgus component may be added to reorient the position of the FH within the acetabulum improving congruency. It also has the benefit of further improving the LLD by aligning the neck more vertically. A preoperative dynamic view can confirm better congruency when the hip is adducted. Similarly, a largely extruded FH that better contains in abduction may require a varus component. Otherwise, if the orientation of the FH in the acetabulum is to be maintained, a pure sliding osteotomy is conducted. The inclination of the sliding osteotomy can further be manipulated; a more vertical cut will add more length, while a more horizontal cut will increase the lateral offset on the expense of gained length. This has to be tailored on a case-by-case basis. Finally, the derotation component has to be planned according to the preoperative examination to fairly produce equal amounts of internal and external rotation of the hip. We recommend re-evaluation of the rotation after osteochondroplasty since it can add up to 15° of internal rotation. The lateral position utilized in this procedure allows easy intraoperative assessment of rotation with the hip extended.
The amount GT distalization to be undertaken has been investigated in an anatomical study by Beck et al. 43 Based on their laboratory findings, overstretching of the abductors increased the passive forces but decreased the force-generation capacity of the muscle. Furthermore, increased muscle fiber excursion mandated greater energy consumption, which might explain earlier fatigue of hip abductors after GT distalization. They also noticed a change in contraction pattern during abduction from isometric to isotonic. The study concluded that optimal balancing and excursion of the muscle occurs when the tip of the GT is at level with the hip center of hip rotation, and any excessive distalization should be avoided. These conclusions were adopted in this study; the GT was distalized until the tip was at the same horizontal level of the FH center.
The surgical technique in this study has reliably improved all the radiographic parameters of hip morphology. The addition of osteochondroplasty was effective in recontouring of the head-neck junction to restore a normal offset. This has been reflected as improvement in the mean alpha angle from 81.8° preoperatively to 49.5° postoperatively, a measurement that significantly correlates with symptomatic FAI and development of OA.32,44 The ATD significantly improved from −6.7 to 20.8 mm, reflecting a mean distalization of the GT of 27.5 mm. The mean NSA improved form 117.8° preoperatively to 129.8° postoperatively. This was attributed to the effect of neck lengthening osteotomy, where the osteotomy lines align at 130° reshaping the NSA, and in some cases, a valgus component was further added to improve the hip congruency.
A multicenter retrospective series 45 reported the outcomes of a similar technique through SHD conducted on 15 patients including sequelae of DDH and Perthes disease, of which 14 patients had simultaneous PAO. Despite that functional scores were not utilized, the study reported a median improvement in LLD of 11.5 mm (range, 3–30 mm), improvement of ATD in all patients to >5 mm, and increase in NSA by a median of 11°. The study did not utilize measurement of the alpha angle; instead, they relied on the FH extrusion index which decreased from a median of 30% to 17%. At a median follow-up of 17 months, two patients had OA progression and six patients had a decrease of the joint space width.
Recommendations in the literature regarding the indication for PAO in Perthes-like hip deformities remain inconsistent. Anderson et al. 12 relied on acetabular remodeling to adapt to the newly shaped spherical FH and did not perform acetabular procedures in this study group. In agreement with other studies,12,46 we have found that patients with minimal acetabular dysplasia (CEA of 20°–25°) tend to do well after FH reshaping. However, those with more moderate or severe (LCEA of 15°–20° and <15°, respectively) acetabular deficiency or iatrogenic instability after FH reshaping may continue to have symptoms and may need to be subsequently treated with staged PAO depending upon coverage and severity of symptoms.
In the current series, OA progression was observed in one patient with considerable asphericity, high alpha angle, and relative flattening of the FH, with high-grade chondral lesions found intraoperatively. These factors were found to carry a worse prognosis, in agreement with previous reports33,47–49. He had an original pathology of sequelae of septic arthritis dating since the neonatal period, with an HHS of 62 points before the index procedure. Despite a good initial improvement of pain, limb length, and ROM during the first year, he developed radiographic OA progression associated with a poor HHS of 67 points at 5-year follow-up.
While these patients frequently have significant clinical symptoms and limited alternative options, and despite that this procedure may provide a remarkable symptomatic improvement in the short term due to relief of impingement, preoperative counseling should encourage realistic expectations with the patients or caregivers. Using univariate analysis, Albers et al. 37 identified factors that predicted poor outcome in their series. Those included the initial clinical score, alpha angle >50°, Stulberg class >3, the degree of OA, the age, a dysplastic morphology with subluxation, acetabular index >14°, and broken Shenton’s line. They highlighted the importance surgical correction to restore a normal alpha angle (<50°), trochanteric height, and an intact Shenton’s line. Similarly, in a series involving RFNL through SHD in 14 hips with Perthes sequelae, 12 failures were isolated to the Stulberg class IV group, indicating that severity of asphericity and flattening of the head may be the biggest factor in postoperative clinical success.
The study limitations include heterogeneity of the study population. Our study included various childhood and adolescent hip disorders, spanning three age decades, and of different primary etiologies. Several patients in this study underwent previous surgeries as well. On the other hand, regardless of the underlying etiology, these hips share common morphologic features in the shape and alignment of the proximal femur, and the different primary causes may not be currently contributing to the present disability which only reflects altered anatomy and biomechanics. The routine use of preoperative magnetic resonance arthrography with radial sequence to determine focal asphericity of the FH and locations of chondro-labral injuries was not conducted. The authors relied on the patients’ symptoms, impingement tests, plain radiographs, alpha angle measurement, computed tomography, and finally, routine intraoperative examination of the labrum, chondro-labral junctions, and articular cartilage. In addition, advanced magnetic resonance imaging (MRI) techniques conducted in similar studies9,12 were not found to alter neither the inclusion criteria nor the outcome. The HHS used for outcome assessment in this study was not prospectively developed for hip preservation surgery. More recent assessment tools focusing on mechanical symptoms and physical activities relevant to the relatively younger more active patients (as international hip outcome tool-33 and hip and groin outcome score) would have greater validity. The follow-up period in this series is relatively short. Hip preservation surgery aims at extending the longevity of the native hip, delaying or avoiding the need for hip replacement, in addition to improving clinical outcome. Hence, long-term studies need to be conducted determine the extended benefit of comprehensive deformity correction in these lesions.
In conclusion, femoral neck lengthening osteotomy through SHD approach provides a safe and effective surgical treatment of sequelae of Perthes disease and similar conditions, with mild to moderate FH deformity (Stulberg II and III). The presented technique offers a single procedure that can simultaneously address the intra-articular lesions, as well as the extra-articular proximal femoral deformity, hence restoring the proper hip biomechanics, optimizing abductor lever arm, decreasing pain, improving ROM, and improving joint congruency, with concurrent limb-length equalization. Hips with moderate or severe acetabular deficiency or iatrogenic instability after FH reshaping may need to be subsequently treated with staged PAO depending upon coverage and severity of symptoms.
Supplemental Material
sj-docx-1-cho-10.1177_18632521221080477 – Supplemental material for Morscher’s femoral neck lengthening osteotomy through surgical hip dislocation approach for preservation of Perthes and Perthes-like deformities
Supplemental material, sj-docx-1-cho-10.1177_18632521221080477 for Morscher’s femoral neck lengthening osteotomy through surgical hip dislocation approach for preservation of Perthes and Perthes-like deformities by Mostafa M Baraka, Hany M Hefny, Mootaz F Thakeb, Mahmoud A Mahran, Ahmed K El Ghazawy and Tamer A Fayyad in Journal of Children’s Orthopaedics
Footnotes
Author contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was approved by our institution’s Ethical Committee of Scientific Research.
Informed consent
Informed consent was obtained from all individual participants included in the study. All parents consented to and were informed that data concerning this study would be submitted for publication.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.