
Abstract
Abstract
Purpose
Legg-Calvé-Perthes disease is an idiopathic avascular necrosis of the femoral head. Although many surgical approaches to treat the late presentation of this pathology have been proposed, there are few reports about the early results of the double osteotomy procedure (femoral varus osteotomy combined with Salter innominate osteotomy). The purpose of this study was to describe the early results obtained with the double osteotomy in patients with late presentation of Legg-Calvé-Perthes disease.
Methods
Cross-sectional evaluation of ten patients intervened with double osteotomy. There were seven males and three females with a mean age of 9.2 ± 1.7 years [standard deviation (SD)]. The average post-surgical time of evaluation was of 46.5 ± 26.2 months.
Results
Of the ten evaluated patients, four had a Catterall III and six had a Catterall IV disease. According to Herring classification, three patients were Herring B and seven were Herring C. The epiphyseal extrusion average before and after the surgical procedure was 19.3 ± 12.4 and 12.1 ± 14.9%, respectively. In accordance with the Ratliff classification and Lloyd Roberts radiological results, the following were the postoperative clinical results: four good, five fair and one poor. Based on the Stulberg classification, there was one patient in class I, five in class II, three in class III and one in class IV.
Conclusion
The surgical treatment for late Perthes disease with the best expected outcome is still a challenge. According to the resultsreported here, the double osteotomy could be considered as an alternative to treat this entity.
Introduction
The Legg-Calvé-Perthes disease (LCPD) is an idiopathic avascular necrosis of the femoral head, affecting children in its vast majority, especially males in a ratio of three to five males to one female [1]. Although there have been important achievements in the comprehension of the nature of this pathology, the best treatment for LCPD is yet to be achieved.
The main purpose of the management of LCPD is to prevent the deformity of the femoral head and the secondary degenerative osteoarthritis that is seen in most of the patients with the late or severe presentation of the disease [2]. There are multiple approaches to the treatment of LCPD ranging from conservative management to a wide variety of non-surgical and surgical methods. All of these provide the contention of the hip within the acetabular space, in the hope that during the healing phase, the femoral head can become more spherical and with more articular congruence in this position [1].
Among the different surgical approaches that are supported by studies in the orthopedic literature, there is not a specific guideline for the treatment of late presentation LCPD. Even though some surgical techniques are more frequently used than others, there is a lack of uniformity in the way this pathology is treated by different surgeons. Traditionally, two surgical approaches have been used for the treatment of late presentation LCPD; the femoral varus osteotomy and the Salter (innominate) osteotomy. The first technique is considered advantageous due to its safety and the contention of the femoral head within the acetabular space with an adequate coverage. The disadvantages consist of limb shortening with weakness of the abductor mechanism causing gait. The advantage of Salter osteotomy is the better coverage of the femoral head without limb shortening or weakness of the abductor mechanism, but it is a more complex and difficult surgical technique that can cause an increase in the joint pressure leading to articular rigidity after surgery [1, 3, 4].
The first double osteotomy (combination of femoral varus osteotomy and Salter innominate osteotomy) was performed in 1974 by Craig and Kramer for the treatment of severe LCPD with lateral subluxation of the hip [5]. The theoretical advantage of the double osteotomy for the treatment of severe LCPD is that it achieves maximal contention of the femoral head avoiding the complications of each procedure by itself.
The purpose of this study was to describe the early results obtained with double osteotomy in patients with late presentation LCPD given the small amount of information available in the orthopaedic literature related to this field.
Materials and methods
Study design and population
This was a descriptive, cross-sectional study of clinical and radiological evaluation of ten patients treated with femoral double osteotomy for late presentation LCPD. Surgeries were performed by the same pediatric orthopedic surgeon.
For the initial diagnosis, patients’ clinical status was assessed using the clinical and radiological classification of Bombelli [6], Catterall [1, 7], Herring [8], and epiphyseal extrusion [9]. The population consisted of children 8 years of age or older with a Catterall classification graded as III or IV, and Herring classification B and C evaluated at one time point independent of the evolved post-surgical time [1, 7, 8].
Evaluation criteria
Regardless of the elapsed time after surgery, all ten patients were evaluated clinically and new anterior–posterior and lateral hip X-rays were obtained. At this evaluation, patients were classified according to the Bombelli classification [6], the Ratliff classification [10], the Lloyd Roberts scale [11, 12], the Mose index [13–15], the Stulberg classification [2], and epiphyseal extrusion [9].
Ratliff classification categorizes the results as good (>18 points), fair (15–17 points), poor (14–11 points) and bad (<10 points) using four parameters (pain, activity, range of movements and radiological appearance) [10].
The Lloyd Roberts scale evaluates the sphericity and the containment of the femoral head within the acetabulum being considered a good result if a femoral head is spherical, congruous and fully contained with minimal loss of epiphyseal height. A fair result implies a femoral head that is not completely spherical but is congruent, have no more than one-fifth of the femoral head uncovered and mild loss of epiphyseal loss. A poor result has flattening of the femoral head with loss of congruity, greater than one-fifth lateral extrusion, and secondary acetabular changes [11, 12].
Statistical analysis
Data were storage and processed in an Excel® data base and in SPSS® version 10, respectively. For quantitative variables, central tendency and dispersion measures were calculated and for qualitative variables, relative and absolute frequencies were calculated.
Results
There were seven males and three females in the study, with an average age of 9.2 ± 1.7 years (SD) ranging between 8 and 13 years of age. The right hip was affected in seven patients. Before surgery, eight patients complained of pain and all of them had a painful limp. Using the Bombelli classification [6] for hip mobility evaluation on the affected side, we found that six patients had hips with normal mobility, two had low mobility, and one patient had a rigid hip. One patient did not have preoperative data for Bombelli classification.
Patients were classified radiologically before surgery as Catterall III (n = 4) and Catterall IV (n = 6); three patients were classified as Herring B and seven as Herring C. Epiphyseal extrusion averaged 19.3 ± 12.36%. The radiological signs of head-at-risk [1, 7, 8] consisting of lateral calcification of the epiphysis, lateral subluxation of the femoral head, metaphyseal cysts, physeal horizontalization and the Gage sign, were also examined to evaluate the status of the patients. Five patients did not present signs of head-at-risk, two patients had one sign, one patient had three signs, one patient had the five signs, and one patient did not have data (Fig. 1a, b).
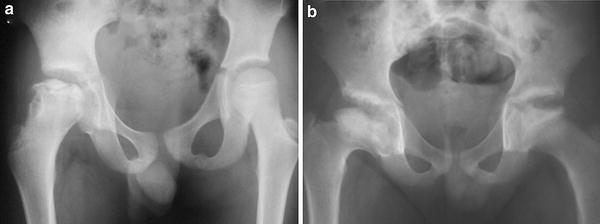
Radiographs of two of the patients before surgery.
The average post-surgical time was of 46.5 ± 26.2 months with a minimum of 18 and a maximum of 82 months of follow-up. At the time of the follow-up evaluation, four patients had a residual limp. Two patients presented pain while walking while the remaining eight did not complain of pain at all. Positive Trendelenburg sign was found in three patients.
According to the Bombelli classification [6] after surgery seven patients had normal mobile hip, two patients had hips with low mobility and one had a rigid hip. Based on the Ratliff classification [10] and Lloyd Roberts radiological results [12], the following were the postoperative clinical results: four good, five fair and one poor. According to the Mose index [13], the following were the radiological results: five good, five poor, with no fair results. Epiphyseal extrusion [9] after surgical procedure was 12.1 ± 14.9%. The post-surgical Stulberg classification [2] showed that one patient was class I, five were class II, three were class III and one was class IV (Figs. 2a, b; 3a, b).

Radiographs of the same two patients in Fig. 1 after surgery.

Radiographs of the same two patients in Fig. 1 after surgery at time of last follow-up.
Three patients required additional treatment; two required valgus femoral osteotomy for an extreme varus and one patient required adductor tenotomy for rigid hip.
Discussion
According to the obtained results from this study, double osteotomy could be considered as an alternative for treatment of patients with late presentation LCPD in which femoral osteotomy or Salter (innominate) osteotomy alone could have not change the natural course of the disease.
The vast majority of articles related to LCPD mention that age and femoral head involvement play an important role in the outcome after treatment [1, 7, 9, 16, 17]. There are many methods to treat this pathology, but in older patients with severe compromise of the femoral head treatment options narrow to a few surgical procedures [1]. One of the most relevant studies about double osteotomy postsurgical results was published by Olney and Asher in 1985 [18]. In this study, after following nine patients with severe LCPD for 4 years and 2 months with a combination of femoral osteotomy and Salter osteotomy, the authors reported good outcomes with this technique and gave specific indications to make use of double osteotomy, implying that it must be reserved for patients with severe disease in whom containment of the femoral head is difficult to obtain by more conventional methods [18]. In agreement with the criteria published by these authors, in the present study older children (average age of 9.2 years) with severe hip disease (Catterall III and IV and Herring class B and class C) were included for surgical correction using double osteotomy.
The clinical outcomes after surgery showed a decrease in pain perception as of the eight patients that related pain before surgery, only two still complain after. According to the Ratliff classification [10], in the present study, good results were obtained in four patients, fair in five patients and poor in one patient. Comparable results were obtained by Olney and Asher where seven patients had good clinical outcomes and only two patients had fair results because of abductor weakness and a limp [18]. In contrast, these results differ from those published by Crutcher and Staheli in a similar study with 14 patients where after an average follow-up of 8 years they obtained good results in 11 patients and fair results in only three patients [11]. The difference of these two studies could be explained by the fact that Crutcher and Staheli evaluated the results using a modified Ratliff scale which does not include the parameter of radiological appearance that was indeed included in the present study.
In studies that describe radiological outcomes of surgical treatment for LCPD, Lloyd–Roberts scale is widely used [11, 12]. Olney and Asher reported four good, four fair and two poor radiological results [18]. Crutcher and Staheli, instead, obtained two good results, whereas 12 were rated fair because many of these hips had a slight degree of femoral flattening or lateral extrusion [11]. In the present study, the early results obtained were four patients with good radiological results, five patients with fair results and one patient with poor results showing improvement of the sphericity and congruence of the severely involved femoral head.
Stulberg et al. by reviewing radiographs taken at skeletal maturity in patients with LCPD developed a classification system that could predict the incidence of osteoarthritis before 50 years of age [2, 11]. In the present study, these early results could indicate a long-term improvement in the prognosis of late presentation LCPD and a decrease in the probability to develop osteoarthritis in adulthood as six patients were rated Stulberg I or II, which implies good prognosis and low incidence of osteoarthritis. Three patients were Stulberg III that implies fair prognosis and late presentation osteoarthritis and only one patient was Stulberg IV. None of the patients was rated as Stulberg V. Crutcher and Staheli reported similar results as well.
In agreement with Olney and Asher, we consider the Mose index to be a strict system for evaluating surgical outcomes in patients that had severe deformed femoral head before treatment as it is almost impossible to obtain a perfect spherical femoral head after surgery [18]. At the same time, this index does not take into account that the aspherical femoral head with joint congruency does not increase the incidence of osteoarthritis, as stated by Stulberg et al. [2] However, according to the Mose index, in the present study, five patients with good results and five with poor results were obtained. These results are compared with those obtained by Olney and Asher, who reported three patients with good results, two with fair results and four with poor; Crutcher and Staheli obtained three patients with good results, four patients with fair and seven patients with poor results [11].
The percentage of femoral head lateral to the Perkin's line in anterior–posterior X-rays with the hips in neutral position (epiphyseal extrusion or index migration) was also used to evaluate radiological outcomes. Epiphyseal extrusion was first proposed by Green et al. [9] as a good prognostic index that could accurately predict the outcome of the disease, suggesting that an index of 20% meant poorer prognosis. Gil and Beguiristain in a study performed in 1992 [19] found that the average migration index of 12 patients after double osteotomy was 29.7% before and 18% after surgery. In the present study, there was a reduction in the averaged epiphyseal extrusion from 19.3 to 12.1%.
Until now, the best treatment for late presentation LCPD is yet to be achieved. With the early results obtained in the present study, we have shown that double osteotomy could be considered as alternative surgical approach in patients with late presentation LCPD. More prospective with higher amount of cases and longer follow-up studies in patients with this disease are needed to increase the evidence for decision-making in order to determine the best treatment for patients with late presentation LCPD.