
Abstract
Chronic pain remains a daunting clinical challenge, affecting 30% of people in the United States and 20% of the global population. People meeting this challenge by achieving wellbeing while living with pain are a virtually untapped source of wisdom about this persistent problem. Employing a concurrent mixed-methods design, we studied 80 people living with chronic pain with “positive stories to tell” using semi-structured interviews and standardized questionnaires. In-depth interviews focused on what helped, what hindered, how they changed, and advice for others in similar circumstances. Major qualitative themes included acceptance, openness, self-efficacy, hope, perseverance, self-regulation, kinesthetic awareness, holistic approaches and integrative therapies, self-care, spirituality, social support, and therapeutic lifestyle behaviors such as music, writing, art, gardening, and spending time in nature. Themes of growth and wisdom included enhanced relationships, perspective, clarity, strength, gratitude, compassion, new directions, and spiritual change. Based on narrative analysis of the interviews and Ardelt's Three-Dimensional Wisdom Model, participants were divided into 2 groups: 59 wisdom exemplars and 21 nonexemplars. Non-exemplar themes were largely negative and in direct contrast to the exemplar themes. Quantitatively, wisdom exemplars scored significantly higher in Openness and Agreeableness and lower in Neuroticism compared to non-exemplars. Wisdom exemplars also scored higher in Wisdom, Gratitude, Forgiveness, and Posttraumatic Growth than non-exemplars, and more exemplars used integrative therapies compared to the non-exemplars. As a whole, the exemplar narratives illustrate a Positive Approach Model (PAM) for living well with pain, which allows for a more expansive pain narrative, provides positive role models for patients and clinicians, and contributes to a broader theoretical perspective on persistent pain.
Introduction
An estimated 20% of the global population lives with chronic pain, 1 with an even higher percentage in the United States, as approximately 1 out of 3 Americans report chronic pain. 2 The heterogeneity of people living with pain 3 and the complexity of the pain experience 4 are acknowledged, but far more attention is paid to the negative pain experience compared to those who adapt well to the challenge of living with persistent pain. Motivational change models focus on the role of self-care and the individual differences in cognition and behavior associated with successful adaptation. 5 Other studies of psychological factors and positive outcomes in people living with pain focus on acceptance and values-based action, 6 and these processes are subsumed under the construct of psychological flexibility. Recent laboratory studies conducted by Farmer et al found that personality differences cluster with serotonin genotype, pain tolerance, and a less stressful physiological response to standardized pain stimuli. Farmer et al propose 2 human pain clusters: PC1 with a more distressing pain response and PC2 with a disposition minimizing the stress response to pain. 7 They suggest that this reproducible variability could help identify people at greater risk for chronic pain (PC1). However, the pathways of less stressful responding may also provide a better understanding of positive pain management and what may be learned in that process.
We think it is important to further study people with the capacity to live well with persistent pain and obtain a “thick description” of their experiences in the larger context of living with pain. We wanted to see if people might also report other positive aspects of the pain experiences, such as positive changes in behavior, empowerment, spiritual growth, and enhanced appreciation of life and relationships, the “silver linings” often reported with serious illness. 8 By asking about living with pain in the context of a life story, we invited people to tell us how they may have benefitted from pain and to describe what that entailed. While the idea of adversarial growth is not without its critics, 9 there is a substantial literature that supports the idea that pain and suffering are sometimes associated with significant personal development.
Theories of psychological development in response to adverse life circumstances date back to antiquity 10 and have been developed in empirical studies of posttraumatic growth 11 and wisdom. 12 People who persevere through daunting difficulties often report significant life improvement, such as greater appreciation of life, more personal strength, improved relationships, increased spirituality and new roles, and these changes are basis for the theory of posttraumatic growth. For an overview of the history of posttraumatic growth, see https://goo.gl/BW0Y2A.
According to Linley, a dialectical relationship exists between coping with adversity and the development of wisdom. 13 The daily flow of events (thesis) is interrupted by the experience of adversity (antithesis), threatening taken-for-granted meanings. 14 If adversity triggers a life review and a reordering of priorities, it might result in greater wisdom (synthesis) by helping individuals gain deeper insights into life and self, overcome self-centeredness, and develop compassion for others.15,16
The work reported here was part of a larger “Wisdom in Medicine” project in which we explored how people live through difficult circumstances and whether their life changes resemble other descriptions of personal growth and wisdom. 10 One group we studied was people living with persistent pain who had positive stories to tell. Living with pain is a complex and highly personal experience, and so we chose Ardelt's 3 Dimensional Wisdom Model (3D-WM) to guide our study. In contrast to models of general wisdom, which emphasize wisdom-related knowledge, 17 the 3D-WM refers to personal wisdom and includes cognitive, reflective, and benevolent components, compatible with most explicit (expert) and implicit (lay) wisdom definitions in the West and East.18,19 By studying pain “success stories,” we allow for a more expansive pain narrative 20 that can provide positive pain role models for patients and clinicians and contribute to a broader perspective on chronic pain.
Methods
Study Design and Overview
Employing a concurrent mixed methods design, the investigators studied 80 people living with chronic pain, using a semi-structured interview guide and standardized questionnaires. Pain conditions were largely typical of the chronic pain population and included musculoskeletal pain, headache, fibromyalgia, congenital conditions, and complications from surgery. Participants were asked to tell their stories of living with pain, what helped them, what hindered them, how they changed, and what advice they had for others in similar circumstances. Prior to the generally hour-long interviews, participants completed questionnaires measuring personality, posttraumatic growth, wisdom, forgiveness, and gratitude. The participant narratives were divided into 2 groups: “wisdom exemplars” and “non-exemplars.” We hypothesized that wisdom exemplars would differ from non-exemplars on the personality factors of Openness to Experience, Posttraumatic Growth, Wisdom, Forgiveness, and Gratitude.
Recruitment and Screening
Participants were recruited with newspaper advertisements in central Virginia, Boston, New Hampshire, and the San Francisco Bay area. The headline of the advertisement read, “LOOKING FOR POSITIVE PEOPLE LIVING WITH PAIN.” The copy of the advertisement read,
The University of Virginia is conducting a study of people who have experienced pain for at least 3 months and who have a positive story to tell. We are looking for participants who have learned important life lessons from their pain experience and who have been changed in a profoundly positive way. We are also studying a smaller group of people who are suffering from pain and who feel pain has not had a positive impact on their lives. Participants will be given a choice of the way in which they will tell their stories: written, audiotaped, or videotaped. Participants will also be required to fill out several questionnaires and be compensated $100 for time and travel.
People responding to the ad were screened to ensure participants had experienced pain for at least 3 months, and a brief pain history was taken. Potential participants were asked to rate the statement: “Pain has taught me important life lessons and has been a positive life-changing experience,” using a 5-point scale with 1=strongly disagree and 5=strongly agree. Interviews were conducted in the summer and fall of 2009. The recruitment goal was to obtain a large sample of people who had positive experiences to report (75%) with the expectation that this recruitment strategy would also result in a smaller comparison group that did not have positive experiences (25%).
The study was approved by the University of Virginia Social and Behavioral Sciences Institutional Review Board (SBS #2008029500). In addition to signing a consent form, participants were asked to sign a material release form to either release their information for public dissemination or to indicate that their information was to be used for research purposes only. Participants whose data are presented here released their information for public dissemination.
The majority of interviews were in person, but some participants wrote their stories in response to a written guide containing the same questions used in the interviews. The interviews began with a scripted introduction and an open-ended question: “I'd like to start by asking you to tell me your story of living with pain.” Follow-up questions were written so that each interview covered the same material, but effort was made to use open-ended questions. For example, each interview contained the question “What helped you to live with pain?” Respondents were also asked, “If you could give your story of living with pain a title, what would it be?”
Rating of Wisdom Exemplars and Non-exemplars
Two independent raters (authors JO and MM) read the interview transcript for evidence of personal growth and wisdom associated with the experience of living with pain. The cognitive, compassionate, and reflective dimensions of Ardelt's Three-Dimensional Wisdom Model (3D-WM) were used as a guide in classifying the narrative as a “Wisdom Exemplar” or a “Non-exemplar.” An example of the cognitive aspect is an awareness of negative beliefs about pain, such as “My body is broken and letting me down” and reframing such a belief to “My body is trying to heal.” Examples of the affective or compassionate domain are acceptance (of pain), gratitude, and compassion for self and others. An example of the reflective domain is enhanced perspective (eg, that an intense pain episode would not last indefinitely and that it was only a matter of time before one would feel better), taking responsibility, and not blaming others.
Each interview was given a global rating on a 1–5 Likert scale, with 1=little or no wisdom, 2=some (minor) wisdom, 4=emerging (moderate) wisdom, and 5=strong wisdom exemplar. We did not use a rating of 3 so that we could categorize each participant as an exemplar or non-exemplar. Strong wisdom exemplars were defined as having many features of wisdom expressed in their interviews. Emerging (moderate) wisdom was defined as having some features of wisdom. Interrater reliability of kappa=.8 was achieved between independent raters of the pain interviews with 6 differences resolved by discussion and consensus agreement between raters. Ratings of 4 or 5 were combined into a “wisdom exemplar” group. Ratings of 1 or 2 were combined into a “non-exemplar” group.
Qualitative Data Analysis
Interviews were digitally video-recorded or audio-recorded and transcribed for content analysis. NVivo8 software (QSR International Pty Ltd, Doncaster, Victoria, Australia) was used to record the analysis of the interview material using constant comparison. The theoretical frameworks of Calhoun and Tedeschi's Posttraumatic Growth Model and Ardelt's 3D-WM informed our analysis. In the first phase of coding structure development, 3 researchers independently read a set of 10 interviews and extracted themes into a preliminary coding structure. Then another set of interviews was coded, expanding the coding structure to accommodate the new material and refining the nodes to reach agreement in theme and subtheme categories. This process was repeated until no new themes emerged and agreement in coding structure was achieved. The researchers then used the final coding structure to separately code another subset of interviews to assure reliability between 2 researchers/coders. Once .85 reliability was established, half of the total number of interviews was coded by each of 2 researchers. Employment status was coded from the interview transcript in the following categories: full-time, part-time, homemaker or volunteer work, and retired. The latter category included all retired regardless of functional status. The use of integrative therapies was coded from the interview transcript and included mind-body therapies, bodywork, energy medicine, herbal and nutritional remedies, hydrotherapy, and acupuncture.
Quantitative Measures
The Posttraumatic Growth Inventory (PTGI)
The PTGI 21 is a 21-item inventory assessed on a 6-point scale (0=no change and 5=very great change) with 5 major domains of posttraumatic growth: greater appreciation of life and changed sense of priorities (eg, “I can better appreciate each day”); warmer, more intimate relationships with others (eg, “I have more compassion for others”); a greater sense of personal strength (eg, “I know better that I can handle difficulties”); recognition of new possibilities or paths for one's life (eg, “I developed new interests”); and spiritual development (eg, “I have a stronger religious faith”). The PTGI has strong internal consistency with Cronbach's α values ranging from .90–.94. and good internal consistency for the 5 subscales with Cronbach's α values ranging from .67 to .85. Test-retest reliability over 2 months is reported to be r=.71. 21 In the current study, Cronbach's α was .94 for the PTGI and ranged from .79 to .89 for the 5 subscales.
The 3-Dimensional Wisdom Scale (3D-WS)
The 3D-WS is a 39-item questionnaire measuring 3 dimensions of wisdom: cognition (the desire to know a deeper truth pertaining to the interpersonal and intrapersonal aspects of life and the acceptance of life's ambiguity and uncertainty, eg, “Ignorance is bliss – reversed”), 14 items; reflection (the ability and willingness to take multiple perspectives into account and to engage in self-examination to overcome projections, eg, “I always try to look at all sides of a problem”), 12 items; and compassion (sympathetic and compassionate love, eg, “Sometimes I feel a real compassion for everyone”), 13 items.. 22 Twenty-four items are presented with a 5-point response scale from “definitely true of myself” to “not true of myself,” and 15 are presented with a 5-point Likert scale from “strongly agree” to “strongly disagree.” The 3D-WS has reported Cronbach's α from .71 to .85 for the 3 dimensions and a 10-month test-retest correlation of .85. A composite wisdom score was computed by averaging the 3 dimensions. In the current study, Cronbach's α were .80, .80, and .79, respectively, for the cognitive, reflective, and compassionate wisdom dimensions and .77 for the composite wisdom score, consisting of the 3 wisdom dimensions (.89 for the 39 items).
The Gratitude Questionnaire (GQ-6)
The GQ-6 is a short, self-report measure of the disposition to experience gratitude. 23 Participants answer 6 items on a 1 to 7 scale (1=strongly disagree and 7=strongly agree). An example of a positive item is “If I had to list everything that I felt grateful for, it would be a very long list.” Two items are reverse-scored to inhibit response bias. An example of a negative item is “Long amounts of time can go by before I feel grateful to something or someone.” The GQ-6 has good internal reliability, with Cronbach's α between .82 and .87. In the current study, Cronbach's α was .87. There is evidence that the GQ-6 is positively related to optimism, life satisfaction, hope, spirituality and religiousness, forgiveness, empathy, and prosocial behavior, and negatively related to depression, anxiety, materialism, and envy.
The Fetzer Forgiveness Scale, Long Form
The Fetzer Forgiveness Scale is a 10-item questionnaire assessing 5 domains of forgiveness: confession, feeling forgiven by God, feeling forgiven by others, forgiving others, and forgiving oneself. 24 An example of an item assessing forgiveness of oneself is “I find it hard to forgive myself for some things that I have done.” Each item is rated on a 1–4 scale with 1=always or almost always, 2=often, 3=seldom, and 4=never. This scale was adapted from items developed by Mauger 25 who demonstrated acceptable internal consistency, with Cronbach's α=.79 and test-retest reliability of .94. The current study α was .70.
The NEO Personality Inventory Revised (NEO-PI_R)
The NEO-PI_R is a global assessment of personality based on the 5-factor model, measuring the interpersonal, motivational, emotional, and attitudinal styles of adults. 26 Internal consistency coefficients range from .86 to .95 for domain scales and from .56 to .90 for facet scales. The 5 domains (factors) measured by the NEO PI-R provide a general description of personality, while the facet scales allow more detailed analysis. These 5 factors and their facet scales include: Neuroticism (Anxiety, Hostility, Depression, Self-Consciousness, Impulsiveness, Vulnerability); Extraversion (Warmth, Gregariousness, Assertiveness, Activity, Excitement-Seeking, Positive Emotions); Openness to Experience (Fantasy, Aesthetics, Feelings, Actions, Ideas, Values); Agreeableness (Trust, Modesty, Compliance, Altruism, Straightforwardness, Tender-Mindedness); Conscientiousness (Competence, Self-Discipline, Achievement-Striving, Dutifulness, Order, Deliberation). The NEO-PI-R form was also used to collect age and gender, data, and these forms were scored by Psychological Assessment Resources, Inc, Lutz, Florida.
Questionnaire and demographic data were entered into an SPSS dataset and SPSS 19 (International Business Machines Corp, Armonk, New York) was used to tabulate participants’ demographics and conduct statistical comparisons between wisdom exemplars and non-exemplars on the quantitative measures.
Results
Eighty participants living with pain completed the study. One hundred thirteen people were screened, 89 were enrolled, and 9 did not complete the study. Of the 9 who did not complete the study, 7 were not able to complete the interview due to scheduling difficulties or lack of response to requests for an interview and 2 moved out of the area. Participant characteristics of age, gender, years living with pain, race and ethnicity, pain type, employment status, geographic region, and response to the screening question are given in Table 1. The proportion of employed to unemployed was greater for the exemplars and differed significantly from the non-exemplars (chi-square=6.2, P<.03).
Participant Demographics and Characteristics

Screening Question Response
Forty-five (56.3%) of recruited participants gave a rating of 5 (strongly agree) to the statement “Pain has taught me important life lessons and has been a positive life-changing experience.” Twenty participants (25%) gave a rating of 4 (somewhat agree), 3 (3.8%) gave a rating of 3 (unsure), 2 (2.6%) gave a rating of 2 (somewhat disagree), and 8 (12.5%) gave a rating of 1 (strongly disagree).
Wisdom Exemplar Classification
Fifty-nine (74%) of the participants were rated to be “wisdom exemplars” with 34 participants (43%) rated as strong wisdom exemplars with many features of wisdom expressed in their interviews, and 25 (32%) as having emerging wisdom, with some characteristics of wisdom. Twenty-one (26%) participants were rated to be “non-exemplars.”
Wisdom Exemplar and Non-exemplar Differences in Personality, Wisdom, Gratitude, Forgiveness, and Posttraumatic Growth
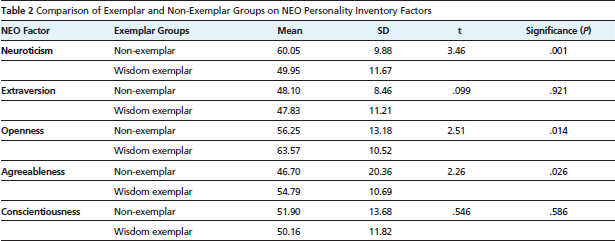
Wisdom exemplars scored higher, on average, in the personality factors of Openness to Experience and Agreeableness and lower in Neuroticism than non-exemplars. Comparisons of Exemplars and Non-exemplars on the factors of the NEO-PI are shown in Table 2.
Comparison of Exemplar and Non-Exemplar Groups on NEO Personality Inventory Factors
Differences between the Exemplar and Non-exemplar groups on the quantitative measures are shown in the Figure. Wisdom exemplars tended to score higher on the 3D-WM with a mean of 3.9 (SD =.3) compared to non-exemplars with a mean of 3.6 (SD=.32), t=6.5, P<.001. Wisdom exemplars tended to score higher on the GQ-6 with a mean of 37.8 (SD=3.92) compared to non-exemplars with a mean of 34.7 (SD=8.31) t=2.2, P<.04. The exemplars also tended to score higher on Forgiveness with a mean of 22.6 (SD=2.36) compared to the non-exemplars with a mean of 20.7 (SD=2.35) t=3.0, P<.004. Average scores on the PTGI were higher in the exemplar group with an average of 66.6 (SD=20.54) compared to the non-exemplars with an average score of 54.3 (SD=23.23), t=2.3, P<.03. More wisdom exemplars (74.1%) reported using integrative therapies compared to 45% of non-exemplars. This difference is significant, chi-square=6.3, P<.03.
Qualitative Themes
The narratives of the wisdom exemplars were more complex than the non-exemplars, and this complexity is reflected in the tables summarizing the exemplar and non-exemplar themes.
Non-exemplars generally expressed a lack of acceptance of their pain and a range of negative emotions, including anger, sadness, low self-esteem, pessimism about the future, and an inability to forgive and deal with repressed emotions. Some expressed openness to new approaches, while others did not. Similarly, some described positive spiritual experiences, while others were more negative about spirituality. Use of mind-body control and integrative therapies was typically described in the beginning stages if at all, and success with these approaches was mixed. Many talked about their inability to calm their minds, relax tension, or commit time for self-care and cited cost as an issue for massage and other integrative therapies not covered by insurance. Social support was typically described as poor. These themes are well known in the psychology of those adapting poorly to living with pain. Representative quotes are presented in Appendix 1, available as supplementary material at www.gahmj.com.
Characteristics of the exemplars and self-regulation themes are presented in Table 3. Acceptance played an important role in many exemplar narratives, in the short-term of not fighting against pain and causing more tension but also in the longer term of realistically assessing their situations. They repeatedly expressed an interest in trying new approaches and the importance of keeping an open mind. The exemplar narratives contained strong elements of hope, optimism, and self-efficacy. Many described keeping in mind the encouraging words of healthcare professionals and using affirmations to stay motivated. They focused on small incremental improvements and perseverance.
Exemplar Characteristics and Self-regulation Capacities
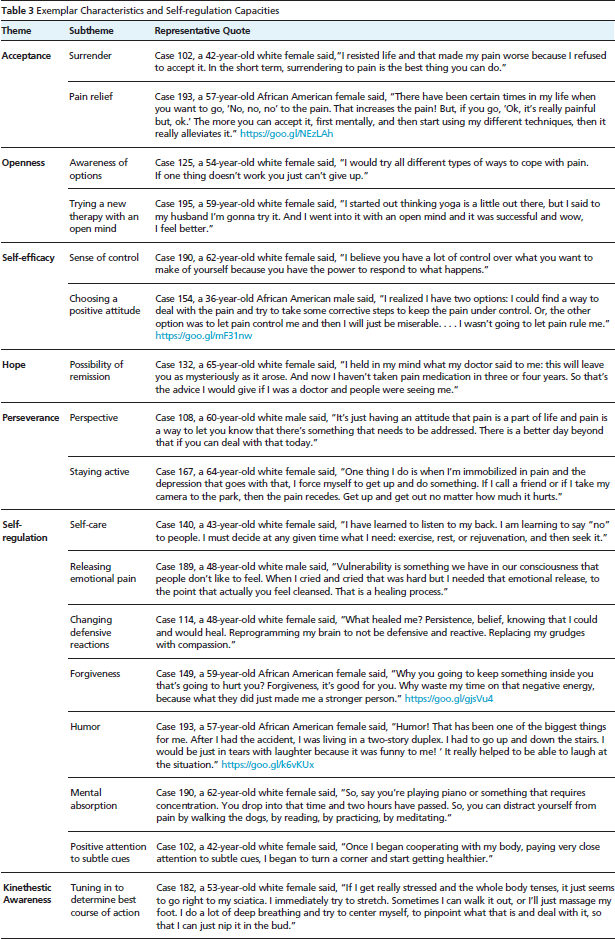
As a rule, the exemplars were mindful of the connection between stress, negative emotions, and pain and realized the value of letting go of negative feelings and improving their responses to negative circumstances. Most expressed a strong commitment to forgiveness, while others described continuing to work on this area. In general, exemplars expressed enthusiasm about the learning process of self-regulation and life improvement. Positive experiences with self-regulation of pain were typically linked to feelings of control and further empowerment. They described the importance of humor and becoming fully absorbed in pleasurable activities in maintaining a positive perspective. A sense of balance and enhanced kinesthetic awareness was expressed by many exemplars: staying active but resting when necessary (pacing), having learned when to push themselves and when to take time for rest, relaxation, reflection, recreation, and restoration (Table 3).
Themes concerning use of integrative therapies and therapeutic lifestyle behaviors are presented in Table 4. As a whole, the exemplar narratives illustrate the success of a multifaceted approach to living well with persistent pain—the bio-psycho-social-spiritual model in practice. This is reflected in a preference for holistic approaches, with an emphasis on good nutrition and healthful lifestyles. Many expressed a strong desire to minimize or eliminate pain medication, preferring mind/body approaches and integrative therapies, although many acknowledged that medications had played or continued to play a necessary role on occasion. Many exemplars described a high level of success with mind-body control over pain, not only with contemplative practices such as meditation and yoga but also with lifestyle activities that involved quiet, contemplative states and focused attention, such as gardening, art, music, and time in nature. Some exemplars focused on specific body therapies in promoting re-alignment of posture, neuromuscular reeducation of patterns of tension, and the importance of bodywork maintenance. Others focused more on cognitive retraining and mindfulness and described pondering existential questions, the helpfulness of journal keeping, and expressive writing. Many described the importance of spiritual practices. While a few were agnostic in their beliefs, they typically had well-developed philosophies about how to live a good life. Many kept gratitude journals and several described spiritual healing experiences that were perceived as turning points. As a rule, the exemplars had strong, positive social networks and attributed to this support an integral role in helping maintain their wellbeing.
Integrative Approaches and Therapeutic Lifestyle Behaviors


On average, the Exemplar group scored higher on wisdom, gratitude, forgiveness, and posttraumatic growth, and a higher percentage used integrative therapies compared to the Non-exemplar group.
Themes expressing the facets of Posttraumatic Growth and Wisdom are presented in Table 5. Most described an enhanced appreciation of life. In particular, much gratitude was expressed not only for pain-free times but also for how much they had learned and grown. They typically felt stronger as individuals, having been tested and survived, and felt more connected to others, having developed stronger relationships. Several talked about changing professions to help others in pain or taking classes as steps in that direction. Enhanced spirituality was often described, as their experiences made them more aware of life's complexity and prompted them to think more deeply about the meaning of life, mortality, and priorities. Most described having more compassion for others’ suffering and a desire to help and comfort others in pain. Growth in cognitive capacity was described as greater awareness and a restructuring of beliefs that did not serve them well and also with a general enthusiasm for understanding the meaning of their experiences. They described clearer perceptions and increasing control over negative reactions and projections in challenging circumstances.
Growth and Wisdom Themes

A comparison of the non-exemplar and exemplar story titles is presented in Appendix 2, available at www.gahmj.com. The story titles of the exemplars are predominantly positive compared to the non-exemplar titles that are mostly negative, although some hint at potential positive trajectories. The idea of a path or journey was the most common theme in both the exemplars and non-exemplars, typically conveying a passage through difficulty, from darkness to light. The exemplar titles tended to describe a positive end to the journey, such as “A Journey to Wholeness With Pain as the Teacher” compared to the non-exemplar titles conveying the struggle. Other themes common to the exemplars and non-exemplars were perseverance, communication, learning, and individuality. Themes unique to the exemplars were transformation, enlightenment, gratitude, hope, friendship, perspective, forgiveness, and peace, although 1 non-exemplar conveyed gratitude for the relief obtained from medication. Themes unique to non-exemplars were complaints about pain, holding on to grudges, lack of meaning, loss, denial, and chaos.
Discussion
People living with pain with positive stories to tell provide qualitative and quantitative support for the age-old idea that dealing well with adversity is, for some people, associated with growth and wisdom. Most of the wisdom exemplars we studied were not just coping well with pain, they were thriving.
The exemplar and non-exemplar narratives illustrate the motivational change model and the stages of self-care. The exemplars describe the action/maintenance stage 27 and the skills of effective copers, specifically exercise, persistence, cognitive control, relaxation, pacing, assertive communication, and proper body mechanics. 28 In contrast, the non-exemplars portray the pre-contemplation or contemplation stage, with some action toward self-care. 4 They describe difficulty calming their minds, not paying positive attention to their bodies, and not committing time for self-care, citing cost as an issue in therapies such as massage. The non-exemplars scored lower on Agreeableness than the exemplars and reported difficulty with relationships. Their lower scores on Openness are consistent with less interest in cultural pursuits and difficulty with concentration.
As a rule, the exemplars are mindful of the relationship between stress and pain and they work on choosing how to respond to adverse circumstances. Choosing how to respond to negative situations is a hallmark of wisdom, and exemplars describe this level of awareness and choice. For more on choosing positive responses and wisdom listen to https://goo.gl/YPFPDm.
The exemplars typically describe many ways of nurturing wellbeing. A review of therapeutic lifestyle behaviors 29 listed exercise, nutrition, relationships, giving back, nature, relaxation, recreation, and spirituality, and these behaviors dominate the exemplar narratives. Humor is also described as a way to stay positive and better tolerate pain. 30 The exemplars describe shifting attention away from pain and getting absorbed in positive experiences, providing distraction, relaxation, pleasure, and periods of concentration that were compared to meditative states. They reflected on the meaning of pain, suffering and mortality, processes thought to promote posttraumatic growth 11 and wisdom. 12 A recent review of spirituality and health concluded that a spiritual life is associated with a positive outlook, emotional comfort, and health-promoting behaviors, 31 all of which are illustrated in the exemplar narratives. Exemplars tended to score higher on the Gratitude Scale compared to non-exemplars. Gratitude can be a powerful way to promote positive affect 32 and may also have a protective effect in extinguishing fear of movement-related pain. 33 In addition to prayer and going to church, several exemplars presented pivotal spiritual experiences at sacred sites, in, for example, Wales, Greece, and Brazil. The exemplars typically described themselves as forgiving and scored higher on average than the non-exemplars on the Forgiveness Scale. Forgiveness is related to lower distress in low back pain patients. 34 Exemplars tended to score significantly lower than the non-exemplars on all the Neuroticism facets.
Leading theorists in the positive psychology movement link wellbeing to character strengths and virtues, 35 and this association echoes through the exemplar narratives. Ardelt defines wisdom as the knowledge it takes to lead a “good life,” to do the right thing for self and society. See https://goo.gl/JFDgyN.
The exemplars tended to score high on Openness, and this trait deserves special attention. It should be noted that 34% of the exemplars scored high (55–65) on Openness and 42% of the exemplars scored very high on Openness (66–83). Previous studies of adaptive vs distressed people living with pains reported significant difference in Openness, 3 and the association between psychological flexibility and positive outcomes corroborates previous findings. 36 But Openness is a complex trait that goes beyond a willingness to try new behaviors and consider new ideas. It is also related to higher involvement with aesthetic experiences and a greater capacity for focused attention and self-regulation.
Openness is consistently correlated with hypnotizability and the Mental Absorption Scale, 37 measures that tap into the capacity for focused attention, endogenous analgesia, imperviousness to distraction, and the ability to shift attention away from noxious sensations. 38 Many studies have demonstrated the ability of high-Absorption subjects to self-regulate physiological processes, 39 beginning with the demonstration that high-Absorption subjects relax more quickly and deeply without a signal in biofeedback studies. 40 The exemplars describe these capacities along with their greater use of integrative therapies, replicating previous findings. 39 Exemplars describe enhanced kinesthetic awareness (a facet of the Absorption Scale) helping them deal proactively with impending flare-ups. In general, the exemplar accounts illustrate the synergy of positive expectancy and self-regulation capacities, factors associated with placebo responding and positive healthcare outcomes. 41
Many exemplars embrace a holistic approach to living and illustrate the wide variation in the elements of integrative pain management. For example, Pam started with a nutritional makeover, weight loss, and body building supported with chiropractic, massage, yoga, mineral baths, and affirmations. Joe relied on his background in martial arts, scripture, nutrition, ice packs, and helping others. Maurice enjoyed ironing, as the calm, focused attention gave him energy. He exercised and attended a men's group. A recent overview of integrative pain medicine focused on nutrition, mind-body neuroplasticity, and subtle nerve dysfunction in myofascial tissue. 42 The emerging picture is that body therapies, self-regulation, and nutrition may work in concert to ameliorate tissue dysfunction, and these elements may be achieved through a variety of choices leading to similar conditions. 43
A positive approach toward pain is an apt global characterization of the exemplar narratives, as the exemplars persisted in approaching pain with positive attention and behaviors. It is noteworthy that the concept of mindfulness rests on an approach stance to experience, and the cultivation of mindful attention reduces distress 44 and is thought to ultimately lead to growth and wisdom.42,43 The distinction between an approach orientation vs an avoidance response is the central construct integrating research on self-regulation of stress and wellbeing45,46 and may be useful in understanding the success of the exemplars. We propose a preliminary Positive Approach Model (PAM) of pain to complement the Fear Avoidance Model (FAM) and to more completely represent the persistent pain experience. The exemplar narratives suggest that the negative pain cycle can be interrupted with persistent positive approaches, supporting the development of psychological maturity in the process. The concept that pain can lead to personal growth if approached with a positive attitude is not new, 47 but the scientific study of this age-old idea is just beginning. We hope that proposing the PAM model may lead to further investigation of approaching pain with positive attitudes and behaviors and the potential for personal growth and wisdom.
The constructs of growth and wisdom are interrelated as wisdom is thought to be the hallmark of psychological maturity. 12 The paradoxical nature of life and adversity—that suffering is negative but can bring about positive changes—was expressed by many exemplars. They often preceded this sentiment with a version of “This may sound funny but …” Yet the conviction that the experience of pain had many positive aspects was strong. For more on the relationship of posttraumatic growth and wisdom listen to https://goo.gl/AC3zkY.
It should be noted that this study was not designed to show that living with pain causes a person to become wise, and we are not claiming that. We see the relationship between pain, growth, and wisdom as more circular than linear, as the wisdom exemplars appeared committed to approaching life with a positive perspective. However, descriptive studies have inherent limitations, and our study is limited to retrospective reports that cannot answer the questions that might be addressed by longitudinal studies of how pain may promote psychological growth. Typically, the exemplars reported a high quality of life prior to the onset of pain and seemed to draw upon this previous experience in their sustained efforts to regain a good life. The extraordinary perseverance illustrated in the exemplar narratives may be viewed in terms of well-established reward pathways—as it may be easier to re-instate rewarding lifestyle behaviors than learn them anew—and an instilled disciplined character. But these are only descriptive observations based on retrospective narratives, and further study is needed to investigate how previous positive life experience influences responses to persistent pain.
Many exemplars expressed the hope that their stories might help others. The strong message of many exemplars is that there is “good news” associated with living with pain—beyond mere coping and recovery—and greater awareness of their stories can help potentiate those outcomes. The exemplar narratives also illustrate the current guidelines for pain treatment: the need for interdisciplinary assessment, the importance of recognizing sub-populations, and the use of integrative therapies, 2 although these guidelines are not currently in widespread practice. Providing early intervention in positive approaches might lead to less suffering, reduced use of medications and risk of opioid addiction, quicker recovery, greater productivity and wellbeing, as well as personal growth and wisdom for those facing the challenge of living with pain.
Footnotes
Acknowledgments
We gratefully acknowledge the generous financial support of the John Templeton Foundation. We are also deeply appreciative of the participants, who shared their stories and enthusiasm for studying the positive aspects of living with pain. Betsy Brantley was instrumental in setting up procedures for screening participants and data collection. Sarah Thaden was responsible for ensuring data entry accuracy and protection of confidentiality in the narratives of participants who did not wish to release their identities. We gratefully acknowledge their efforts.