
Abstract
Background/Objective
Pain is one of the most common chronic conditions in the US, estimated to affect 20.9% of the population (51.6 million people). We evaluated the Partners Aligned in Transformative Healing (PATH) program at University Medical Center’s Comprehensive Pain Program clinic. Feasibility, initial clinical and financial results were assessed to inform payers’ support for PATH, an integrative transdisciplinary program within a bundled payment format.
Methods
Participants completed a multi-week program including integrative therapies, with empirically validated assessment surveys administered at the beginning and end of the program. Insurance claims data were analyzed 12 months pre- and post-program. Statistical significance of pre-post differences was assessed by paired T-tests with P < 0.05.
Results
Between June 2019 and August 2022, 170 individuals enrolled in PATH, 151 (88.8%) completed the program, and 121 participants completed outcome surveys. Participants were predominately White, non-Hispanic (98%), female (76%), with an average age of 49.8. All participant-reported clinical outcomes (PROs) showed statistically significant improvement from baseline to final assessment, and some but not all were clinically significant. PEG subscale of average pain interference, enjoyment of life, and interference with general activity each decreased. The T-scores for the following domains of PROMIS-29 decreased: Pain interference; fatigue; sleep disturbance; anxiety, and depression. The PROMIS-29 domains of overall physical function and social roles and activities mean T-scores increased. Per Member Per Month (PMPM) total cost of care decreased by $462 (18%). Emergency room utilization for all diagnoses decreased by 457 visits/1000 patients (65%), and for pain-related diagnoses by 194 visits/1000 patients (67%) during the observation period.
Conclusions
Results suggest that the PATH Program is a feasible and acceptable model that shows initial effectiveness relative to short-term patient-reported clinical outcomes and shows signs of durability in both utilization and financial outcomes at 1 year. The results support continued study including a multi-site RCT.
Keywords
Introduction
Chronic pain is one of the most common chronic conditions in the United States based on multiple prevalence studies 1 with the most recent national estimate at 20.9% of US adults. 2 Like many conditions, chronic pain spans a spectrum of severity and functional impact. In 2016, the Center for Disease Control (CDC) created a National Pain Strategy that called for more precise prevalence estimates of chronic pain with a focus on more granular definitions of the severity and impact of pain. A new classification, “high impact chronic pain” has emerged as a result and defines a chronic pain experience that results in limitations in major life domains including work, social, recreational, and self-care activities. 3 This classification distinguishes it from those who maintain normal life activities despite chronic pain. The prevalence of high impact chronic pain is between 4.8%–8%.4,5 As a comparison, in 2021 the overall prevalence of diabetes in the United States was 8.9%. 6
Healthy People 2030, a program of the US Department of Health and Human Services has a primary goal to “reduce high impact chronic pain and misuse of prescription pain relievers”. 3 Secondary goals include reducing the current proportion of adults who have high impact chronic pain that frequently limits life or work activities. Substantial reductions were observed from 2019-2021, meeting the 2030 target of reducing this prevalence to 6.4%. While this translates to nearly 1.7 million fewer people experiencing high impact chronic pain, 6.4% prevalence still represents nearly 21.5 million people and their families who continue to suffer. Additional objectives of Healthy People 2030 include increasing the self-management of high impact chronic pain and reducing the impact of high impact chronic pain on family and significant others. 3
CDC’s 2016 “Guideline for Prescribing Opioids for Chronic Pain” called for clinicians to maximize the use of non-opioid treatments, discuss risks and benefits for those on opioid treatment, taper if patients were interested and motivated, closely monitor and mitigate overdose risk, and offer and arrange medication-assisted treatment when opioid use disorder is identified. 5 In 2019, Dowel et al published a commentary that re-emphasized that the CDC guideline calls for maximizing use of physical, psychological, and multimodal pain treatments, which have not been available, used, or reimbursed sufficiently. 7 The CDC has supported non-opioid pain treatment research with the goal of increasing the use of these treatments and increasing insurance coverage. 8 A number of non-opioid pain treatments have demonstrated efficacy.9,10
In response to this need, the University of Vermont Medical Center established the Comprehensive Pain Program (CPP) to improve treatment options for people struggling with chronic pain. One of the treatment options available at CPP and the focus of this paper is the PATH (Partners Aligned in Transformative Healing) program, which brings together medical and mental health treatments combined with a variety of integrative therapies in a transdisciplinary model of care, including both group and individual treatments over several months. CPP’s approach to high impact chronic pain models a ‘Whole Person’ approach to the treatment of chronic pain, emphasizing non-interventional, self-directed, integrative pain treatments. CPP successfully co-developed a financial model of support with Blue Cross Blue Shield of Vermont (BCBSVT), which pays for care over the program’s sixteen-week duration in a “bundle” format. The bundle is divided into monthly claim intervals, and covers the cost of the entire program, including all group and individual services. Participant’s financial responsibility is equivalent to the copayment for a primary care appointment each month, thus minimizing financial burden to participants.
The objective of the PATH program is to equip participants with knowledge and skills intended to optimize management of their pain, including the utilization of integrative health services not traditionally covered through commercial or public Fee-For-Services (FFS) insurance models. The overarching goals of the program are to optimize comfort, ease suffering, and improve participants’ functional status.
PATH Program Overview
The PATH program starts with a medical intake visit where a comprehensive patient history and pertinent physical exam components are obtained. Eligibility for the program is assessed at this visit. All participants are either referred by primary or specialty care providers or self-referred. Participants must be age 18 or over, have had chronic pain lasting 3 months or longer that affects – or has the potential to affect – one’s mental health, family relationships, social relationships, and/or ability to work. PATH serves any adult with HICP, so they have a wide variety of musculoskeletal degenerative diseases coupled with comorbid mental health challenges, typical of a high impact chronic pain population.11,12 They must have adequate concentration and memory function to learn and apply new information. They must not have any other significant pending medical workup for a pain-related condition. They must be stable from a psychiatric perspective without untreated substance use disorder or a significant untreated personality or thought disorder. They must have a willingness to participate actively in groups and therapies and the ability to sign an informed consent for care. Prior to this visit, participants complete a questionnaire that includes the below health survey tools, demographic information, subjective description of their pain experience and symptoms as well as screens for depression (PHQ-2), 13 anxiety (GAD-2,13 PTSD/trauma (PC-PTSD-5), 14 alcohol abuse (AUDIT-C) 15 and Kinesiophobia (3 questions adapted from the Tampa Scale of Kinesiophobia). 16
These tools were only used as clinical screens and were not analyzed as part of this pilot study, additionally, each eligible individual is called by the PATH Program Coordinator to review details of program format and schedule. The Program Coordinator further assesses the individual’s availability for and ability to enroll in a 16-week program by reviewing family support and responsibilities, work schedule, transportation, working technology and any potential barriers to entry. Continued follow up with the Program Coordinator occurs to mitigate potential barriers.
Following an intake visit conducted by one of the physicians or nurse practitioners, the participant’s history is shared in a transdisciplinary meeting of all integrative practitioners. In this session, clinicians from all backgrounds are asked to make recommendations for the patient regarding the potential value of their particular therapeutic approach. These recommendations are then shared with the participant at their orientation session at the beginning of the program. The care team reviews each participant’s experience and response to therapies again at the midpoint of the episode of care and prior to graduation. The participant is not present at these meetings. Participants receive suggestions that arise following the midpoint integrative review and receive recommendations regarding continued care upon graduation from the program.
Informal transdisciplinary work happens through an amalgam of working in a shared clinical space and connection through a shared electronic medical record with access to instant messaging and other HIPAA appropriate asynchronous communication through provider notes. The transdisciplinary staff also meets regularly to address operations and affords the opportunity for interaction around participant care as needed.
Therapeutic offerings available in the program include Acceptance and Commitment Therapy (ACT), Acupuncture, Art Therapy, Clinical Hypnotherapy, Craniosacral Therapy, EMDR (Eye Movement Desensitization and Reprocessing), Health Coaching, Massage, Medical Group Visits and Medical Consults, Meditation and mindfulness instruction, Nutrition Consults, Psychologically-Informed Physical and Occupational Therapies, Reiki, and Yoga. Additional group educational offerings include cooking classes and a rotation of nutrition-based topics with a dietician, education on medical uses of cannabis, an introduction to EMDR, yoga classes, and a Care Alliance Group for participants’ loved ones. The integrated care team is comprised of acupuncturists, a chef educator, a clinical dietician, massage therapists, movement specialists, nurses, nurse practitioners, physicians, a psychiatrist, psychologically-informed physical therapists, a psychologically-informed occupational therapist, a health coach, a psychologist, Reiki practitioners, and a clinical social worker. All therapies are provided at the Comprehensive Pain Program Clinic (or on-line) by providers appropriately certified and/or licensed for the therapy provided.
During the PATH program’s episode of care (See Supplemental Figure 1 for a snapshot of the program), participants engage in weekly group sessions with either one or two facilitators around an established and standardized curriculum. Each group consists of no more than 12 participants to optimize group dynamics. Individual therapies are provided to participants each week as recommended by their care team and chosen by the participant. The three highly utilized therapies of Reiki, massage and acupuncture are offered in 8-week blocks, starting 2 weeks apart, during the 16-week program (Reiki is available weeks 3-10; massage is available weeks 5-12; and acupuncture is available weeks 7-14). Participants are free to access care within the bundle as frequently as they need within the scheduled availability of the provider. Not all patients receive all modalities offered by the program. All providers are available regularly at the clinic for patient interactions with the participants.
Participants are placed into a closed “cohort” that meets weekly at the same day and time throughout the PATH program. The program begins with 6 weeks of ACT group sessions called “COMPASS Living”. Compass stands for “Continuing On My Path And Strengthening my Story” and focuses on how to decrease suffering and increase quality of life by doing more of what matters, despite having pain. These sessions are facilitated by a mental health professional. Woven into the first half of the PATH curriculum are group educational sessions including Pain Neuroscience Education (PNE) provided by a psychologically informed physical therapist, and a “Food Kit” presentation by a registered dietician.
During the second half of the PATH program, there are six weekly medical group visits called “Openings”. These sessions build upon the skills and momentum developed in the first half of the program and focus on supporting the participant in framing the experience of chronic pain using the following four pillars: self-compassion, spirituality or meaning-making, mindfulness, and community/connection. During Openings, medical consultation opportunities are identified within the group on a weekly basis and provided on an individual basis as needed. The medical group visits are facilitated by a medical provider and a co-facilitator with medical and/or integrative training (i.e., an RN who is also a Reiki practitioner).
In addition to the foundational weekly group sessions described above, participants have the option to attend other group offerings (shown in Supplemental Table 1) that are available to anyone actively involved in treatment at CPP. Group attendees may be from different cohorts who may be at varying stages of their program. Individual therapies outlined previously are available throughout the PATH program. In addition, a midpoint and a final visit occur with the intake medical provider to assess progress and provide input to the care plan and provide consultation if needed.
A final care plan is developed jointly by the team at the end of the program and presented, along with an extensive resource list, at the final group visit and graduation, which ends the bundled episode of care. Following graduation, alumni group support is offered monthly at no charge to participants as are free weekly virtual yoga classes and virtual mindfulness meditation sessions via telehealth. Self-guided tools are provided to the participants throughout the program. Pre-recorded mindfulness exercises and yoga classes led by program providers are made freely available via YouTube.
As a new program, PATH evolved over time, starting as an 8-week program from June 2019 to September 2020. Considering participant feedback that the program was too intense and time-consuming, PATH was extended to a 13-week program from January 2021 to January 2022, and ultimately expanded to the current 16-week format to accommodate a predominately working participant population who could not commit the time needed to attend the program and access the various integrative therapies. The expanded duration decompressed the schedule while the program content, time commitment, and availability of therapies did not change as the program was lengthened.
This program began shortly before the onset of the COVID-19 pandemic, at which time PATH was quickly shifted to a fully virtual approach, and initially limited access to all in-person modalities. Over time, these in-person treatments were resumed in a safety-optimized manner as per the medical center guidelines. Currently, the PATH program continues to offer a mix of both in person and virtual participation in each cohort.
Purpose of the Study
This pilot evaluation assessed the feasibility, and preliminary clinical and financial results of PATH. We evaluated the recruitment and retention of PATH participants, the change in participant self-reported measures of pain, psychological well-being, and function, and the anticipated value of the program to payers through change in health care cost and utilization. We also qualitatively assessed the delivery of this multiple activity program. This pilot evaluation was deemed exempt from review by the University of Vermont Committee on Human Subjects Research in the Medical Sciences.
Methodology
Study Design
PATH is offered as a group program with a maximum of 12 participants in each cohort. Upon being assessed as meeting the inclusion/exclusion criteria, participants are added to the next available cohort, and all participants in each cohort start the program together. This study includes all cohorts that started on or after June, 2019, and were completed by August, 2022.
Feasibility Study Inclusion/Exclusion Criteria
All participants starting the PATH program were included for the purpose of feasibility assessment. PATH program inclusion criteria can be found in the PATH Program Overview section above. All participants who completed the PATH program and completed both pre- and post-outcome surveys are included for the purpose of preliminary patient outcomes analysis. All participants who completed at least half of the PATH program and had continuous BCBSVT coverage for at least 6 months pre- and 6 months post-program are included for the purposes of cost and utilization analysis.
Outcome Measures
The primary outcomes for this study are (1) feasibility, measured by participant retention, provider availability, and formal participant and informal provider feedback; (2) preliminary participant self-reported measures of pain, psychological well-being, and function; and (3) preliminary health care costs and utilization measures. Data was analyzed using Microsoft Excel Version 16.77.1 and STATA 17.0, StataCorp. 2023. Stata 17. College Station, TX.
Feasibility
Participant completion rate is used as a measure of program practicality for the participants, measured as the percentage of those who start the program who go on to complete the entire program. We also calculate the percentage of those referred to PATH who enroll in the program. This is a program with many optional services, dependent on the local availability of providers for each of them. An informal assessment by providers during the program, as well as a formal feedback survey of participants at Graduation is used to determine how well the program meets these needs.
Patient Reported Outcomes
In this initial pilot evaluation, participants complete validated health survey measures at the beginning and at the end of the program. Health survey measures include the PEG scale (Pain intensity [P], interference with Enjoyment of life [E], and interference with General activity [G]). 17 Patient-Reported Outcomes Measurement Information System (PROMIS®)–29, 18 Brief Resilience Scale, 19 Self-Compassion Scale, 20 Chronic Pain Acceptance Questionnaire-8,21 and the Health Confidence Scale. 22 All measures were administered pre- and post-intervention.
The PEG scale is a validated brief survey which is used among primary care and other ambulatory clinic patients to improve assessment and monitoring of chronic pain. 17 The PEG scale is included to obtain averages in the past week related to pain rating, pain interference with enjoyment of life, and pain interference with general activity.
The PROMIS-29 assesses multiple functional domains including physical function; fatigue; pain interference; depressive symptoms; anxiety; ability to participate in social roles and activities; and sleep disturbance. 18 It has been validated for use in assessing impacts of health care interventions. 18
The Brief Resilience Scale measures one’s perception of their ability to bounce back and recover from stress. This validated measure correlates with both resilience resources and health outcomes. 19 Resilience is an important skill to develop for those living with high impact chronic pain. Studies indicate that those who are more resilient to pain adopt more adaptive coping strategies to pain. 23 and that failure of resilience may contribute to the development of chronic pain. 24
The Self Compassion Scale - Short form, validated in general populations, measures self-compassion as well as the 6 second-order factors of self-kindness, self-judgment, common humanity, isolation, mindfulness and over-identification, and has been shown to be positively correlated with psychological health. 20 Self-compassion is positively associated with pain acceptance, and use of pain coping strategies, and may be effective in reducing pain interference. 25
The Chronic Pain Acceptance Questionnaire-8 (CPAQ-8), a validated 8 item measure of chronic pain acceptance 21 is a significant predictor of reliable change in depression, anxiety and disability in populations of patients with chronic pain, above that of pain intensity alone. 26
The Health Confidence Scale is a simple and validated tool used often in primary care settings. Higher health confidence can lead to the person taking actions that improve their health outcomes and reduce utilization of health care services. 22 The brief single question pain scale is used in this study as opposed to a longer what matters index. In addition, the single question was modified to reflect the program’s focus on chronic pain: “How confident are you that you can successfully control and manage your pain?”
Health Care Cost and Utilization
BCBSVT claims data is analyzed for total costs of care, medical costs, pharmaceutical costs, and musculoskeletal-coded specific costs using a proprietary diagnosis-related grouping system developed by 3M and used by the payer. Utilization rates/1000 people for emergency room visits are also evaluated. Claims data for the time periods 12 months prior to the program and the 12 months following graduation from the program are analyzed for participants who completed at least half of the program. We have followed the insurance industry standard by presenting the cost measures as per member per month (PMPM) mean values.
Data Collection and Privacy
During the period of this study, all data collection was on paper, at the medical intake visit, the start of the program, and completion of the program. Participants are requested to complete a questionnaire at home prior to coming to the Comprehensive Pain Program clinic at these 3 milestones, or sending it by secure electronic methods for those attending virtually. The Program Coordinator is responsible for securing all paper questionnaires in a locked file cabinet, in a locked room, in the locked CPP clinic.
Results
Participants and Retention
Participant Demographics (n = 170).

This table includes all participants who enrolled in the PATH program n = 170.
Total participants screened n = 175.

PATH program participant flow.
PATH Participant Retention.

Patient-Reported Outcomes
PATH Program Patient Reported Outcomes.
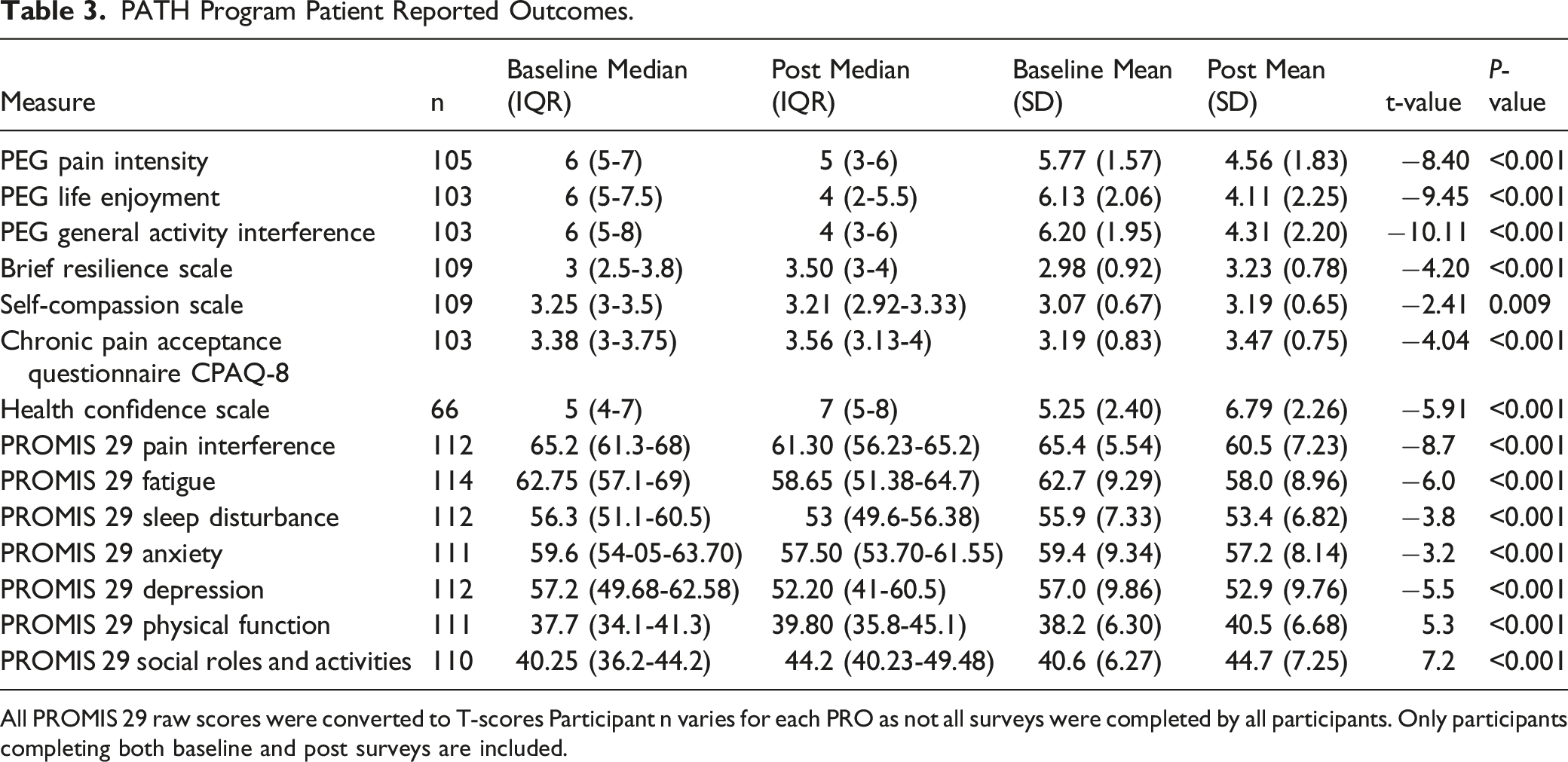
All PROMIS 29 raw scores were converted to T-scores Participant n varies for each PRO as not all surveys were completed by all participants. Only participants completing both baseline and post surveys are included.
Cost and Utilization Outcomes
120 total participants who completed at least half of the program and had coverage through BCBSVT for at least 6 months pre- and 6 months post-PATH, were included for the claims and utilization analysis.
The cost of care and utilization rates were tracked for 12 months pre-and post-study. Cohorts 1-13 all included data for 12 months post-PATH. Cohort 14 included 11 months of data post PATH, cohort 15 included 10 months of data post-PATH, cohort 16 included 8 months of data post-PATH, and cohort 17 included 6 months. Cohorts 18-20 all had less than 6 months of follow-up and are not included in this analysis.
PATH Program Pre- and Post-medical Costs and Utilization.

PMPM = per member per month.
All costs are means.
All values are means.
Discussion
The PATH program’s intention is to bring a coordinated and integrative, transdisciplinary approach to help people living with high impact chronic pain through an accessible and convenient clinic mixing group and individual medical and educational visits, and in-person and telehealth care, to best meet the needs of participants.
Participant Demographics
The PATH gender mix (76.4% female) is typical of an HICP population that uses integrative health.27,28 The gender difference in PATH participation may be due to differences in prevalence of HICP, and to females’ greater utilization of integrative health. A study using 2019 NHIS data indicates a 14.2% higher prevalence of chronic pain for females. 27 The prevalence of HICP in females is 8.5% and in males is 6.3%, indicating a 35% higher prevalence of HICP for females relative to males. 27 Analysis of the 2012 NHIS data finds that users of complementary and alternative medicine are 73% female (OR = 2.75). 28 The higher prevalence of using integrative health by females relative to males suggests that there may be attitude and belief differences affecting the use of integrative health care by men. As the evidence base increases demonstrating the effectiveness of integrative health care for conditions such as HICP, it will be important to understand what any attitudinal or belief barriers might be, and whether they can be eliminated. While we found studies that investigated preferences for users of integrative health care, 29 and some for medical students and doctors, 30 we did not find any high-quality studies of non-users that explored factors that might be involved in not using integrative care. This should be investigated in a study with more granularity for non-users.
The mean age of the PATH participants (49.8 years) is also typical of the HICP population in the US (low 50s). 2 The employment status, however, is not typical. In the US, 30.1% of those with HICP are employed 2 while 50% of the PATH participants are employed full-time, and 17% are employed part-time. This may influence the generalizability of our results. This difference should be investigated in future studies.
The NHIS data showed that increased age, decreasing level of education, and non-married status were associated with higher likelihood of the presence of chronic pain. 31 We did not evaluate these relationships as part of this pilot feasibility study, and should be included in future evaluations.
Participant Retention
This PATH study demonstrates high participant follow-through. Our 88.8% completion rate is similar to the highest retention rates reported in a systematic review of research of complementary and integrative health therapies for pain management. 9 Unlike the highest-performing program in the review, PATH did not include direct cash payments. However, the bundled payment structure may have incentivized some participants to persist in PATH because some integrative modalities and classes were covered that would not have been outside of the bundled payments.
Delivery Effects
Participants in the 16-week program were much more likely to complete the program than those in the 8-week program, increasing the effectiveness of PATH. Based on informal feedback from participants and providers, the relative effect size of longer duration cohorts was likely a result of greater ease in fitting the weekly time required for PATH into their life. This suggests that the PATH program should remain at 16 weeks.
Shifting program delivery from all in-person to virtual, and then to a hybrid of in-person and virtual, which allowed the participants to choose the format that works best for them, had the effect of increasing the PATH completion rate. Those in the virtual cohorts were more likely than those in the all in-person cohorts to complete PATH. Those in the hybrid cohorts were even more likely to complete PATH relative to the all in-person cohorts. The increase in PATH completion is likely a reflection of the ability to shift between formats as life circumstances change and suggests that PATH should continue using the hybrid format.
Self-Reported Outcomes
Results show consistent improvement in disability & function, pain reduction, self-compassion, resilience, acceptance and willingness to engage in activities despite pain, and increased confidence in ability to manage pain. As a single-arm study though, we can’t make definitive statements about causality, and these outcomes should be replicated in a controlled study.
Although we did not have a tool per se to measure the effectiveness of the group setting, we consistently heard feedback that being with others who share a chronic pain experience was incredibly validating and helped decrease the isolation that comes with having chronic pain and the mental health challenges stemming from or contributing to chronic pain. Being in a consistent cohort for 16 weeks enabled participants to develop a sense of community, trust, and support. The group format is foundational to our philosophy and approach to helping people improve their health and function. The results support the value of this interdisciplinary integrative approach, to both individuals and payers.
Value to Payers
Through claims analytics, our partner insurance company, Blue Cross Blue Shield of Vermont, showed improvements in overall and musculoskeletal-coded costs, and a very significant decrease in adverse health care utilization in the emergency room. Interventional procedure costs did increase by 6% over this period, which may suggest not an absolute increase in utilization but rather a more effective connection to the health care system and more appropriate use of these tools. These results appear to be consistent with one another and the utilization and financial outcomes which were studied for one year post intervention, suggesting that the program may have long-lasting, sustainable results, an important component of outcome studies. The PATH program maximizes the use of physical, psychological, and integrative pain treatments within a transdisciplinary model accessible to patients and is consistent with the CDC 2019 statement and call to action. 7 The preliminary results from this study show potential efficacy, enough so that BCBSVT is continuing to support participants through the bundled payments. The Department of Vermont Health Access, which administers Vermont’s Medicaid insurance program, has also agreed to a pilot program to assess PATH’s value to the state’s Medicaid population with high impact chronic pain.
Program Assessment
During the planning of PATH, consideration was given to what types of integrative practitioners were available in the area, which is a mid-size city. PATH was successful in being able to offer a wide variety of modalities. As the program expands to other locations, the mix of integrative offerings will likely need to adapt to the local availability of practitioners, especially in more rural areas.
PATH has completed 20 cohorts during the period of this study. While combining many group and individual visits, it had flexibility to shift as needed to address the feedback of the participants, as well as the safety protocols of the Covid pandemic.
The program’s financial model of support with Blue Cross Blue Shield of Vermont, which pays for care in a “bundle” format, includes the utilization of integrative health services not traditionally covered through Fee-For-Services insurance models.
Research should be undertaken to further explore the effectiveness of the PATH approach in a larger and more diverse population in multiple settings, and with an appropriate control group. Contributions could also be made in implementation research to learn how to best scale this program into multiple sites through a standard and reproducible approach. At the same time, we are exploring the creation of an extension of this program into primary care using a medical group visit model to sustain and support patients in their improvements and move from a tertiary prevention model to an integrated primary care model for many patients.
Limitations
The program showed resilience and flexibility with a focus on patient safety. For a period, due to Covid-19, participant and provider safety were prioritized and enrollment was briefly limited to a maximum of 6 people per group. PATH was completely virtual from March to September 2020. The later shift to a hybrid format allowed for the comparison of delivery methods.
This pilot study was completed with an initial intent to re-survey participants at 6 months post-intervention, but resources were unavailable to perform an additional assessment. The intent going forward is to expand our reach to study longer-term outcomes at both 6 and 12 months using the same outcome measures. In addition, the clinical measures we administer at intake (e.g., social determinants and mental health screening) could be included in a follow-up assessment as other data points to compare pre- and post-treatment as well as between group variations within a more comprehensive study with controls. Analysis of utilization data should be expanded rather than relying predominately on cost data in future studies.
The PATH participant demographics are consistent with those of our region (Northern Vermont and New York) and do not reflect the racial and ethnic diversity of the United States as a whole. It is established that non-Hispanic Black adults and Hispanic adults are more likely to experience chronic pain than non-Hispanic white adults, 31 and because they are represented in our program proportionate to the local population, they are therefore underrepresented in this sample as compared to other areas of the United States. Future multi-site studies should be conducted to represent the diversity of the US more closely.
Related to language access, CPP is developing a way to include simultaneous interpreter services that would enable people for whom English is not their first language to join the group portion of the PATH program. Thus far, the program was modified to create an “Individual PATH” program for people whose primary language is not English. The individual track provides access with interpreters to all the integrative therapies, and they receive information provided in the primary curriculum during one-on-one sessions with providers who are also group facilitators. This Individual PATH program has also been made available to people who may benefit more from an individual approach (i.e., people who are neuro-diverse or have other individual reasons why they would have challenges succeeding in a group setting).
A person’s health care regimen and needs can be as unique as each person, given the complexity of high impact chronic pain. Each participant was encouraged to try a variety of therapies and determine for themselves what seemed to make a difference. This sampling would then help them decide how to prioritize and/or combine integrative therapies post-graduation as a long-term approach to pain management.
While all outcomes showed statistically significant improvements, this was a single-arm study and some measures with small effect size may not be clinically significant. Minimal Clinically Important Difference (MCID) is an estimate of how much change is required for a patient to think it is significant. For PROs the MCID may vary depending on the baseline pain level and type of pain, and the PATH program includes patients with a range of pain types. For the PROMIS scale scores, for example, MCID has been estimated to be a change in T-score of 5, which is 1/2 standard deviation. We did not evaluate MCID in this study, but it should be determined in future studies to help assess the value of all findings.
As this was primarily conducted as a feasibility study, confounding factors such as type of chronic pain or type of pharmacologic medications were not examined. This will be addressed in future studies.
A strength of this study is the inclusion of all types of high impact chronic pain, a broad diversity of integrative therapies, a mix of group and individual education and treatment, and possibly indirect incentives for participation. Most of these are included as study design recommendations of the systematic review mentioned above. 9
Generalizability
Many factors affect the generalizability of the findings of this study. The mean age of participants is typical of the HICP population in the US. The race/ethnicity of 98% non-Hispanic white is typical of northern Vermont but not of the US in general and may impact generalizability. 67% of the participants were employed at least part-time vs only 30.1% of those with HICP in the US are employed. 2 PATH is a pragmatic program and includes all types of high impact chronic pain as would be seen in most clinics, increasing generalizability.
Comparison with Similar Pain Management Programs
There are many multidisciplinary integrative chronic pain management programs, but two that are close to PATH are the Whole Health model of care at the Veterans Health Administration (VHA) and the Osher Center for Integrative Medicine at Harvard Medical School. Both have published multiple pain studies. We are not comparing outcomes because this study did not have a comparison group., There are a few major differences between the programs that might impact effectiveness. PATH is only for those diagnosed with high impact chronic pain, while Harvard and VHA work with anyone with chronic pain. This could be a confounder, as the HICP population has a more complex presentation. 11 PATH has group education and medical visits which helps grow group cohesion, which might also be a confounder. PATH has 1 location for all services and is set up to encourage provider interaction and team meetings to discuss patient care in a transdisciplinary manner.
Conclusion
With the changes made to the PATH program format during the first 20 cohorts, this study of the 16-week integrative PATH Program at UVMMC’s Comprehensive Pain Program suggests effectiveness in relation to short-term patient-reported clinical outcomes and appears to show signs of durability in both utilization and financial outcomes up to 12 months following the program. Future studies are recommended that would expand the study population to better represent the US demographics. They should also be structured to include a usual care comparison group.
Supplemental Material
Supplemental Material - Overview and Feasibility of a Novel Transdisciplinary Integrative Approach to High Impact Chronic Pain in Vermont
Supplemental Material for Overview and Feasibility of a Novel Transdisciplinary Integrative Approach to High Impact Chronic Pain in Vermont by Joshua Plavin, Jerry Landau, Gail L. Rose, Erika Ziller, Sarah Nowak, Heather Finley, Laurel Audy, and Jon Porter in Global Advances in Integrative Medicine and Health.
Supplemental Material
Supplemental Material - Overview and Feasibility of a Novel Transdisciplinary Integrative Approach to High Impact Chronic Pain in Vermont
Supplemental Material for Overview and Feasibility of a Novel Transdisciplinary Integrative Approach to High Impact Chronic Pain in Vermont by Joshua Plavin, Jerry Landau, Gail L. Rose, Erika Ziller, Sarah Nowak, Heather Finley, Laurel Audy, and Jon Porter in Global Advances in Integrative Medicine and Health.
Footnotes
Author’s Note
Josh Plavin works for BlueCross BlueShield of Vermont as a per diem Medical Director.
Acknowledgements
We are grateful to Cara Feldman-Hunt and the staff at the Osher Center for Integrative Health at UVM, and the staff, practitioners, and patient advisors at the Comprehensive Pain Program for supporting the design, development, and operations of the CPP, and for championing our research efforts.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors acknowledge financial support for this work from Whole Health in the States, the Osher Center for Integrative Health at UVM, and University of Vermont Health Network. Partial support for JP time was funded by the Larner College of Medicine. Heather Amatulli at Blue Cross Blue Shield of Vermont contributed to data analysis.
Disclosures
Many of our contracted integrative therapists also have private practices, and may benefit financially if participants choose to continue working with them after the program is complete. We also see this as a potential benefit for continuity of care that remains completely within the participant’s control to seek out and invest if they find it beneficial.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.