
Abstract
Objective
Veterans Healthcare Administration (VHA) conducted a large demonstration project of a holistic Whole Health approach to care in 18 medical centers, which included making complementary and integrative health (CIH) therapies more widely available. This evaluation examines patterns of service use among Veterans with chronic pain, comparing those with and without PTSD.
Methods
We assessed the use of Whole Health services in a cohort of Veterans with co-occurring chronic pain and PTSD (n = 1698; 28.9%), comparing them to Veterans with chronic musculoskeletal pain only (n = 4170; 71.1%). Data was gathered from VA electronic medical records and survey self-report. Whole Health services were divided into Core Whole Health services (e.g., Whole Health coaching) and CIH services (e.g., yoga). Logistic regression was used to determine whether Veterans with co-occurring chronic pain and PTSD utilized more Whole Health services compared to Veterans with chronic pain but without PTSD.
Results
A total of 40.1% of Veterans with chronic pain and PTSD utilized Core Whole Health services and 53.2% utilized CIH therapies, compared to 28.3% and 40.0%, respectively, for Veterans with only chronic pain. Adjusting for demographics and additional comorbidities, Veterans with comorbid chronic pain and PTSD were 1.24 (95% CI: 1.12, 1.35, P ≤ .001) times more likely than Veterans with chronic pain only to use Core Whole Health services, and 1.23 (95% CI: 1.14, 1.31, P ≤ .001) times more likely to use CIH therapies. Survey results also showed high interest levels in Core Whole Health services and CIH therapies among Veterans who were not already using these services.
Conclusion
Early implementation efforts in VHA led to high rates of use of Core Whole Health and CIH therapy use among Veterans with co-occurring chronic pain and PTSD. Future assessments should examine how well these additional services are meeting the needs of Veterans in both groups.
Chronic musculoskeletal pain, defined as having recurring pain for at least 3 months, affects nearly 50% of the Veteran population.1,2 A large portion of Veterans with chronic pain (up to 50% in specialty clinics) may also experience significant symptoms of posttraumatic stress disorder (PTSD).3,4 The chronic pain and PTSD comorbidity is particularly complex, and linked to higher levels of pain disability, pain severity, anxiety, depression, sleep problems, as well as lower levels of mood, pain self-efficacy, and functioning.3,5,6 Importantly, co-occurring PTSD is also linked to more opioid use. 7
One component of the 2016 Comprehensive Addiction and Recovery Act (CARA), which aimed to address the nation’s opioid epidemic, was Veterans Healthcare Administration’s (VHA) large-scale demonstration project of the Whole Health System of Care. In this demonstration project, 18 Veterans Integrated Service Networks identified and funded a flagship VA medical center within their respective network for a 3-year Whole Health pilot. 8 The VA’s Whole Health approach to care has 3 components 1) The Pathway: peer-led educational efforts to help Veterans identify goals, preferences and priorities in areas such as physical health, spiritual health, and social health; 2) Well-Being Programs: well-being services (e.g., group classes focused on pain) and CIH treatments (e.g., yoga, mindfulness, and acupuncture); and 3) Whole Health Clinical Care: Whole Health coaching and engaging Veterans in care that ensures Veterans’ personal health goals are part of treatment. 8
The 18 VA flagship sites were granted a wide range of flexibility in how they proceeded with Whole Health implementation. Implementation strategies took place at both the system level and individual level, including disseminating Whole Health workbooks and intervention guides for providers to use with Veterans, training Whole Health coaches, and disseminating educational materials so that employees and Veterans could learn more about the Whole Health approach to care.8,9 Allocation of space and the ability to hire staff that would focus on Whole Health care were also components of implementation. In combination, efforts were designed to alter the culture of care to focus on the whole person, patient-specific values, and be patient-centered. 8
Among other priorities, the CARA funding emphasized expanding access to CIH therapies as non-pharmacologic approaches to pain management. This is particularly important for Veterans with complex symptom profiles, such as those with co-occurring chronic pain and PTSD. Non-pharmacologic approaches often target psychological and physiological factors that may help improve symptoms across many comorbid conditions simultaneously (i.e., transdiagnostic factors).10,11 Therefore, it is imperative to ensure that implementation efforts reach patients that are at risk for multiple conditions.
The aim of the present manuscript is to examine whether Veterans with comorbid chronic pain and PTSD utilize the Whole Health model of care, including Core Whole Health services and CIH therapies, to the same degree as Veterans with chronic pain but without PTSD. Assessing whether Veterans with comorbid chronic pain and PTSD are utilizing Whole Health services to the same extent as Veterans without PTSD would help determine whether implementation efforts are meeting this goal. Moreover, information gleaned from such an examination would inform future implementation efforts.
Methods
Participants and Procedure
The data for this analysis is from a congressionally mandated evaluation of the Whole Health demonstration project conducted in partnership with the Office of Patient Centered Care and Cultural Transformation (OPCC&CT), and as part of a Quality Enhancement Research Initiative (QUERI) evaluation. This evaluation was conducted as a quality improvement activity in accordance with VA Handbook 1058.05 and Program Guide 1200.21. The evaluation focused on assessing Whole Health implementation across the 18 VA flagship sites, how successful the pilot medical centers were in reaching Veterans, and how successful the pilot medical centers were in improving patient outcomes associated with Whole Health use, including reductions in opioid use and improvement in physical and mental health outcomes.
Study Sample
For the present study, we identified Veterans from the 18 flagship medical centers who had a primary care, mental health, or pain clinic visit who were regular VA users.12,13 Regular VA users were defined as having been assigned a Patient Aligned Care Team (PACT). 14 Exclusion criteria included age 90 or older, serious mental illness, and having an inpatient visit within 30 days of their most-recent visit. An initial sampling phase identified a random sample of regular VA users with an existing diagnosis of chronic musculoskeletal pain as implementation was just beginning. A second sampling phase, as implementation was ramping up, identified regular VA users with recent utilization coded with stop code 139, an early coding approach for Whole Health services. The objective of this phase was to identify a higher proportion of Veterans using Whole Health services. Veterans were approached for the survey using a tailored administration method. 15 Veterans were sent an introductory invitation letter, then sent an initial survey (including a $5 gift card), and if they did not reply were sent a reminder postcard, and a second copy of the survey. Veterans were informed that participation was voluntary and given the option to opt-out by phoning the project manager.
Combining both sampling strategies, a total of 9689 Veterans returned valid surveys of the 19,790 who were invited (49.0% response rate). For this analysis, 2 separate groups were created. The chronic pain group required at least two pain diagnoses at least 90 days apart over the prior year to the baseline survey, in addition to at least one moderate numeric rating scale (≥4) over the prior year to the baseline survey (n=4170). The comorbid chronic pain and PTSD group (i.e., comorbid group) included the same chronic pain diagnostic criteria, and, in addition, an ICD-10 diagnosis code of PTSD over the prior year (n = 1698).
Whole Health and CIH Use
We used VA electronic medical record (EMR) data to identify utilization of Core Whole Health services (defined as Whole Health pathway, coaching, and education), chiropractic care, and 8 CIH therapies encompassed in the standard VA medical benefits package 16 (acupuncture, therapeutic massage, biofeedback, guided imagery, clinical hypnosis, meditation, yoga, and Tai Chi/Qi gong) delivered by the VA and in the community (but paid for by the VA). In the current study, chiropractic care is included as a CIH therapy, although this service is considered a medical care. We used CPT codes (for chiropractic care, acupuncture, biofeedback, hypnosis, and massage only), clinic stop code 436 for chiropractic care, and newly created CHAR4 codes and health factors designed by VA. In addition, we developed search terms based on guidance from OPCC&CT and feedback from subject matter experts to search for Whole Health and CIH therapies using clinic location names and clinic note titles. To avoid double counting services identified by different coding strategies on the same day, we collapsed concurrent episodes of care among the 10 types of care. For example, if we found 1 or more CPT codes for acupuncture, a note title for acupuncture and a CHAR4 code for acupuncture on the same day, this was coded only as a single acupuncture encounter.
To assess overall use of Whole Health services and CIH therapies during the evaluation period, we examined a summary measure of Core Whole Health, and a summary measure of any CIH therapy based on services in the 12-month period prior to the return date of the baseline survey. The EMR data were then augmented with Veterans’ self-reported utilization of therapies from the survey. Veterans indicated in the survey if they were currently using or interested in using 2 types of Whole Health services (coaching and group) and 8 complementary and integrative health therapies (i.e., acupuncture, massage, chiropractic, hypnosis, guided imagery, meditation, yoga, and tai chi or qi gong). We created the 2 items about Whole Health (groups and coaching) to capture what Veterans may be familiar with or have an intuitive understanding about regarding interest if they had not heard about these services before. We did not ask about all possible Whole Health services being offered because sites were early in developing names of the specific services being offered. Use and interest in biofeedback was also not asked in the survey, because at the time of the survey this therapy was not yet being regularly offered at VA. Veterans could choose “not at all interested,” “somewhat interested,” “very interested,” or “already using” (either “In VA” or “out of VA”). If a Veteran indicated in the survey they were currently using a CIH therapy, but this was not found in the EMR, the participant was coded as using that service. The survey item for acupuncture did not differentiate between traditional acupuncture and battlefield acupuncture for VA use; however, the EMR was differentiated between the 2 types of acupuncture. Because it was unlikely that Veterans had received battlefield acupuncture outside of the VA, survey-reported community acupuncture (out of VA) was designated as traditional acupuncture use. However, because we could not determine whether survey-reported VA use of acupuncture was traditional or battlefield, this data was not included in the use count.
Summary variables for using each service thus included the combination of use identified in the EMR in the 12-month period prior to return of the baseline survey or indication of currently using in the baseline survey. Percentages for interest in Whole Health services are presented in 2 ways: percentage of interest among the entire sample, and percentage of interest among Veterans who have not used the Core Whole Health service or CIH therapy.
Measures
Demographics
Veterans provided basic demographic information on the survey, including marital status, education, combat experience, ethnicity, and race. Age, gender, urban or rural status, and drive distance to the nearest VA facility were gathered from the Veteran’s electronic medical record.
Pain and Chronic Conditions
Pain severity was assessed using the pain intensity, interference with enjoyment of life, and interference with general activity scale (PEG), 17 a three-item measure that assesses pain severity and interference, and the Defense and Veterans Pain Rating Scale (DVPRS), 18 a one-item assessment asking Veterans to rate their pain over the last 24 hours on a 0–10 scale. Each number is accompanied by a facial expression representing level of pain and a brief description ranging from “no pain” (0) to “as bad as it could be, nothing else matters” (10). The measure indicates that mild pain is represented by endorsing 1–4; moderate pain is represented by endorsing 5–6; and severe pain is represented by 7–10. Patient comorbidities were assigned via ICD-10 codes and modeled after the Elixhauser comorbidity index. 19 The count of total comorbidity variable was created by summing the number of comorbidities a patient had listed (a total of 31 possible comorbidities) in the EMR. Body mass index (BMI) was calculated using data from the EMR. Pain chronicity was assessed using survey data. ICD-10 codes were used to determine whether Veterans had a diagnosis of anxiety or depression.
Data Analysis Strategy
Global Advances in Health and Medicine.–

Note. SD = standard deviation; SMD = standardized mean difference; PEG: pain, enjoyment, general activity; DVPRS: Defense and Veterans Pain Rating Scale; BMI: body mass index.
Results
Descriptive Statistics
The chronic pain group (M = 64.7; SD = 11.2) was older than the comorbid chronic pain and PTSD group (M = 60.7; SD = 12.3) and included fewer women Veterans (12.4% v. 18.0%). A greater proportion of Veterans in the comorbid group endorsed military service that included combat (73.7% v. 40.2%). Frequencies regarding being married or in a civil union were 55.9% for the chronic pain group and 60.2% for the comorbid group). Frequencies for ethnicity were 7.6% Hispanic/Latino/a for the chronic pain group and 8.0% for the comorbid group. Most Veterans were White (73.5% for chronic pain group and 71.7% for comorbid group). See Table 1 for all demographic and clinical characteristics differences across the groups.
Veterans in both groups endorsed significant levels of pain in the past 24 hours, as assessed by the DVPRS. Veterans in the chronic pain group had high rates of either moderate (41.1%) or severe pain (45.9%), as did Veterans in the comorbid group (37.9% moderate pain, 52.7% severe pain). Both the chronic pain group (70.5%) and comorbid group (79.8%) reported high rates of problematic pain lasting more than 5 years. Veterans in the comorbid group endorsed more comorbidities as assessed by the Elixhauser index (M = 3.3; SD = 2.0) compared to the chronic pain group (M = 3.1; SD = 2.1). Veterans in the comorbid group also had higher rates of depression (55.0% v. 22.6%) and anxiety (30.9% v. 15.9%).
Interest in Whole Health Services Among Veterans Not Currently Using Whole Health.
Veteran Interest in Whole Health Services.

Note. Collapsed across both groups; *electronic medical record use of WH group, WH coach, and healing touch not included.
Interest in Whole Health Interventions and Approaches by Group.

Note. *electronic medical record use of WH service not included in “already using.”
Whole Health Services Use
Unadjusted models showed Veterans in the comorbid group were 1.42 (95% CI: 1.32; 1.52, P ≤ .001) times more likely (40.1% v. 28.3%) to use Core Whole Health services and 1.33 (95% CI: 1.26, 1.40, P ≤ .001) times more likely (53.2% v. 40.0%) to use any CIH intervention, compared to the chronic pain group. Unadjusted models consistently showed that the comorbid group was more likely to use any of the CIH therapies compared to the chronic pain group, with significant unadjusted risks ratios ranging from 1.23 (95% CI: 1.02, 1.47, P = .032) for battlefield acupuncture (9.0% v. 7.3%) to 2.38 (95% CI: 1.45, 3.89, P = .001) for biofeedback (1.8% v. .7%).
Differences in Whole Health Utilization Across Conditions.
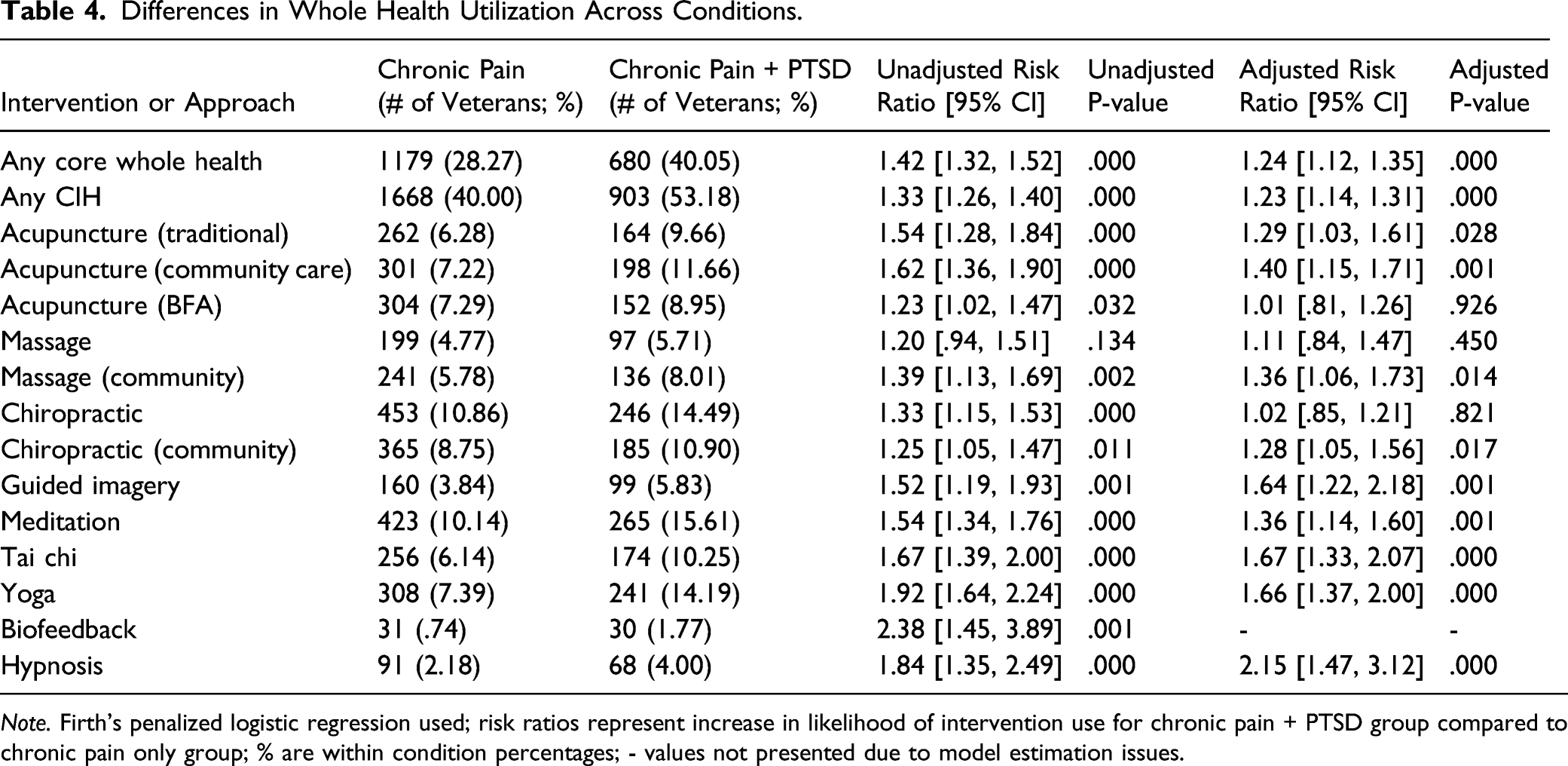
Note. Firth’s penalized logistic regression used; risk ratios represent increase in likelihood of intervention use for chronic pain + PTSD group compared to chronic pain only group; % are within condition percentages; - values not presented due to model estimation issues.
Discussion
The present study showed that Veterans with co-occurring chronic pain and PTSD consistently utilized more Core Whole Health services and CIH therapies compared to Veterans with chronic pain but without PTSD. Unadjusted models showed that significant differences existed across all services, except for massage. Controlling for demographics, pain severity, physical health, and mental health, these differences persisted for Core Whole Health Service use, any CIH intervention use, traditional acupuncture, community acupuncture, community massage, community chiropractic, guided imagery, meditation, tai chi, yoga, and hypnosis. Interest was also high across all services if Veterans were not already using them, highlighting that Veterans with chronic pain, with or without PTSD, are enthusiastic about utilizing these services. VA has placed a significant amount of resources into ensuring that Whole Health and CIH therapies are implemented system-wide.8,21 The present study highlights the degree to which these efforts are reaching Veterans with complex symptom presentations.
Prior published work indicated that about half of surveyed Veterans have used CIH therapies in the prior year, 22 which is consistent with our overall sample. However, results from the present study showed lower use, 40%, for Veterans in the chronic pain group. Whereas Taylor and colleagues 22 used detailed self-report, we combined less-detailed self-report information without specific timeframes with EMR data; this may account for the discrepancy. The discrepancy could also be explained by Taylor et al. 22 asking Veterans about more CIH therapies and using a Veterans Insight Panel, which is a voluntary panel of Veterans who have agreed to comment on VA activities. Although our study used a sampling technique based on VA use, the Veterans Insight Panel is an added level of VA involvement, which may have resulted in higher levels of utilization.
Consistently higher use among Veterans in the comorbid group is congruent with a recent meta-analysis showing greater frequency of healthcare use among Veterans with co-occurring chronic pain and PTSD compared to those with pain but without PTSD. 3 Importantly, higher use in the present study remained significant even after controlling for comorbid physical and mental health conditions, which points to a unique contribution of PTSD. Results also suggest that Whole Health services may be an efficient way to reach complex Veteran populations in a way which more traditional approaches struggle to do. Indeed, results of the present study could be explained by Veterans’ desire to reduce PTSD symptoms, and the search for effective treatment. Core Whole Health services provide patients with opportunities to set their personal health goals and choose treatments aligned with those goals, thereby increasing engagement with healthcare and self-care. The VA Whole Health approach is personalized and ensures that the focus of treatment remains on goals important to the Veteran. This approach may be particularly appealing to patients with PTSD for whom treatment is often highly prescribed and inflexible. Veterans are aware that VA offers certain standardized treatments for PTSD, and it is likely they have communicated with other Veterans around what those treatments may entail. Pre-conceived notions about more conventional treatments, despite their efficacy, may result in Veterans wanting to try something new and different. At the same time, Whole Health services and CIH therapies often do not confront PTSD directly, and the choice of using these services may represent an act of avoidance of the trauma. Because research indicates that PTSD is linked to more pain severity and disability, 3 greater use of Whole Health and CIH interventions may represent Veterans’ attempts at improving their pain symptoms. Future work should focus on understanding patient choice and how treatment choice (or perceived lack thereof) relates to engagement in care and clinical outcomes.
Although Whole Health and CIH use was consistently higher among Veterans with comorbid chronic pain and PTSD, rates of use were low for some therapies. For instance, only 5.8% of Veterans in the comorbid group, and 3.8% of Veterans in the chronic pain group used guided imagery during the prior year. These low rates likely correspond to the limited availability of guided imagery in VA and through community referral during the study period. These rates of use contrast with 33.1% of Veterans stating they were “Somewhat Interested” and 21.5% stating they were “Very Interested” in using guided imagery among those with no prior year guided imagery use. Prior research also shows interest in CIH approaches is high: among Veterans, 84% indicated an interest in at least 1 CIH approach, with pain, stress/relaxation, and overall health and well-being as the most cited reasons for seeking these approaches. 22 Similar results were seen in a VA primary care setting. 23 Other than improvement in symptoms and well-being, Veterans are particularly attracted to CIH therapies because of their focus on holistic approaches and spirituality/existential concerns, and autonomy around decision-making processes. 24 Removal of negative symptoms (e.g., anxiety) was only part of Veterans’ interest, as positive emotions, such as “joy” and “bliss” were also important. 24 The large discrepancy between rates of interest and rates of use in the present study points to a potential treatment gap among Veterans with chronic pain and/or PTSD.
Of note, we found that the comorbid group had significantly higher rates of combat experience, anxiety, and depression. Biofeedback, tai chi, yoga, acupuncture, mindfulness, and massage may all be valuable resources in pain improvement.25-30 Meditation, yoga, biofeedback, and mindfulness-based stress reduction help improve PTSD symptoms.31-37 Improved pain and PTSD symptoms in these trials suggest a focus on CIH therapies holds promise in treating the complexity of comorbid chronic pain and PTSD. The effects of pain and PTSD are often not confined to pain severity and characteristic PTSD symptoms (e.g., hypervigilance). Separately, these disorders are associated with negative changes in social relationships, sense of purpose, identity, and spiritual concerns.38-45 Core WH services may have a particular impact on issues surrounding personal meaning and purpose, setting personal health goals, and focusing on issues that are typically not medically focused. Thus, holistic approaches to care, either as stand-alone treatments or in adjunct with more conventional treatments, may offer particular advantages and benefits for many patients. Whole Health implementation efforts are ongoing, and the present study suggests that continued outreach efforts and Core Whole Health service and CIH therapy availability should both be improved to fully transition VA into using a Whole Health model of care.
Other clinical implications are related to clinical triage and recommendations when patients present with chronic pain or PTSD. Clinic leadership may have varied opinions on whether CIH interventions are effective, which may or may not be a barrier toward implementation. 46 Moreover, clinicians often must weigh available clinic resources with patient symptom severity and patient choice. By highlighting that patients will use these therapies if they are offered, the present data may encourage other healthcare settings and clinics to continue to expand their availability as these data demonstrate “If it is built, they will come.” In turn, engagement in these treatments can potentially improve targeted outcomes. Indeed, VA guidelines for lower back pain and PTSD focus on patient preference as an important component of clinical decision-making.47,48
Limitations and Future Directions
The study has limited generalizability to populations outside of VA and health systems without robust efforts to include alternatives to conventional care. It is important that similar research is conducted outside of VA that includes non-Veteran populations and beneficiaries of private insurance, Medicare, and Medicaid. The second phase’s sampling strategy was designed to reach Veterans who had used Whole Health services, potentially biasing the sample to include Veterans who were more likely to use Core Whole Health services and CIH therapies. The average age of our sample was 63.5 (SD = 11.7), and it will be important to determine whether results differ with younger or older Veterans/individuals. Although we attempted to match interest and use variables according to the Whole Health service, some were not congruent. For instance, our survey only captured Whole Health directly linked to Whole Health coach or Whole Health group interest. Similarly, we chose to use binary outcome variables and not levels of use or dose. Therefore, more detailed understanding of utilization patterns of these services and therapies could provide other useful information. The present work focused on interest and use only, whereas it will be important to determine whether use and interest are associated with patient-reported outcomes and other outcomes linked via electronic health records, including cost effectiveness outcomes.
It is important to note that delivery of these services across VA sites varies widely. Veterans may have received these services because of general interest, word of mouth, guidance from friends or peers, advertising about their availability, through referrals from primary care, rehabilitation, mental health, specialty pain clinics, or seeking care outside the VA. Moreover, mental health providers (e.g., psychologists), nurse care managers, and intervention specialists all play a role in how these services are delivered. Thus, examining pathways of accessing Whole Health services and how these pathways may affect use and outcomes could greatly inform implementation efforts and how to optimize clinical effectiveness of these interventions. Finally, our population of interest was co-occurring chronic pain and PTSD. However, it would be beneficial if future studies examine other populations (e.g., co-occurring chronic pain and depression) to determine whether similar results are found and what may account for any discrepancies. Moreover, future studies should examine certain populations in comparison to healthy controls.
Conclusions
VA is moving toward a model of care designed to more holistically and collaboratively improve Veteran health. The Whole Health model of care focuses on well-being through education, well-being classes, CIH therapies, and Whole Health coaching. The present study showed that Veterans with chronic pain and co-occurring chronic pain and PTSD are interested in Core Whole Health services and CIH therapies. This study also showed how VA efforts to target all Veterans may be working, as Veterans with co-occurring chronic pain and PTSD are more likely to use Core Whole Health services and a variety of CIH therapies compared to Veterans without PTSD. Future research should examine how well these additional services are meeting the needs of Veterans in both groups and Whole Health’s role in improving patient outcomes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article: This evaluation was supported by the Department of Veterans Affairs: Office of Patient-Centered Care and Cultural Transformation and Health Services Research and Development Service, Quality Enhancement Research Initiative (PEC-3-001).
Author’s Note
The views in this paper are the view of the authors and do not represent the views of the Department of Veterans Affairs or the U.S. Government.