
Abstract
Background
Individuals with posttraumatic stress disorder
Objective
Assess whether comorbid PTSD moderates Veterans’ response to yoga and/or cognitive behavioral therapy (CBT) for pain.
Methods
Veterans with Gulf War illness (n = 75) were assessed using the Brief Pain Inventory at baseline and posttreatment as part of a randomized clinical trial. PTSD status was abstracted from participants’ medical records.
Results
PTSD+ participants (n = 41) reported more pain at baseline than PTSD− participants (n = 34; d = .66, p < .01). PTSD+ participants experienced more improvement in pain from baseline to posttreatment than PTSD− participants by a small to moderate, marginally statistically significant amount (d = .39, p = .07). The relationship between PTSD and treatment outcome was not moderated by treatment type (yoga vs CBT; p = .99). Observation of treatment responses across PTSD status (+ vs −) and treatment (yoga vs CBT) revealed that PTSD+ participants responded well to yoga.
Conclusion
PTSD is not associated with reduced effectiveness of behavioral chronic pain treatment among Veterans with Gulf War illness. Therefore behavioral pain treatment should be made readily available to Veterans with pain and PTSD. Yoga deserves further consideration as a treatment for pain among individuals with PTSD.
Chronic pain and posttraumatic stress disorder (PTSD) frequently cooccur. 1 Theorists have argued that the presence of PTSD may complicate pain treatment as PTSD may prompt avoidant pain coping strategies that prevent treatment engagement, trauma reminders may trigger or exacerbate pain, and care for the comorbid conditions may require more coordination than is often available.2-4 We assessed whether PTSD was associated with different outcomes in behavioral pain treatment via secondary analyses of a randomized clinical trial. The trial compared yoga to cognitive behavioral therapy (CBT) among Veterans with Gulf War illness (GWI).
Many Veterans who served in the 1990–1991 Gulf War subsequently developed a constellation of chronic symptoms that could not be explained by known medical diagnoses. Symptoms included chronic pain, fatigue, and cognitive impairment. This condition was termed Gulf War illness.5-7 Little is known about the etiology and effective treatment of this condition. 8
Veterans of the Gulf War appear to have an increased risk for several other long-term health conditions including PTSD. 9 An epidemiological survey indicated that 44% of Gulf War Veterans reported symptoms indicative of GWI and 21% of PTSD. 10 A smaller study found that 35% of Veterans with GWI met criteria for PTSD as opposed to only 3% of Gulf War Veterans without GWI. 11 Relatedly, a large (n = 21 000) study of treatment-seeking Gulf War Veterans found that Veterans with PTSD reported more pain than Veterans without PTSD, even after accounting for wartime exposures and medical illnesses. 12
Similarly, PTSD frequently cooccurs with chronic pain. A systematic review of 19 studies reporting rates of PTSD among individuals with chronic pain and assessing for a statistical relationship between the two conditions revealed that 16 of the studies found evidence of association. 1 The association between pain and PTSD may be particularly relevant to Veterans as the average rate of PTSD among the four of these studies that used Veteran samples (50%) was higher than it was among all 19 samples combined (both Veteran and nonveteran; 19%). Another empirical analysis concluded that severe pain is “strikingly” more prevalent among Veterans than nonveterans. 13
Several studies suggest that PTSD is associated with differences in pain presentations, coping strategies, and course of treatment. Individuals with PTSD and chronic pain reported more pain and functional impairment than those with pain alone.2,14-16 Veterans with chronic pain and PTSD used more illness-focused coping strategies, such as “guarding” painful areas. 14 Finally, those with PTSD used more pain medication and utilized more pain-related medical services. 17
Theorists have argued that PTSD may complicate pain treatment in several ways.3,18 Maladaptive PTSD coping strategies such as avoidance and distrust may prevent engagement in pain treatment. PTSD may exacerbate pain symptoms, such as when an individual is reminded of a traumatic event and experiences pain in the location that was injured during the event. Conversely, pain may remind the individual of the traumatic event and trigger PTSD symptoms. Finally, the comorbid conditions may not be treated with adequate coordination of care between providers.
Despite these concerns and the high rates of comorbidity between chronic pain and PTSD, little is known about the effectiveness of treating pain among individuals who also have PTSD. A report of a Veterans Affairs consensus conference on treatment of comorbid chronic pain, PTSD, and/or traumatic brain injury stated “The consensus panel…was still left with the question of how useful are the current [individual disorder treatment] guidelines for treating the two or three disorders concurrently and how well can a Veteran with the comorbidities benefit from the evidence-based treatments.” The panel called for randomized clinical trials to address these questions. 4 One recent study compared outcomes in a clinical behavioral pain treatment, acceptance and commitment therapy, between PTSD+ and PTSD− patients and generally found equal outcomes. 16 The present study further addresses this need.
The Present Study
We evaluated the relationship between PTSD and behavioral pain treatment outcomes via secondary analyses of data from a randomized clinical trial comparing cognitive behavioral therapy (CBT) to yoga for pain among Veterans with GWI. 19 Analysis of primary outcomes from this dataset showed that participants assigned to yoga experienced a significantly greater decrease in pain as measured by the Brief Pain Inventory (BPI) total score than participants assigned to CBT. The between-group differences in the BPI’s pain severity and pain interference subscores were not statistically significant.19,20 In the present secondary study, we addressed the following questions: (1) Overall, did participants with PTSD report a different change in pain from baseline to posttreatment than participants without PTSD? and (2) Did this relationship between PTSD status and treatment outcome assessed in question #1 depend on treatment type (CBT vs yoga)? That is, did treatment type moderate the relationship between PTSD status and treatment outcome? For example, in the CBT group, participants with PTSD could have had worse outcomes than participants without PTSD, whereas in the yoga group, participants with PTSD could have had better outcomes than participants without PTSD.
Methods
Participants and Procedure
The clinical trial’s methods were described in detail previously in the report of the study’s primary outcomes. 21 Key points are reiterated here. Veterans of the Persian Gulf War with symptoms of GWI volunteered for a randomized, controlled study with two parallel treatments for pain at the Palo Alto Veterans Affairs Healthcare System. Study inclusion criteria included (1) enrolled in the armed forces between 1990 and 1991; (2) current chronic pain rated in the moderate to severe range on the Short-Form McGill Pain Questionnaire; and 22 (3) currently met case definition for GWI using the Fukuda et al. 5 symptom–category approach of having one or more chronic symptoms from at least two of the following three categories: musculoskeletal (eg, muscle pain and joint stiffness); mood-cognition (eg, difficulty concentrating, feeling moody, and difficulty finding words); and fatigue. A total of 75 participants were eligible and randomized to a treatment. Stanford University Institutional Review Board conducted ethical review and approved the protocol.
Interventions
Treatments were delivered to groups of ≤10 individuals in 10 weekly 60-minute sessions.
Yoga: The intervention was designed by the yoga instructors, the study’s physician, and its physical therapy collaborators. Classes were Hatha yoga style and incorporated yoga elements of controlled breathing, poses, and meditation. Each technique was selected for its potential to reduce chronic pain. Classes were taught by three different Yoga Alliance 200-hour certified instructors with training in different lineages of Hatha yoga. During the 10-week treatment phase, participants were instructed to perform 30 minutes of yoga “homework” on five non-study days per week.
Cognitive Behavioral Therapy: We used a modified version of a CBT protocol from a previous study 23 which targeted physical functioning in Veterans with GWI. The goals of the protocol were to teach behavioral skills to help participants experience a safe and gradual increase in physical functioning without exacerbating symptoms and to teach cognitive strategies to help participants learn systematic ways of modifying unhelpful beliefs and solving problems. Behavioral techniques included activity pacing, pleasant event scheduling, sleep enhancement, relaxation, and communication skills. Throughout the 10-week treatment phase, participants were instructed to practice the techniques on five non-class days. All study therapists were psychologists or psychological trainees with previous training in CBT.
Measures
Sociodemographic data were collected via self-report. Participants also completed a self-report checklist in which they identified medical conditions with which they have been diagnosed by a physician.
PTSD was not assessed in the clinical trial. In order to conduct the present secondary analysis, PTSD status was determined by abstraction from participants’ electronic VA medical records. The fields searched were problem list, compensation and pension claim adjudication note(s), treatment notes, and treatment discharge summary note(s). Medical records from both the study site’s catchment area and from national records were searched. Participants were coded PTSD+ if evidence of diagnosis was found in records dated less than 10 years prior to enrollment in the study. This procedure was similar to a procedure recently described as a “gold standard” for abstracting PTSD status from Veterans’ medical records. 24
Pain was assessed via the Brief Pain Inventory-Short Form (BPI-SF), 20 a self-report measure which was administered at baseline, during treatment (weeks 2, 4, 6, and 8) and at end of treatment (within a week of the tenth and final treatment session). The BPI-SF yields three summary scores: pain severity, pain interference, and total pain. Pain severity is an average of four pain ratings on a 0–10 scale (worst in last 24 hours, least in last 24 hours, on average, right now); pain interference is an average of nine items assessing how much pain interferes with nine daily activities (eg, general activity, mood, walking, and work) on a 0–10 scale; and total pain is an average of all 13 items.
GWI diagnostic status was determined using a self-report symptom scale of 34 symptoms used by Fukuda et al. 5 that were assessed on a none/mild/moderate/severe ordinal scale. Depression was measured via the interviewer-administered Hamilton 25 Depression Rating Scale (HAM-D).
Statistical Methods
We assessed the validity of the abstracted PTSD status variable in several ways. To assess predictive validity, we assessed how likely PTSD+ participants were to also show evidence of being PTSD+ in the same data fields at any date after enrollment in the study. Second, we evaluated convergent validity via comparisons to participants’ self-reports of having previously been diagnosed with PTSD. Third, we assessed convergent validity with participants’ self-report of symptoms that were not assessed in the context of PTSD assessment but nevertheless are difficulties that may reflect PTSD symptoms. Fourth, we evaluated criterion validity based on known associations between PTSD and depression and antidepressant use (certain selective serotonin reuptake inhibitors, a type of antidepressant medication, are first-line psychopharmacological agents for PTSD 26 ).
We employed linear mixed effects modeling27,28 to assess the relationship between PTSD status and treatment outcome and whether this relationship was moderated by treatment type using the MacArthur approach.29,30 We included all timepoints (baseline; weeks 2, 4, 6, 8; end of treatment) in the model. In line with the intention to treat principle, we included all randomized individuals in the analyses. To estimate our mixed effects model, we used maximum likelihood embedded in the Mplus program v8, 31 where it is assumed that data were missing at random conditional on observed information. 32 Specifically, we used a random intercept model assuming linear change over time. In the model, PTSD status (+ vs −), treatment type (CBT vs yoga), and the interaction between PTSD status and treatment type were the independent variables. Participants’ total pain score slope from baseline to end of treatment was the dependent variable. Following convention, alpha was set at .05 (two-tailed). Cohen’s d effect size estimates were computed using changes in model-estimated means and observed baseline standard deviation pooled across all participants.
Results
Demographics and Clinical Characteristics
Demographics and clinical characteristics.

PTSD = posttraumatic stress disorder; SD = standard deviation; BMI = body mass index; GWI = Gulf War illness
aDisabled = receiving disability benefits, irrespective of whether also employed, enrolled in school, etc.
bSelf-reported symptoms experienced subsequent to Gulf War and in three months prior to study.
cOut of a total of 7 cognitive symptoms reflecting Fukuda cognitive symptom criteria (concentration, memory, word finding difficulties, anxiety, depression, irritability, and feeling moody).
dDepression measured by the Hamilton Depression Rating Scale.
Validating PTSD Status
Forty-one participants (55%, 27 male, 14 female) were coded positive for PTSD and the remaining 34 (45%, 30 male, 4 female) participants were coded negative. As expected, 11 this exceeded the rate of PTSD among an epidemiological sample representative of all Gulf War Veterans (21%). 10 We evaluated predictive validity and found evidence of a PTSD diagnosis in the medical record after participation in the study for 38 of the 41 PTSD+ participants. Second, we evaluated convergent validity and found that participants coded as PTSD+ were far more likely to self-report having previously received a diagnosis of PTSD (85% vs 21%, p < .01). Third, we assessed convergent validity with participants’ self-report of symptoms that may reflect PTSD symptomology, namely, difficulty concentrating, difficulty sleeping, irritability, and anxiety. PTSD+ participants scored more highly on all of these measures (all p's < .01). Fourth, we evaluated criterion validity and found that PTSD+ participants also scored more highly on a measure of depression and were more likely to use antidepressant medication (ps < .01). Taken together, the PTSD status variable abstracted from medical records was likely a sufficiently valid indicator of participants’ true PTSD status to permit further analysis.
Pain Treatment Outcome
Pain treatment outcome by PTSD status and treatment.
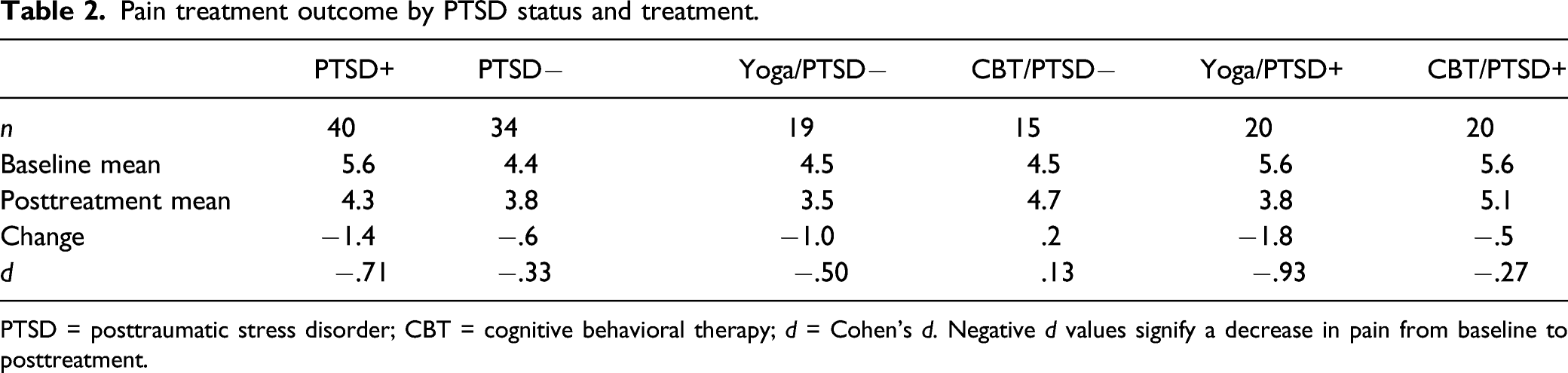
PTSD = posttraumatic stress disorder; CBT = cognitive behavioral therapy; d = Cohen’s d. Negative d values signify a decrease in pain from baseline to posttreatment.

Pain outcomes by PTSD status and treatment. Changes in model-estimated mean BPI total from baseline to end of treatment. (a) Trajectories for participants with PTSD (PTSD+) and participants without PTSD (PTSD−) and (b) trajectories by PTSD status (+ vs −) and treatment (yoga vs CBT). BPI = Brief Pain Inventory-Short Form; PTSD = posttraumatic stress disorder; CBT = cognitive behavioral therapy.
Treatment outcomes by PTSD status (+ vs −) and treatment (yoga vs CBT) are shown in Table 2 and Figure 1B. Participants with PTSD improved more than participants without PTSD in both the yoga group (d = −.93 vs d = −.50) and in the CBT group (d = −.27 vs d = .13). Therefore, the interaction between PTSD status and treatment type was not statistically significant (p = .99). This suggests that PTSD did not attenuate response to either treatment. Rather, the pattern of changes was best explained by additive effects of the marginally significant effect of PTSD status, with PTSD+ participants improving more than PTSD− participants, and the effect of treatment type reported previously, 21 with participants in the yoga condition improving more than participants in the CBT condition. As a result of these additive main effects, PTSD− participants in the CBT group improved the least, and the PTSD+ participants in the yoga group improved the most.
Discussion
Clinical theory predicts that pain treatment may be less effective among Veterans with PTSD than those without.3,18 However, there is little data describing the effectiveness of behavioral pain treatment among Veterans with PTSD, 4 despite high rates of comorbidity between these conditions. Therefore, we assessed the relationship between PTSD status and behavioral pain treatment outcome among Veterans with GWI via secondary analysis of a randomized clinical trial of yoga and CBT for pain. Contrary to our hypothesis, participants with PTSD did not improve less than PTSD− participants and in fact improved more by a small to moderate effect size which was marginally statistically significant.
This may be due to PTSD+ participants reporting more pain at baseline and therefore greater reversion to the mean at end of treatment. Alternatively, the results could be compromised by measurement error in the PTSD status variable. For example, a prior comparison of PTSD status ascertained via medical record abstraction to that determined by diagnostic interview among Veterans found that the two methods disagreed on 27% of cases. 33 Therefore, we evaluated the predictive, convergent, and criterion validity of the PTSD status variable in the present study and judged the results to be sufficient to allow further analysis. While it is possible that measurement error could have influenced the present results, it is unlikely that improved assessment of PTSD status would lead to the exact opposite conclusion—that PTSD+ Veterans improved less than PTSD− Veterans. Therefore, it is safe to conclude that PTSD+ Veterans benefitted no less than PTSD− Veterans.
A recent study of PTSD’s role in treatment of chronic pain via a single behavioral psychotherapy also found that PTSD generally did not moderate outcomes. 16 Taken with our findings, this suggests that PTSD is generally not associated with inferior behavioral pain treatment outcomes.
However, combined treatment of the two conditions may still be indicated, when available, for many of the reasons previously cited.3,18 These include reducing Veterans’ barriers to engaging in treatment and facilitating provider sensitivity to potentially complex interrelationships between Veterans’ pain and PTSD symptoms. The present study does not support, for example, delaying behavioral pain treatment until combined pain and PTSD treatment is available. Further research into the role each condition plays in the treatment of the other may be indicated as the causal processes may be complex. For example, one study indicated that pain may be associated with worse PTSD treatment outcome only if the pain is related to the event that led to the PTSD. 34
The relationship between PTSD status and treatment outcome did not differ by treatment type. That is, the interaction between PTSD status and treatment type was not significant as yoga appeared to be more effective than CBT for both the PTSD+ and PTSD− groups. Rather, outcomes were predicted by main effects of treatment type previously reported 21 and the marginally significant effect of PTSD status (reported in the present paper). As a result of these additive main effects, the group that improved the most was the PTSD+ individuals assigned to yoga. Yoga appears to be effective in treating PTSD as it exerted a medium to large effect size according to a meta-analysis of four randomized trials. 35 One explanation for these observations is that yoga exerts a beneficial effect on chronic pain and PTSD simultaneously. A non-specific effect of yoga on multiple health conditions has been previously noted.36,37 Therefore, it may be worth further evaluating yoga as a treatment for comorbid chronic pain and PTSD.
Strengths of the present study include its data being drawn from a randomized controlled trial and the clinical relevance of its findings. A limitation is that, as expected, PTSD+ participants reported more pain at baseline, and therefore, more of the gains in this group may have been due to reversion to the mean. Additional limitations include its moderate sample size and its determination of PTSD status via abstraction from medical records. Further, it is unknown to what extent these findings would generalize to populations beyond Veterans with GWI.
Conclusion
Despite clinical theory to the contrary, PTSD does not appear to decrease the effectiveness of behavioral pain treatment, at least among Veterans with GWI. Therefore, while integrated treatment may be desirable, these treatments should be made readily available to Veterans with symptoms of GWI, including pain, and PTSD. Yoga deserves consideration as a treatment for comorbid pain and PTSD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a CDMRP/DoD Gulf War illness Research Program Innovative Treatment Evaluation Award (#11488016).
Data Availability
Study data is available from the corresponding author upon reasonable request.