
Abstract
Muscle strength training for stroke patients is of vital importance for helping survivors to progressively restore muscle strength and improve the performance of their activities in daily living (ADL). An adaptive hierarchical therapy control framework which integrates the patient's real biomechanical state estimation with task-performance quantitative evaluation is proposed. Firstly, a high-level progressive resistive supervisory controller is designed to determine the resistive force base for each training session based on the patient's online task-performance evaluation. Then, a low-level adaptive resistive force triggered controller is presented to further regulate the interactive resistive force corresponding to the patient's real-time biomechanical state – characterized by the patient's bio-damping and bio-stiffness in the course of one training session, so that the patient is challenged in a moderate but engaging and motivating way. Finally, a therapeutic robot system using a Barrett WAM™ compliant manipulator is set up. We recruited eighteen inpatient and outpatient stroke participants who were randomly allocated in experimental (robot-aided) and control (conventional physical therapy) groups and enrolled for sixteen weeks of progressive resistance training. The preliminary results show that the proposed therapy control strategies can enhance the recovery of strength and motor control ability.
Keywords
1. Introduction
Patients suffering from strokes or spinal cord injuries require specific training to improve motor learning and recovery [1]. Conventionally, these therapy programmes are manually implemented by physical or occupational therapists. However, the efficacy of such therapist-centred therapy methods is often dependent on the therapist's experience and subjective judgment. Robotic-aided neurorehabilitation is becoming increasingly common in motor rehabilitation, because they are not only able to provide a variety of highly reproducible, repetitive movements and training protocols, but they are also able to offer objective measurements and an estimation of the patient's motor performance and functional improvement [2]. In recent years, several categories of therapy control strategies for robotic-aided rehabilitation training have been explored in some existing robot-assisted rehabilitation training systems, including impedance, admittance and EMG/EEG-based controllers, as well as force/haptic stimulation and other virtual reality-related control methods [3]-[6]. Although shown to be effective to some extent, most of these therapy control algorithms are focused on providing active-assisted exercises by designing a low-level controller, with only a few attempts being made to incorporate muscle strength training into robot-aided therapy[7][8]. Moreover, these robotic devices – including resistance-based training options – often apply constant resistive forces to the affected limb all the time. From motor learning and neurorehabilitation theories, it is known that the learning rate and rehabilitation outcome are maximal at a positively challenged task difficulty level [9]. With regard to the progressive resistance muscle strength training of stroke patients, an exerted resistive force that is too small for the subject will be perceived as boring and a force that is too large will overstress the subject; meanwhile an adaptive resistive force that adjusts in real-time to challenge the patient all the time should induce maximal engagement and optimal physical participation.
The provision of adaptive functional training corresponding to the patient's progress has been received much attention from rehabilitation robot researchers over the past few years. K. Kiguchi et al. [10] proposed an adaptive impedance controller for an upper limb rehabilitation robotic exoskeleton system where the desired impedance control parameters were regulated based on the EMG signals of human muscles. Experimental results based on healthy human subjects verify the effectiveness of the proposed adaptation scheme. Y. Choi et al. [11] presented a novel robotic adaptive and automatic presentation of tasks (ADAPT) which can adaptively present simulated ADL functional tasks, implement performance-based task scheduling and generate the desired trajectories for motor control based on learned models of task dynamics. M. Duff et al. [12] have successfully shown that an adaptive mixed reality rehabilitation system can provide customized reaching and grasping training for chronic stroke survivors based on the retention of goal completion and activity recovery conditions. One common aspect of the majority of these adaptive therapy control algorithms is that they mainly concentrate on the modification of controller parameters or task difficulty levels according to the patient's motor performance evaluation after one or more training sessions. Their focus is still on assistive exercises and, moreover, these adaptive therapy controllers are all developed within the framework of predefined trajectories and related task-performance motoring. Crucially, they do not offer an insight into the patient's real-time state estimation and monitoring.
The integration of the patient's real-time state into the control loop while making the system bio-cooperative has been shown to be crucial for motor learning and rehabilitation [13]. A robot-aided progressive resistance muscle strength training system that can provide moderate challenge-based resistive exercises in agreement with the patient's actual muscle force changes will be more effective than the one that does not. As a consequence, estimating the patient's real-time biomechanical state corresponding to his/her actual muscle force changes and integrating the estimated state into the resistive controller design – and thus providing progressive resistive force up to the limit of what the patient can do – may have a positive effect on the success of muscle strength recovery.
An adaptive hierarchical control framework that combines a high-level progressive resistive supervisory controller with a low-level adaptive resistive force triggered controller is proposed. The former is presented to implement performance-based resistive force base scheduling for each training session while the latter is designed to further regulate the interactive resistive force in agreement with the patient's real-time biomechanical state during one training session. To verify the clinical efficacy of the hierarchical therapy controller, the stroke participants were allocated to robot and conventional groups and participated in a 16-week session of robot-aided or conventional physical therapy, respectively. The remainder of this paper is organized as follows: Section 2 presents the hierarchical controller design, the experimental setup and the clinical training protocols. In Section 3 and 4, the details of the results and discussions about the motion control and the rehabilitation evaluation of the proposed therapy control algorithm on the two groups of recruited stroke patients are presented.
2. Methods
2.1 Subjects
Stroke patients with upper extremity motor impairments, aged 55 years and above, 6 months to 2 years after a single mild to moderate stroke, were recruited as representative participants. Participants were excluded from the study if they had epilepsy, severe neurological disorder or serious psychological or cognitive impairment [14]. Subjects were also excluded if they were incapable of overcoming their own arm gravity – i.e., Grade 3+ at least in the Medical Research Council (MRC) scale for the muscle strength test. Following the above inclusive and exclusive criteria, participants including five inpatients and thirteen outpatients from Zhongda Hospital (affiliated with Southeast University) and Nanjing Tongren Hospital were recruited and randomized into one of two groups: an experimental group (robot-aided therapy) and a control group (conventional therapist therapy). Their demographic characteristics are shown in Tables 1 and 2.
Demographic characteristics of the stroke patients in the experimental group

Demographic characteristics of the stroke patients in the control group

2.2 Experimental setup
The prototype therapeutic robotic system for the upper-limb progressive resistance training shown in Fig. 1 consists of a Barrett WAM™ Arm (

Therapeutic robotic system prototype with Barrett WAM™
2.3 Training protocol
2.3.1 Experimental group
Individuals randomized to the experimental group received WAM-aided progressive resistance rehabilitation therapy. No other therapy methods were provided in this group. The clients are seated in a chair or wheelchair in front of a computer screen at a height adjustable table. In this study, the robot is restricted in the vertical plane with control threads and a pilot study of elbow flexors resistance recovery training in one plane was performed, which is commonly adopted in traditional therapist-centred muscle strength training. The stroke participant grasps the WAM robot and performs lift-and-reach exercises, whereby the exercises require the patient to move the WAM through several target points with different task difficulties, though no predefined trajectory was needed. Fig. 2 shows a side view of the graphical user interface used for the progressive resistance training. An adaptive resistive force regulated by the proposed hierarchical controller is exerted at the robot end-effector. These exercises are designed to allow the patient to perform some meaningful functional activities, such as reaching and lifting objects during the activities involved in daily living.
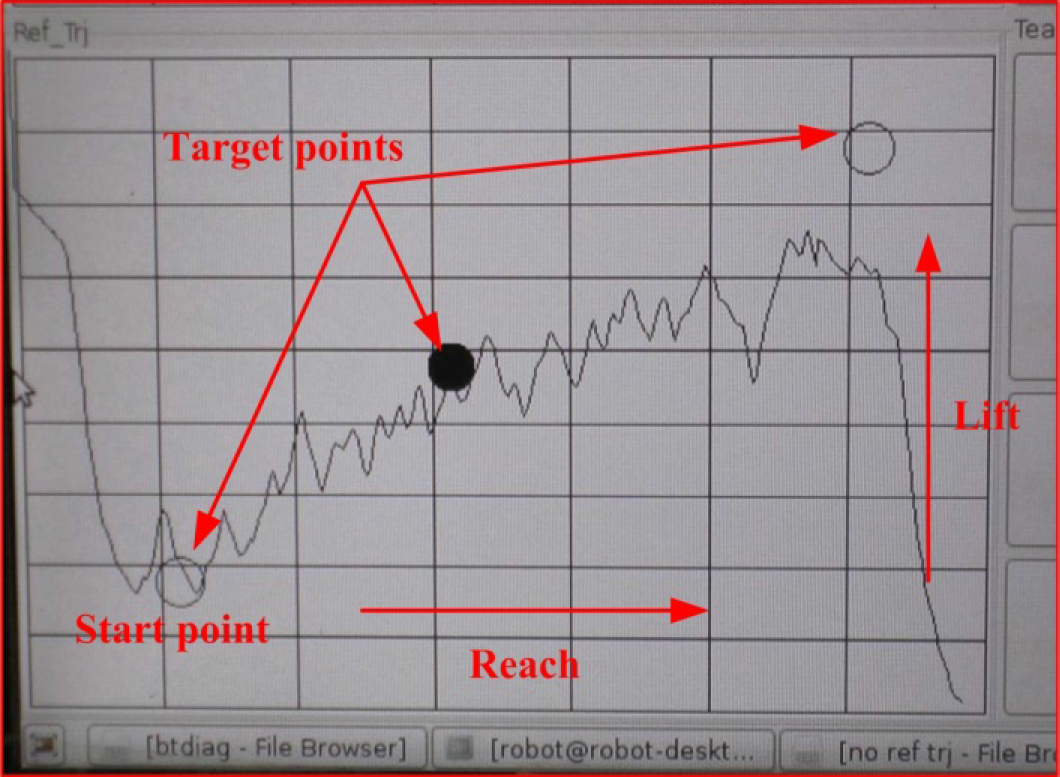
A side view of the graphical user interface for the progressive resistance training
2.3.2 Control group
Similarly, individuals randomized to the control group received conventional therapist therapy. Assorted techniques and progressive resistance programmes for upper extremity retaining were used by the treating therapists. For both groups, the resistance training programme consisted of three sets of 15 repetitions per exercise session, 2 exercise sessions a day, 3 days a week over a period of 16 weeks.
2.3.3 Outcome measure
A robot-aided rehabilitation training system is used as the main therapy outcome test platform and the robotic measured parameters are objectively selected as quantitative evaluation indices. A standard assessment procedure is used at the start and at the end of treatment for both groups. To ensure that there is no bias in comparing the two groups, the patients allocated in the conventional group had to be familiarized with the robot-aided training environment before the therapy outcome evaluation procedure could be carried out. This procedure includes the following outcome evaluation parameters:

where x, y and z are the position of the WAM end-effector on the x, y and z axis, respectively, t is the movement time and s is the movement distance.
2.4 Hierarchical controller design
With the progressive resistance training, it is desirable that the resistive force be exerted in a moderate and challenging, but engaging and motivating manner, without causing boredom, frustration or harm. Fig. 3 gives the block diagram of the robot-assisted progressive resistance hierarchical control framework which is composed of a high-level progressive resistance supervisory controller and a low-level adaptive resistive force triggered controller.

Block diagram of the robot-aided progressive resistance adaptive hierarchical control framework
2.4.1 High-level progressive resistance supervisory controller
The high-level progressive resistance supervisory controller is mainly used to determine the resistive force base for each training session based on the participant's motion performances, which are characterized by the impaired limb's movement velocity and the resistive force endured. The fuzzy regulator is designed to provide the adaptive resistive force base in agreement with the impaired limb's muscle power restoration, where the changes of the average resistive force ΔAvg(fres) and movement velocity ΔAvg(v) are selected as inputs while the resistive force base adjustment coefficient Δuf is used as the output. The resistive force base control law is defined as:

where fini is the determinate resistive force base, fres is the actual resistive force exerted on the impaired limb, uf is the adaptive factor regulated by the resistive force base fuzzy regulator, Abs(•) and Avg(•) denote the absolute and average value, and i – 1, i and i + 1 refer to the (i – 1)th, ith and (i + 1)th training session.
During the fuzzification process, the input and output of the fuzzy regulator are scaled to five triangle-shaped or trapezoidal membership functions (MFs), namely, negative big (NB), negative small (NS), zero (ZE), positive small (PS) and positive big (PB). Table 3 and Fig. 4 show the inference rules and MFs for the fuzzy regulator.
Fuzzy inference rules for the coefficient Δuf

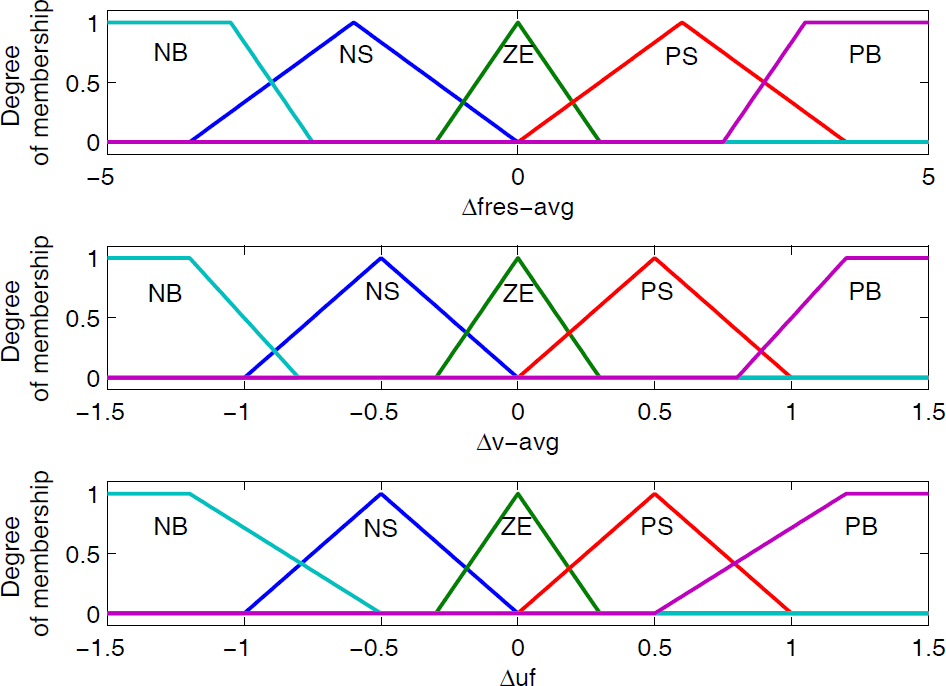
MFs for the high-level resistive force base fuzzy regulator
Generally, if Δvg(fres) and ΔAvg(v) are both positive – which implies that the patient has good muscle force recovery then a bigger resistive force base value may be exerted. Otherwise, a smaller resistive force base value should be added. In addition, if the changes of ΔAvg(fres) and ΔAvg(v) are opposite, positive or negative increments must be supplied relying on the resistive force and movement velocity change characteristics.
2.4.2 Low-level adaptive resistive force triggered controller
With regard to the high-level progressive resistive supervisory controller, the resistive force base is not determined until one training session is finished. It is well known that any progressive resistance training which constantly challenges the patient will produce the maximal therapy outcome. In each training session, several (or more) training sets are included and the exerted resistive force may not be challenged during one training session if only the high-level progressive resistive force supervisory controller is applied. The idea behind a low-level adaptive resistive force triggered controller is to further regulate the interactive resistive force in a triggered and challenged way based on the changes of the impaired limb's biomechanical state in one training session.
A. Estimation of the patient's biomechanical state
As mentioned in Refs.[17][18], the human arm's bio-impedance parameters, bio-damping and bio-stiffness can sensitively reflect the arm's muscle power changes. Based on our previous work in Ref.[6], the impaired limb's bio-impedance characteristics can be modelled as the following linear time-variant system:

where fe denotes the interaction force between the robot and the impaired limb, δx = x – xe is the displacement between the actual position and the equilibrium position of the impaired limb, δẋ is the velocity vector, and be and ke denote the impaired limb's bio-damping and bio-stiffness respectively.
Using the bilinear transformation in Ref.[19] where the robot environment was modelled as a linear time-invariant spring-damper system, Eq. (3) can be reorganized in the discrete-time domain as:

where T is the sampling period and z−1 is one shift step in the time domain. According to Eq. (4), the continuous linear time-variant model is discretized to provide a model for linear estimation:

where:

Furthermore, Eq. (5) can be represented as regression vector as follows:

where θ[k] is the estimated parameter vector, and h[k] and y[k] represent input and output regression vectors, respectively.
According to the regressive least square method with the forgetting factor (FRLS), we have:

where λ is the constant forgetting factor, which influences the weight given to earlier data relative to the newly acquired data. The covariance matrix P[k] can be calculated as:

In Ref.[19], the estimated results using the above FRLS method were still not satisfactory – especially for the damping coefficient – although the given environment parameters, stiffness and damping are constant. In robot-aided clinical rehabilitation, the impaired limb's dynamics vary randomly and its bio-impedance parameters are time-variant throughout the whole rehabilitation process. It is suggested that the estimation of the impaired limb's bio-impedance parameters using RLS with an adaptive forgetting factor (AFRLS) is superior to that with a fixed forgetting factor. The forgetting factor may be adapted as:

where l and R are the forgetting step and parameter. In addition, the maximum and minimum forgetting factors λmax and λmin may be set to prevent unfortunate disturbance. After the vector θ is estimated, the impaired limb's bio-damping b̂e and bio-stiffness k̂e can be obtained from Eq. (6):

B. Fuzzy adaptive resistive force triggered controller
The low-level adaptive resistive force triggered controller consists of two parts: activation and regulation. As to activation, the changes of the patient's bio-damping and bio-stiffness are calculated first, and if the patient's bio-impedance changes exceed the predefined thresholds, the patient is considered to have good muscle strength endurance with the current resistive force level. Accordingly, the triggered controller is activated to provide a slightly bigger but challenged resistive force. On the contrary, the triggered controller doesn't work. After activation, the fuzzy regulator is designed based on the patient's bio-impedance changes so as to adjust the velocity-based adaptive coefficient and to further regulate the resistive force.
Note that each participant requires some settling time to generate a certain amount of muscle strength and to perform resistive exercise. In addition, the estimated impaired limb's biomechanical state parameters may witness sharp changes resulting from the unknown noise disturbance. Therefore, the triggered controller will not be activated if only the changes of the impaired limb's instantaneous bio-impedance values exceed the predefined thresholds. The averages of the impaired limb's bio-damping/stiffness (b̂e_avg, k̂e_avg) and their changes (Δb̂e_avg, Δk̂e_avg) are calculated in a given time interval and used to decide whether the triggered resistive force is needed. The following equations are calculated:


where ti, tf and ts are the starting time, final time and sample time, respectively, b̂e(t) and k̂e(t) are the estimated impaired limb's bio-damping and bio-stiffness, while j – 1 and j denote the (j – 1)th and jth activation.
The adaptive resistive force triggered strategy is defined as:

where ftrig is the triggered resistive force, v is the impaired limb's movement velocity, uv is the velocity-based coefficient regulated by the triggered resistive force fuzzy regulator, Abs(•) and Avg(•) denote the absolute and average value, and j – 1, j and j + 1 refer to the (j – 1)th, jth and (j + 1)th resistive force trigger.
In the fuzzy triggered regulator, the patient's average bio-damping/stiffness changes (Δb̂e_avg, Δk̂e_avg) and the velocity-based adaptive coefficient Δuv are selected as input and output variables, respectively. All these input and output variables are mapped to five skewed triangular or trapezoidal MFs (NB, NS, ZE, PS, PB). Fig. 5 depicts MFs for the input and output variables, respectively. If Δb̂e_avg and Δk̂e_avg are positive – which implies that the impaired limb's muscle force is strengthened – then the positive increment Δuv may be added to the velocity-based factor uv. On the contrary, if Δb̂e_avg and Δk̂e_avg are negative, this means that a small amount of muscle strength is generated and that a proportional negative increment Δuv should be supplied. Fig. 6 shows the control surface of the proposed fuzzy adaptive resistive force triggered controller.

MFs for the resistive force triggered fuzzy regulator
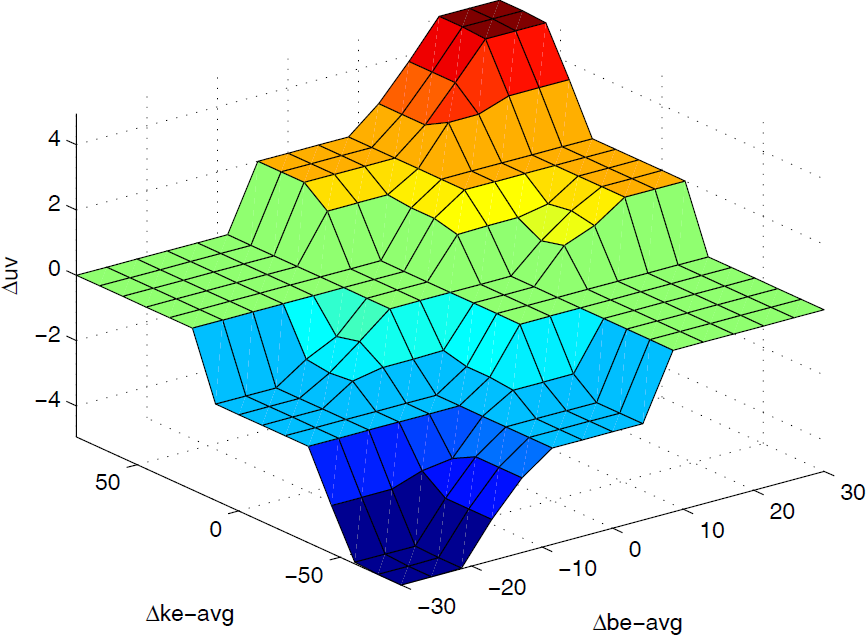
Control surface of the fuzzy triggered regulator
2.5 Safety
Ensuring safety of the participants constitutes a very important issue when designing a robot-aided rehabilitation system. The WAM Arm rehabilitation safety system consists of the pendants and the safety board/module which are used to monitor the joint torque and velocity, communication between the computer and the Pucks™ (motor controllers), the voltage levels to the WAM and the various safety states, including E-STOP, IDLE and ACTIVATED. The safety module will register a heartbeat fault and shut down the WAM manipulator in the case where the corresponding joint torque, velocity and voltage levels exceed the predefined limits or else any motor controllers fail to issue any communication. In addition, the robot can also be stopped by shutting down the power supply with an emergency button activated by either the stroke patients themselves or else the physical therapist.
3. Results
3.1 Resistive force base and its coefficient adjustment result
According to DeLorme's progressive resistive training method [20], the stroke patients are first asked to perform ten-repetition maximum (10RM) resistive exercises and 60–65% of 10RM is set as the resistive force base of the first training session. The fuzzification input variables ΔAvg(v) and ΔAvg(fres) are set from −1.5 to 1.5 and −5N to 5N, respectively. The output variable Δuf is defined from −1.5 to 1.5. Fig. 7 shows the representative results of the resistive force base and its corresponding coefficient adjustment for patients R3 and R4 during the course of continuous twenty-four training session samples. It is clear that the resistive force bases for R3 and R4 can be progressively and steadily increased with the progress of resistance training. There were still some trivial fluctuations in resistive force base regulation. This is because the original resistive force base may be set beyond the patient's actual muscle strength and the fuzzy supervisory controller can then adjust the force-based adaptive factor so that the resistive force base values can match the patient's muscle force changes.

Representative results of resistive force base and its corresponding coefficient adjustment for patients R3 and R4
3.2 Low-level adaptive resistive force triggered control result
3.2.1 Estimation result of the arm's bio-impedance parameters
To investigate the relationship between the arm's bio-impedance characteristics and its muscle power changes, the participant was asked to actively perform the same sinusoidal trajectory exercise in a vertical plane under three different conditions: full, zero gravity compensation for the WAM robot and the participant's intentionally increased muscle force. The parameters xe, T, λmax, λmin, l, R, θ0 and P0 of AFRLS were chosen as 0.576, 0.05, 0.99, 0.1, 5 and 20 respectively. Fig. 8 shows the estimation of the arm's bio-damping and bio-stiffness parameters with full and zero gravity compensation. Compared with the results at full and zero gravity compensation, it is observed that the arm's bio-damping and bio-stiffness are close to zero under the former condition while those in the latter case increase significantly. This is because very little muscle strength is needed with full gravity compensation, but with zero gravity compensation the subject has to generate a certain muscle force to overcome the WAM robot's gravity. Further verification was conducted by asking the subject to apply intentional force when performing the same exercise at full gravity compensation, shown in Fig. 9. It is obvious that the estimated bio-impedance parameters show a substantial increase at the moment when the arm generates intentionally increased muscle force. All these results confirm that both the arm's bio-stiffness and its bio-damping can sensitively reflect the arm's muscle power changes by using the AFRLS algorithm, which is an improvement compared with the results obtained in Refs.[17][18] and may be used as objective indices for evaluating the patient's muscle strength recovery.

Estimation of the arm's bio-impedance parameters with full and zero gravity compensation for the WAM robot

Estimation of the arm's bio-impedance parameters with the participant's intentionally increased muscle force
3.3 Fuzzy adaptive resistive force triggered controller
The averages of the impaired limb's bio-damping/stiffness (b̂e_avg, k̂e_avg) and their changes (Δb̂e_avg, Δk̂eavg) are calculated every five-repetition (rpt) intervals. Thresholds for the patient's bio-impedance changes are set as Abs(Δb̂e_avg) ≥ 8 and Abs(Δk̂e_avg) ≥ 40, respectively. To avoid substantial changes resulting from any unknown disturbance and ensure the patient's safety, the upper limits are also set as Abs(Δb̂e_avg) ≤ 20 and Abs(Δk̂e_avg) ≤ 65. The triggered resistive force controller of the WAM-based progressive resistance muscle strength training system monitors the patient's bio-damping and bio-stiffness changes over the course of one training session. Once the changes simultaneously enter into the triggered band, the triggered controller is activated and the fuzzy regulator begins to work. The activation of the triggered controller for each patient in the control group is recorded.
The activation segments of the resistive force triggered controller for patients R1 and R7, as examples, are shown in Fig. 10. The patient's bio-impedance average changes are calculated at rpt=5, 10, 15,…., 45 for one training session.

Average changes of bio-damping/stiffness and the activation of the triggered controller for patients R1 and R7 during resistive exercise
Fig. 11 describes the velocity-based coefficients and triggered resistive force regulation profiles. Synthesizing the results of activation with fuzzy regulation for the resistive force triggered controller, it is obvious that positive activation and progressively increased resistive force for R1 can be found. With further analysis for R7, a negative velocity-based coefficient and triggered resistive force regulation are observed at the 15th repetition interval. The reason for this is that the negative changes of the bio-impedance values for R7 resulting from unreasonable triggered resistive force or other psychophysiological factors exceed the triggered thresholds and the fuzzy regulator has to revise the triggered resistive force in order that it can be in agreement with the patient's muscle force recovery.
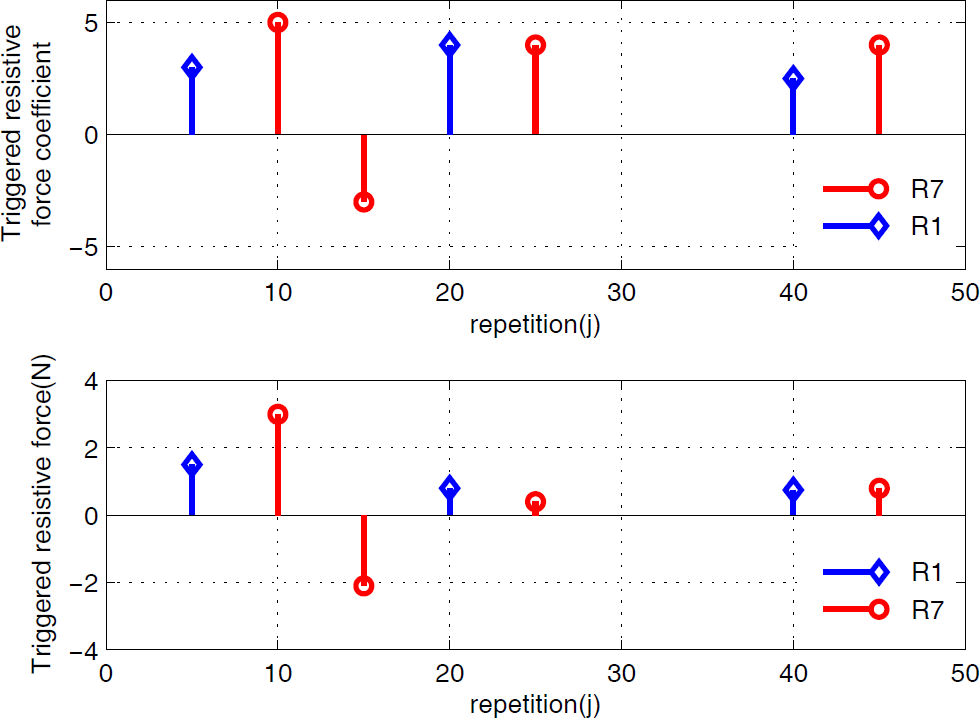
Results of velocity-based coefficient adjustment and triggered resistive force for patient R1 and R7
3.3 Therapy outcome evaluation and statistical analysis
Data is compared to determine the effectiveness of robot-assisted versus conventional therapy treatments. As mentioned in 2.3.3, movement smoothness, movement velocity and maximum resistive force are selected as the primary outcome measures for the robot-assisted and conventional groups. The subjects in both groups are requested to perform five successful trials and the average test values are used as final evaluation results. The difference in each outcome measure from pre- to post-training is statistically analysed with Student's t-test methods using SPSS Statistical Software (Lead Technologies, Inc., Chicago, USA). Those P-values of 0.05 or less are considered as statistically significant. Table-4 shows the results of the therapy outcome evaluation and statistical significance.
Average improvements of three outcome measures for the experimental and conventional groups

At the functional level, both groups perform well, with improvement in the scores on three outcome measures and showing clinical and statistical significance. Individuals in the robotic therapy group, on average, improve by (381.9, p=0.001), (12.5, p=0.002) and (33.8, p=0.000) on movement trajectory smoothness, mean movement velocity and maximum resistive force, respectively. Under the conventional therapy, three outcome measures all see certain improvements, but not significantly so for movement smoothness (238.4, p=0.002), the mean movement velocity (10.8, p=0.002) or the maximum resistive force (25.1, p=0.001). Compared with the differences in treatment for movement smoothness (143.5, p=0.041), mean movement velocity (1.7, p=0.142) and maximum resistive force (8.7, p=0.025), it is clear that the improvements of the three outcome measures under robot-assisted therapy are significantly greater than those under conventional therapy. Significant differences in both movement smoothness and maximum resistive force measures are revealed between pre- and post-tests except for the mean movement velocity.
The robotic assessment sample given in Fig. 12 shows the movement trajectory change at pre- and post-training for patient R3 while moving the WAM through the predefined target points. 5N and 10N resistive forces are exerted at the pre- and post-evaluation procedure, respectively. As a further comparison, the movement trajectory performed by the unaffected arm is also demonstrated. Compared with the three profiles, it is clear that patient R3 displays a more normalized movement trajectory – even with a larger resistive force at post- versus pre-therapy – as the training trial progresses, which indicates that their muscle strength and motor control capability have made great improvement over the course of robot-aided treatment. Fig. 13 displays an example of hand movement velocity curves at pre-and post-training with one repetition for patient R4 in which 9N resistive force is exerted at the robotic end-effector. In spite of a small oscillation existing in the post-training speed profile, a much smaller oscillating frequency and amplitude is achieved after sixteen weeks of training. It is further verified that robot-aided resistance training not only enhances the impaired limb's muscle strength but also that it improves the affected arm's motor control ability.
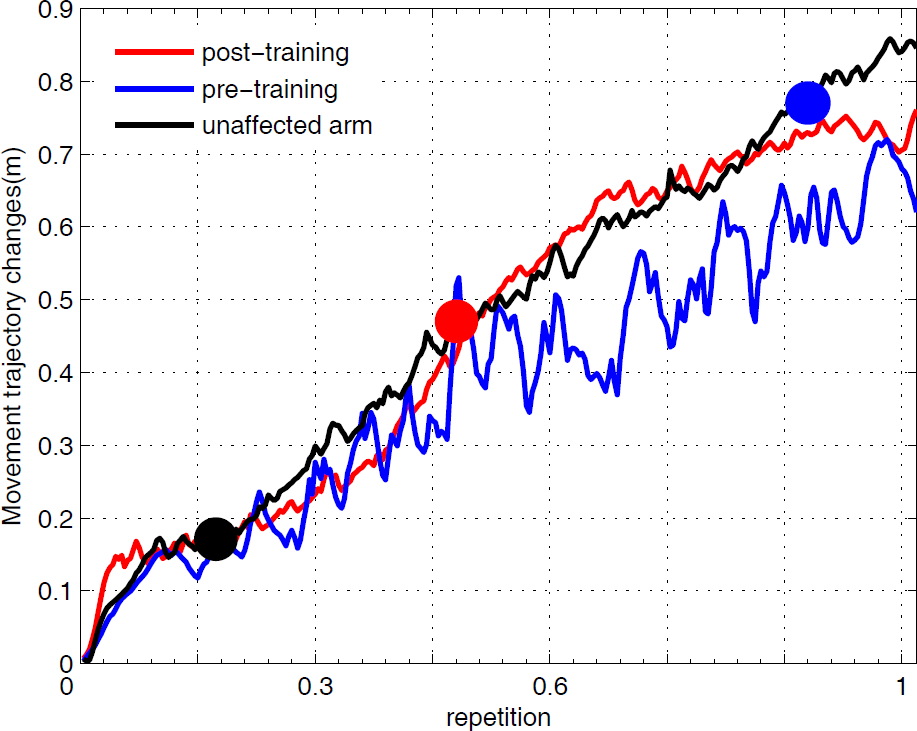
Sample movement trajectory smoothness comparison at pre- and post-training for patient R3. 5N and 10N resistive force is exerted at the pre- and post-evaluation procedures, respectively.

Representative movement velocity profiles comparison at pre- and post-treatment with one repetition for patient R4. 9N resistive force is exerted at the pre- and post-evaluation procedures, respectively
Fig. 14 and Fig. 15 describe the sustained average maximum resistive force and mean movement smoothness computation results for the patients in the robot group for pre- and post-test measures with five successful trials, respectively. The latter is implemented under conditions of 5N resistive force. There are significant increases in the average maximum resistive force outcome measure, where the least improvement for patient R9 is 19.6N±1.8166. Further analysis of the patients' lifting and reaching abilities show substantial decreases in Fig. 15, with mean changes of 381.9±52.4 observed on NJS computation, which indicate that jerk decreases dramatically and that more efficient and smoother training movements are achieved with the progress of resistance exercises.

Average maximum resistive force at pre- and post-training for patients in the robot group (9 subjects). The error bar is the standard error of the mean.
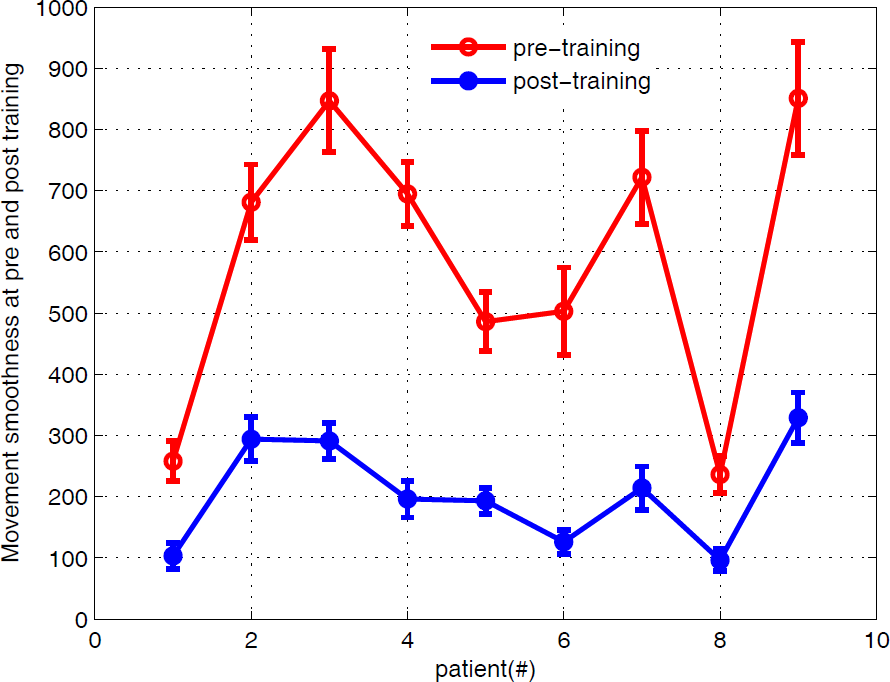
Average movement smoothness at pre- and post-training for patients in the robot group (9 subjects). The error bar is the standard error of the mean.
4. Discussion
The primary goal of this study is to carry out clinic experimental studies and to explore the effect of an adaptive hierarchical therapy control algorithm on the muscle strength recovery of stroke survivors which integrates a high-level resistive force base fuzzy supervisory controller and a low-level fuzzy adaptive resistive force triggered controller. This is compared with a conventional therapist-centred therapy method for a control group. Preliminary therapy evaluation results with the three outcome measures show that robot-aided progressive resistance exercises over a 16-week period can not only improve the muscle strength of the impaired limb but also enhance the motor control and coordination capability for the hemiparetic arm. Moreover – and in comparing the differences between the two treatments – on average, stroke patients in the robot group display better clinical improvements than those in the conventional group. This also indicated that the robot-aided progressive resistance training method that integrates a resistive force base determination with real-time resistive force triggered regulation has the potential to improve stroke patients' muscle strength.
With the WAM-aided progressive resistance training, the question of how to challenge stroke participants in a moderate but engaging and motivating manner formed the main idea behind this study. To do this, adaptive and triggered mechanisms in the form of a hierarchical supervisory control are presented. The proposed low-level adaptive resistive force triggered controller intermittently optimizes the exerted resistive force base in a bio-cooperative way based on the average changes of the impaired limb's bio-impedance during one training session. In other words, if the resistive force base is set too high or too low, the resistive force triggered controller will decrease or increase the unreasonable resistive force so as to prevent secondary injury to the impaired limb's muscle tissue and to challenge the patient in an encouraging way. This is beneficial to aid the stroke patient's active effort and self-initiated movements as well as to improve the impaired limb's muscle strength. Another important advantage of the proposed therapy control framework in this study is that the resistive force between the WAM and the impaired limb is exerted in a hierarchical and progressive way, and this is helpful in performing a stable interaction and avoiding any fluctuation in hemiparetic arm's motor control or coordination.
As a preliminary investigation, the proposed robot-aided hierarchical progressive resistance training method shows a clinical therapeutic effect. However, and in the resistive force triggered controller, the triggered bands for the average changes of the impaired limb's bio-damping/stiffness are still predefined by the therapist. An adaptive mechanism should be explored for the determination of the bio-impedance changes triggered thresholds.
5. Conclusions
An adaptive hierarchical therapy control framework integrating a high-level resistive force base fuzzy supervisory controller and a low-level resistive force triggered fuzzy regulator is developed. Two groups of post-stroke patients are randomly allocated in WAM-aided and conventional physical therapy groups, participating over sixteen weeks in progressive resistance training. Preliminary clinical therapy outcome measures indicate that robotic-aided rehabilitation therapy alone (i.e., without additional physical therapy interventions) tailed to the paretic arm is as effective as conventional therapist-centred rehabilitation training and even more effective than standard physiotherapy treatment for those patients with a mild or moderate physical condition. A further conclusion that can be drawn from our findings is that robot-aided progressive resistance training with the proposed therapy control algorithm can not only enhance a patient's muscle strength but also improve the hemiparetic arm's motor control and coordination. This is very important for stroke patients to improve their daily living.
Footnotes
6. Acknowledgements
This work is jointly supported by the National Natural Science Foundation of China (61104216, 61104206, 11202107), the Natural and Science Foundation of Jiangsu (No. BK2010063, BK2012832), the Natural Science Foundation for Colleges and Universities of Jiangsu Province of China(12KJB510015, 11KJB130002), the Scientific Research Foundation of Nanjing University of Posts and Telecommunication (NY211020) and the Priority Academic Programme Development of Jiangsu Province (YX002001).