
Abstract
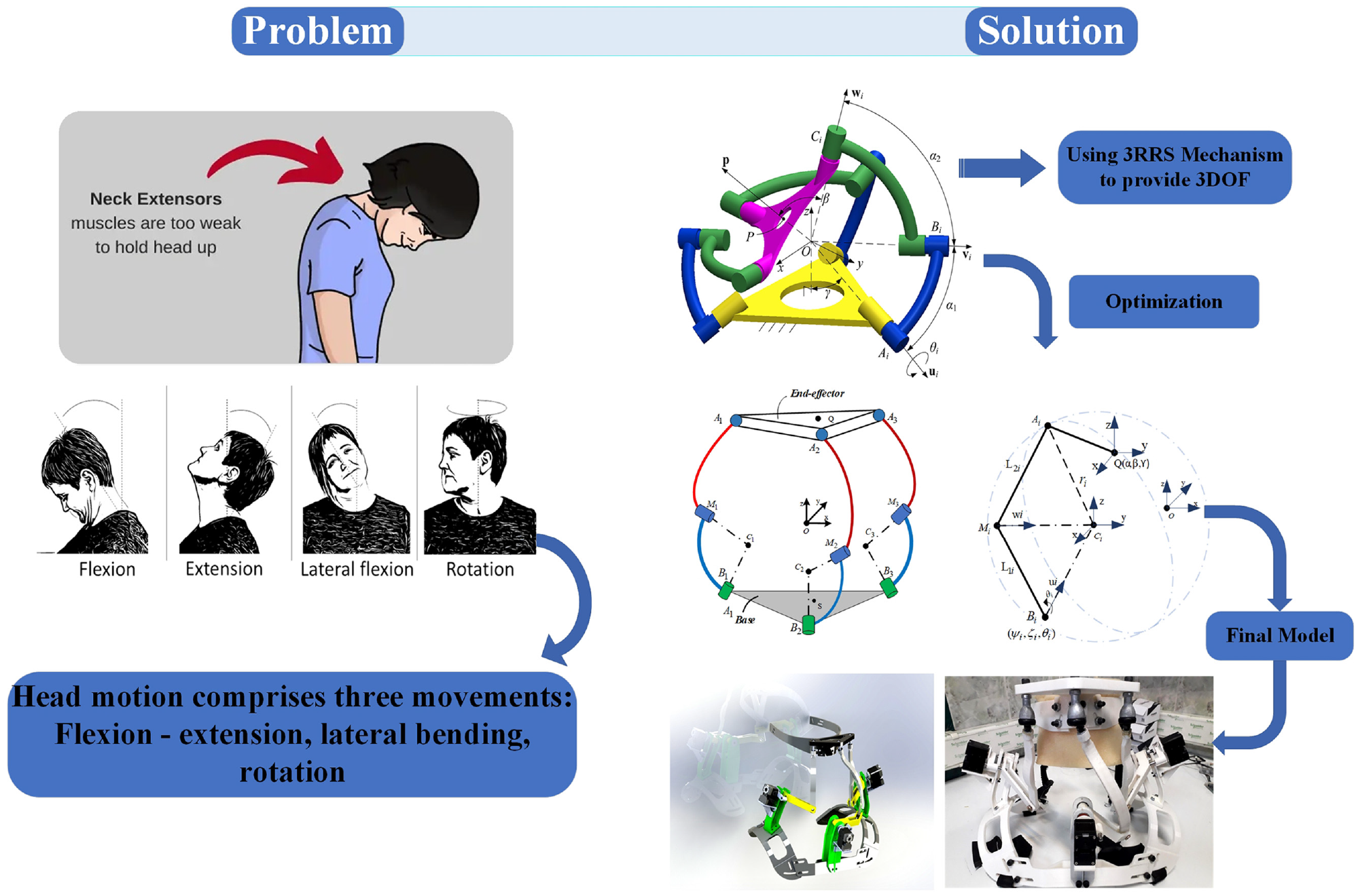
Patients with neurological disorders, such as amyotrophic lateral sclerosis, Parkinson’s disease, and cerebral palsy, often face challenges due to head-neck immobility. The conventional treatment approach involves using a neck collar to maintain an upright head position, but this can be cumbersome and restricts head-neck movements over prolonged periods. This study introduces a wearable robot capable of providing three anatomical head motions for training and assistance. The primary contributions of this research include the design of an optimized structure and the incorporation of human-robot interaction. Based on human head motion data, our primary focus centered on developing a robot capable of accommodating a significant range of neutral head movements. To ensure safety, impedance control was employed to facilitate human-robot interaction. A human study was conducted involving 10 healthy subjects who participated in an experiment to assess the robot’s assistance capabilities. Passive and active modes were used to evaluate the robot’s effectiveness, taking into account head-neck movement error and muscle activity levels. Surface electromyography signals (sEMG) were collected from the splenius capitis muscles during the experiment. The results demonstrated that the robot covered nearly 85% of the overall range of head rotations. Importantly, using the robot during rehabilitation led to reduced muscle activation, highlighting its potential for assisting individuals with post-stroke movement impairments.
Keywords
Introduction
Head drop is a prevalent symptom observed in individuals with neurodegenerative diseases, including Amyotrophic Lateral Sclerosis (ALS), Cerebral Palsy, and Parkinson’s.1–5 This condition is characterized by severe weakness in the neck extensor muscles, resulting in the inability to hold or move the head properly. Consequently, individuals affected by head drop face difficulties in maintaining eye contact, swallowing, breathing, and engaging in social interactions. The natural movement of the head plays a crucial role in facilitating face-to-face conversations and enabling respectful and effective communication.1,6 Traditional rehabilitation approaches involve one-on-one interactions between patients and physical therapists, which have proven to be valuable in the rehabilitation process. 7 However, this method has disadvantages such as high therapist workload, prolonged treatment duration, elevated therapy costs, and the potential for monotony for both patients and therapists. Manual assistance provided by therapists is typically limited to rehabilitation centers or hospitals, requiring specific conditions and considerable time before the beneficial effects of therapy become apparent. 8 Similarly, assistive devices have been developed to aid individuals with weak muscles in restoring their functional abilities.9–11 In the case of a head drop, existing treatments involve the use of static braces such as the “Sheffield Port Snood” or “Miami J.”12–15 However, these rigid, semi-rigid, or soft collars fail to adequately address head movements, often resulting in muscle fatigue. For instance, a study evaluating the effects of Philadelphia and Miami J collars on pulmonary function reported a statistically significant expiratory flow obstruction after using both collar types. 16 Furthermore, a study assessing the effects of four commercial cervical collars (Aspen, Philadelphia, Miami J, and Miami J with Occian back (Miami J/Occian)) on cervical range of motion (CROM) and mandibular and occipital tissue-interface pressure (TIP) revealed that Miami J and Philadelphia collars restricted CROM to the greatest extent. 17 Additionally, Miami J and Miami J/Occian back collars had the lowest levels of mandibular and occipital pressure, but there is a risk of occipital pressure ulcers without compromising immobilization. 17 Consequently, these soft and rigid collars can lead to skin deterioration and impede vital functions such as breathing, swallowing, and engaging in conversations. Moreover, their design, which maintains the head in an upright position, contributes to the gradual weakening of the neck muscles over time.
In recent decades, there has been increasing interest in robotic-assisted rehabilitation solutions that offer unique advantages over conventional manual methods. 18 Rehabilitation robots provide high-efficiency training programs that can be customized to meet the specific recovery progress and conditions of each individual. 19 This approach offers consistent training patterns without inducing fatigue, allowing therapists to tailor training plans for optimal patient outcomes.20,21
In the context of neck disorders, some previous work has explored the use of medical robotics. For example, a dynamic brace was introduced as a tool to aid patients with head drop due to ALS in restoring normal head motion. 22 However, this design had limitations, as it was unable to achieve a wide range of natural head rotations. In head extension, the achievable range of motion was only 53.1% of the natural range, and the effectiveness of the brace in terms of human interaction was not thoroughly studied. 23 Another proposed solution was a three-degrees-of-freedom Revolute-Prismatic-Spherical configuration parallel manipulator.24,25 However, this design rigidly enclosed the neck and supported the head at the level of the chin, which made conversation and breathing challenging for the patient. A cable-driven robotic brace capable of providing three degrees of freedom in human head movements was also introduced. 26 Although it offered mobility, it lacked portability, had lower stiffness compared to parallel mechanisms, and its efficacy was not investigated through human testing. In another study, a dynamic neck brace rehabilitation device was designed to measure the position, orientation of the head, and pressure forces exerted on the head due to traction.27,28 However, the motion range of the brace was limited, allowing only 12% of normal head movements (−8.10 ± 0.02° to 8.12 ± 0.01°). These previous works highlight the need for an improved and comprehensive solution for neck rehabilitation that offers a wide range of natural head movements, portability, and effective human testing to ensure its efficacy.
This paper introduces a wearable robot designed to assist individuals with muscle defects in regaining mobility and motor functions in head-neck movements. The robot must have two distinguishing features, (i) The robot’s structure should cover a considerable range of head movements to adapt to neutral head movements, (ii) as it will interact with humans, its movements must be safe and offer interaction space when it uses with subjects. The robot’s design is based on motion capture data collected from a healthy subject’s head and neck. Utilizing a spherical parallel mechanism, the robot provides three degrees of freedom for the head. Geometrical parameters of the robot’s workspace were optimized for improved dexterity performance using a genetic algorithm (GA). The resulting robot design incorporates unique features and is fully portable. Three servomotors are employed to measure joint angles within the robot, enabling human-robot interaction during head motion, and a simulation assists in calculating the position and orientation of the head.
In robot-assisted rehabilitation, the control strategy is one of the vital components determining its usefulness.29–31 Compliance control, which ensures safe physical human-robot interaction, allows patients to follow trajectories with reasonable interaction forces. 32 This approach facilitates human-robot interaction during tasks, encourages active patient participation, and enhances movement safety.33,34 To ensure safety in this study, a compliance control method was developed to provide assist-as-needed force to subjects during the robot’s movements.35,36
The effectiveness and motion assistance provided by the robot under this control scheme was evaluated through an experiment involving 10 healthy subjects. The subjects performed lateral bending in both passive and active states, and surface electromyography signals (sEMG) were utilized to quantify the activity of the splenius capitis muscles during the movement. Kinematic parameters, specifically movement errors in head angles, were analyzed to demonstrate improvements achieved through the robot’s performance in both states.
Overall, the objective of this study is to design a robotic collar specifically intended for individuals with neck disorders. The aim is to assist them in regaining their movements by providing dynamic head movements under interactive forces. The robotic collar serves as a supportive device that facilitates rehabilitation and promotes the recovery process for patients with neck-related impairments. Its construction was optimized based on human head motion data to accommodate a vast range of neutral head-neck movements. Additionally, by offering targeted assistance and interaction, the robotic collar aims to enhance the mobility and functional abilities of individuals affected by neck disorders. The following sections detail the robot’s design, control strategy, and experimental evaluation, providing valuable insights into its potential for effective neck rehabilitation.
System design
Considering the anatomical motion of the head and neck, which includes flexion, extension, lateral bending, and rotation, it is crucial to develop a device that can accommodate these movements. 37 Biomechanically, the head is attached to the trunk by a series of cervical joints and vertebrae. Consequently, the head conducts a predominant spherical motion with a trivial translation. Therefore, a spherical mechanism that provides three degrees of freedom can not accommodate the fully spherical and translational motion of the head. The proposed mechanism is similar to a spherical parallel structure with three revolute-revolute-spherical joints (3-RRS) that provide three degrees of freedom. 22 In this mechanism, the three distinguished and non-aligned points in the body move on separated-concentric spheres, so the rotational and translational movements of the rigid body can be achieved.
As opposed to a spherical parallel structure, in which the axes of the revolute joints converge at a single point (O in Figure 1(a)),
38
in this mechanism, the common point (Ci) for each separate chain is considered as the intersection of their revolute joints.
22
As shown in Figure 1(a), the axes of revolute joints
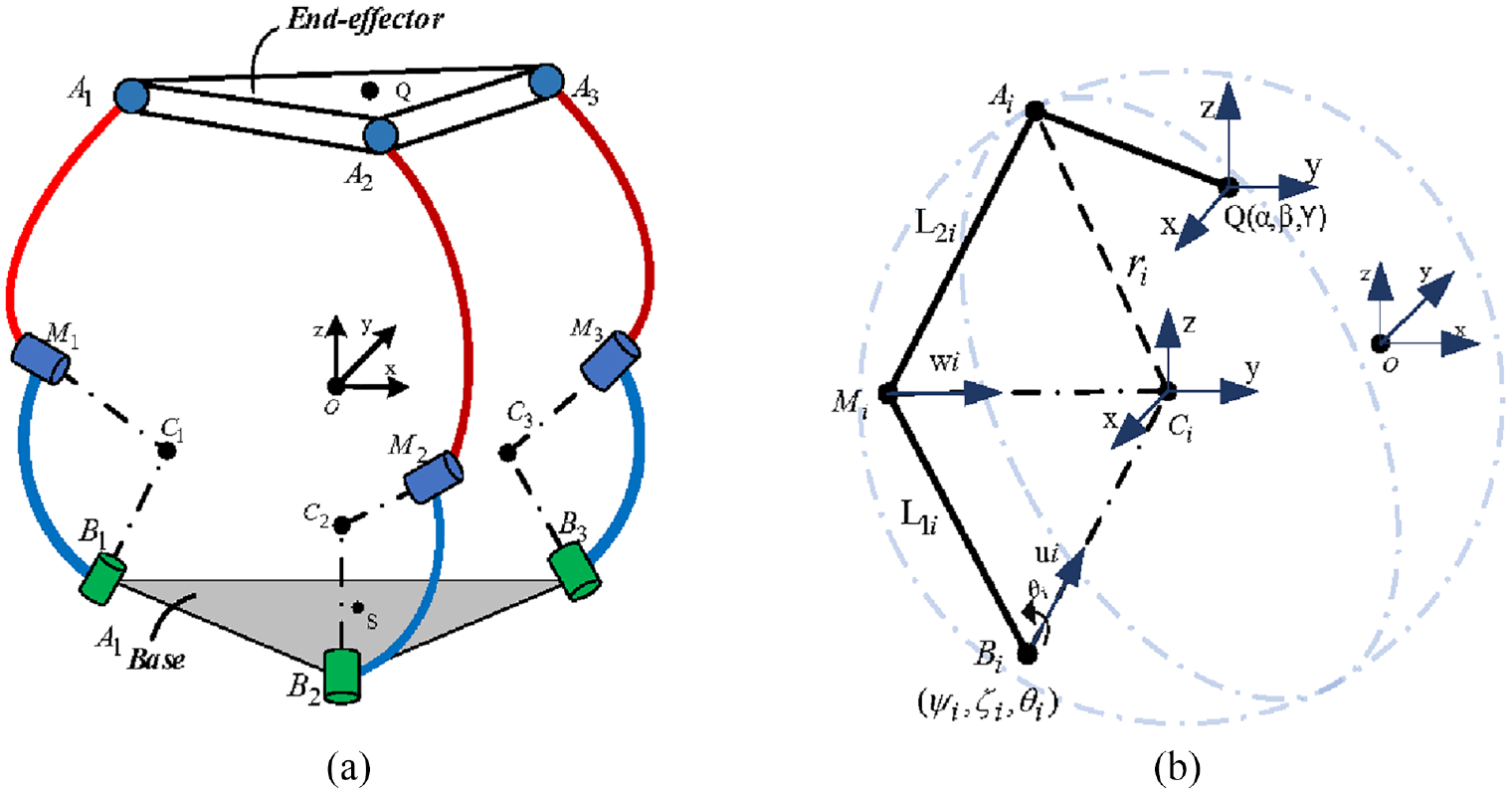
(a) The mechanical structure of the robot and (b) a chain of the mechanism and its characteristics.
This mechanism has some advantages: (1) the parallel structure is more precise and more robust. Its design could be small and reduce the moving inertia. (2) RRS chain has good accuracy, is suitable to realize, and is lightweight. (3) From a manufacturing perspective, it is easy to fabricate a chain in which the two revolute joints intersect rather than all of the revolute joints in each chain.
Optimization and simulation
Optimization to calculate Ci in each chain
The system was designed based on the analysis of the anatomical head-neck kinematics data of one person. First, eight infrared cameras were used with a lab-based motion capture system from VICON (ProCalc 1.2). It was used to record the natural head movement of a person. Eight markers were placed on the face, the head, and the shoulders, as shown in Figure 2(a). According to Figure 2(b), these markers were used to construct the trunk and head frames. With the x-axis running from left to right, the origin of the trunk frame is located at the center of the left and right shoulder markers. The origin of the head frame is defined as the position of the x-axis pointing in the direction of the left cheek marker, based on the geometric center of the triangle formed by the left cheek marker, right cheek marker, and inion marker. First, a static trial was conducted with the individual standing upright to determine the relative positions of the markers. A total of three head/neck movements were recorded, which included flexion-extension, lateral bending, and axial rotation.
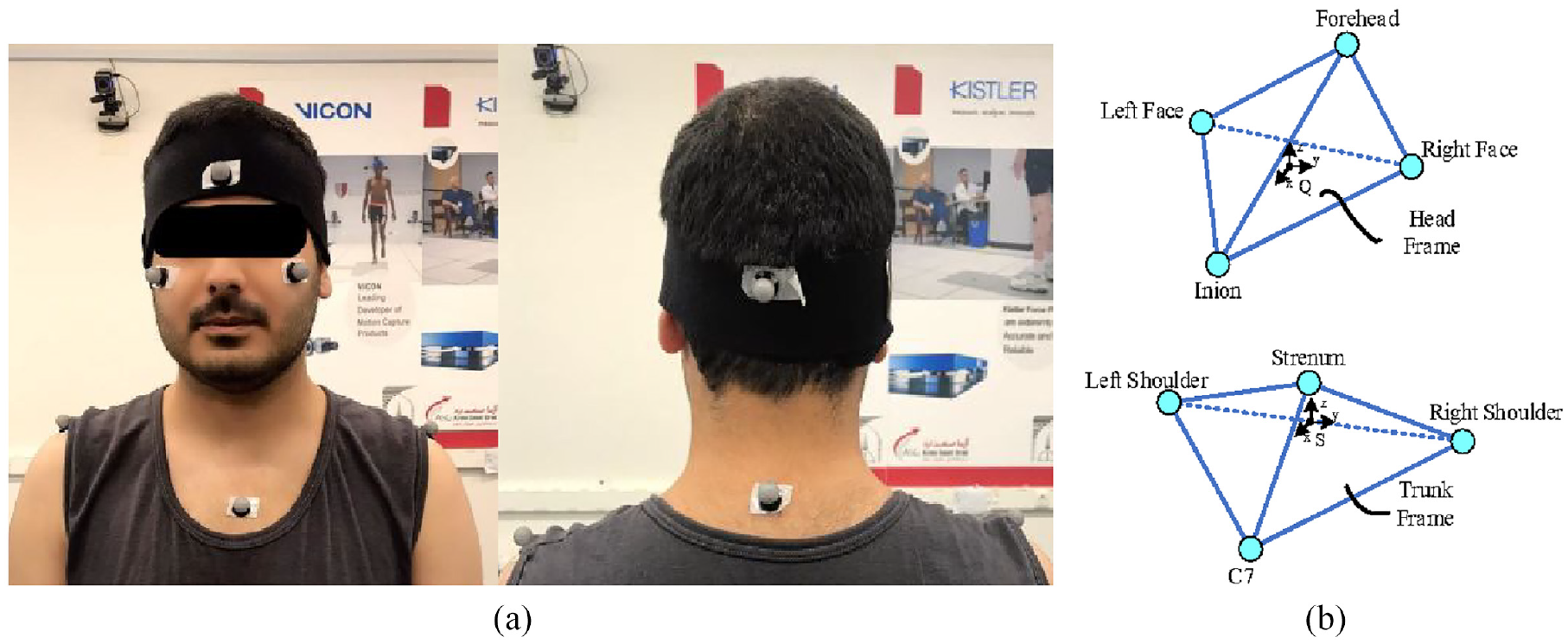
(a) Markers placement on head and shoulder and (b) head and shoulder frames considering markers locations.
Using markers, the head motion was computed related to the trunk. The human head has six degrees of freedom, and only three of these can be precisely satisfied by the proposed 3 DOF mechanism. Considering the extensive range of rotation in comparison to the small translation of the head, the objective of the optimization is to identify geometric parameters that can be used to construct a device that can accommodate head rotations while minimizing translational errors relative to the trunk. As a design feature, it is intended to be symmetric about the sagittal plane, leading to the optimization of fewer parameters.
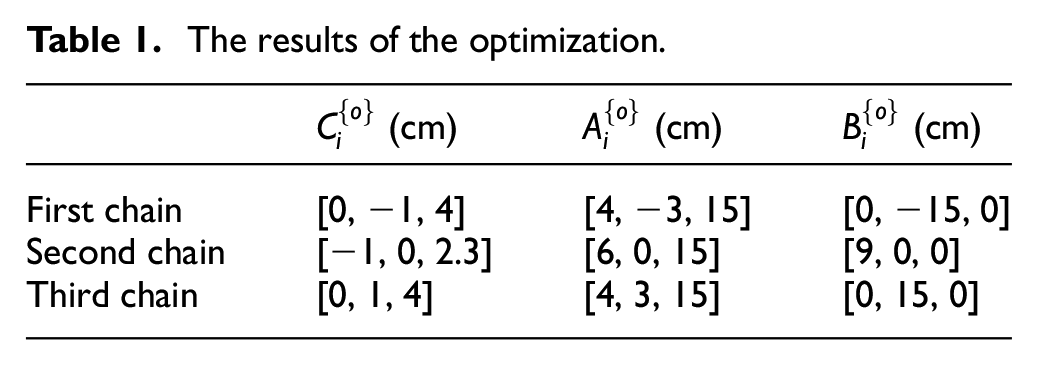
Previously, it was mentioned that the three distinct spheres have a center at point Ci, which is connected to the end-effector at point Ai by a constant distance ri. These spheres should be such that they involve the head movements space. Thus, a key point of mechanism designing is to find the Ci, Ai coordinates 22 in trunk (base) space and head (end-effector) space such that the distance between the two varies minimally during the recorded motion. The genetic algorithm method was used to find the optimum solution. In the optimization, a possible location of Ai is randomly selected in the moving frame Q within a search range. The location of Ci fixed in the static frame O is searched randomly such that the deviation of the distance between the two points, Ai and Ci, is minimized. Therefore, the cost function here is

where
The results of the optimization.
Geometric optimization
In this section, after finding the position of Ai and Ci points, the mechanism’s geometric parameters, for example, the length of

Which
Here we use the inverse of the condition number to have a value between zero and 1, so the objective function is turned to

Matlab (Mathworks, 2020B) is used as the platform for computation. Based on the objective function and data volume, the optimization runs for 10,000 iterations. After the location of the Mi point was found in each chain, the length of
Simulation
Figure 3 depicts the simulation model representing the selected parameters. It is evident that the intersecting points Ci do not coincide, leading to both rotation and translation of the end-effector. After simulating the optimal design of the robot using SimMechanic (MATLAB) and solving forward kinematics, the overall translational error for all three motions was calculated as x = 2.1 ± 2.4 mm, y = 2.0 ± 2.9 mm, and z = 1.7 ± 2.7 mm. This design enables a range of rotations up to +40°/−30° in the mid-sagittal plane, ±30° in the frontal plane, and ±68° in the horizontal plane.
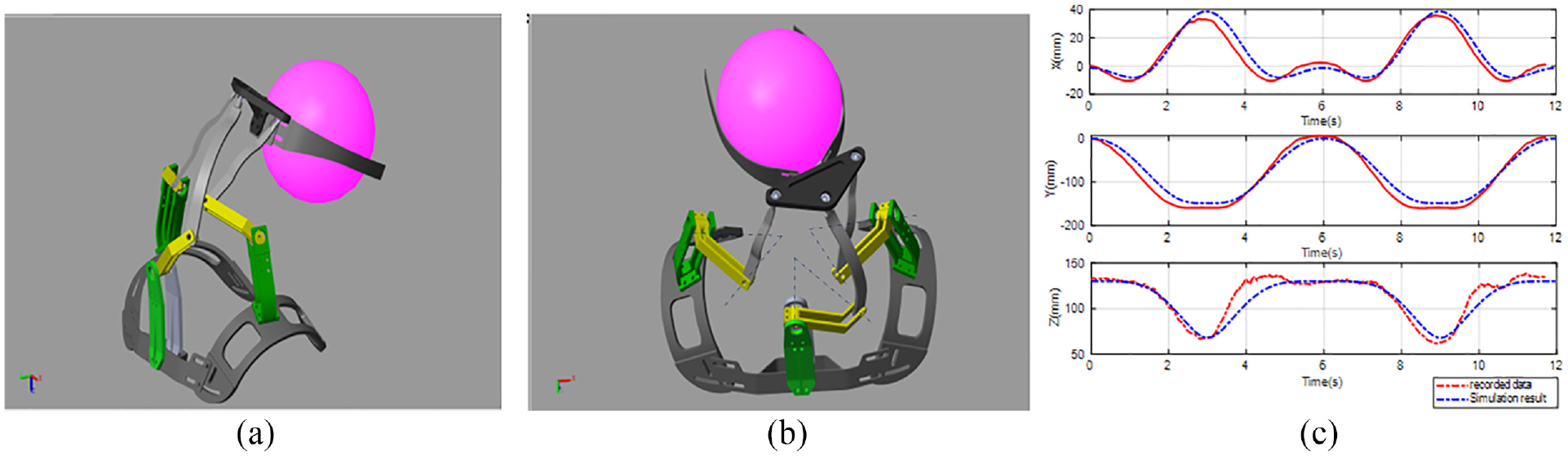
Simulation of robot’s motion in Simscape: (a) robot performs flexion-extension, (b) rotation motion of the robot, and (c) flexion translation motion in recorded head data and simulation result.
The simulation results demonstrate the feasibility of designing a wearable system that can achieve a significant range of head rotations while minimizing translational motion using the proposed mechanism. It should be noted that due to the placement of the mechanism’s linkages behind and to the side of the neck, the range of backward extension is smaller compared to forward flexion.
Physical design
After optimization, the entire model was designed with attention to details such as geometric links, joints and connections, and the placement of servomotors, taking into consideration the space between the head and shoulder. Figure 4 illustrates both the computer model and the prototype of the robot structure.
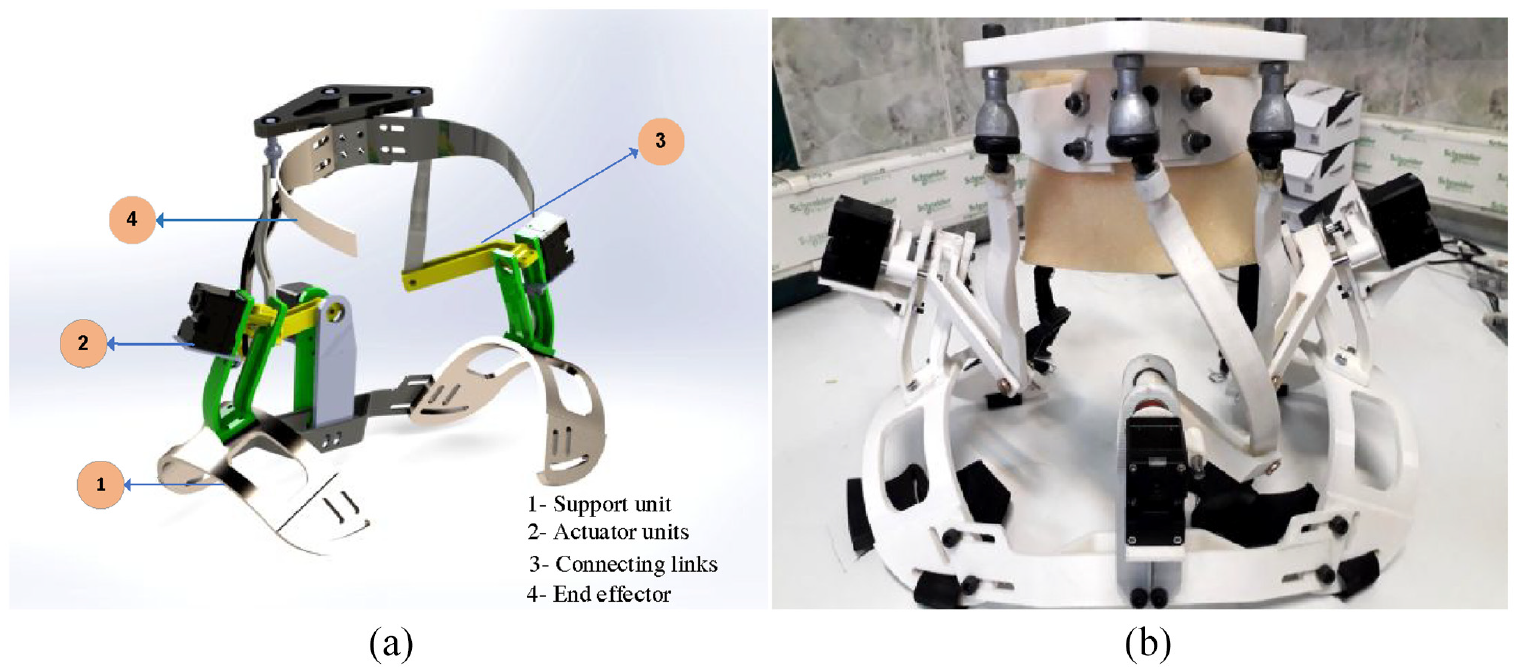
(a) A robot’s computer model and (b) the physical model of the system.
The robot system comprises a bottom support unit, chains with different length links, and a mobile platform with a strap and headband for fixation on the head. In Figure 4(a), section 1 represents the support unit, which serves as the base of the robot structure and attaches to the shoulder using a strap. The actuator units, mounted on bases fixed on the support unit with bolts, are shown in section 2. The bottom support unit is connected to the end-effector through chains that consist of links and joints, as depicted in section 3. Each chain is composed of an RRS linkage. The placement of the revolute joints in the robot model was determined based on the optimization results. Various factors, including weight, strength, and range of motion, were taken into account during the design of the linkage.
All parts of the robot were manufactured using a 3D printer (Quantum3D), with PLA plastic chosen as the material, Figure 4(b). (All parts were made at AMIC lab, Tarbiat Modares University, Tehran, Iran).
Control system
In the robot-assisted rehabilitation exercise, the passive training that controls the trajectory tracking is the most basic and simple training. It is particularly suitable for patients with no motor function in their muscles. 39 However, the cooperative training mode has better therapeutic outcomes.33,40 In this mode, Compliance control can be essential in the interaction between patients and robots. Training becomes more comfortable and safer using compliance control and allows for more active engagement for improved rehabilitation. One of the compliance control branches is impedance control, which explains the dynamic relation between position and force. 41 Impedance control can control motion and contact forces simultaneously by properly interacting with a manipulator and its environment. Impedance control does not need precise details of the exterior environment compared to hybrid force and position control, and the safety of human-robot interaction can be guaranteed. Thus, this control strategy has been implemented in robot-assisted rehabilitation.42,43 The paper presents a compliance control strategy to assist patients in achieving desired training and human-robot interaction with cooperative treatment. It consists of a two-level trajectory tracking control, as depicted in Figure 5. A closed loop with an embedded torque controller was used at the low level to control the desired torque from impedance output. The high-level controller gains the interaction torque based on the desired impedance and the error between the desired trajectory and the actual position, as measured from the servomotor encoder. The desired impedance in the joint space is defined as follows


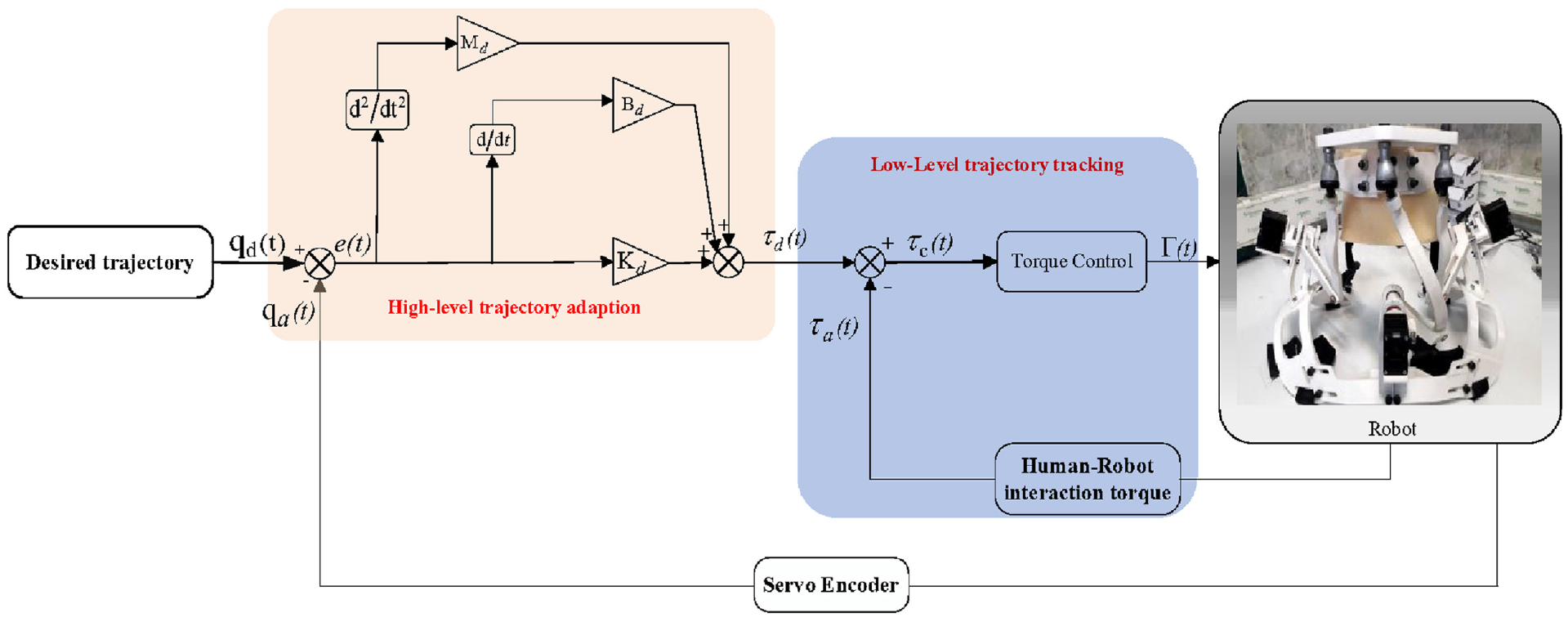
The control diagram of the system.

Where

Here, the coefficients
The servo motor has the embedded control torque mode and can control torque automatically. The command torque delivered to the servo is the same equation (7). Therefore, with the placement of equation (6) in equation (7), and considering human-robot interaction torque, we have

Where
Wearability
The robot was evaluated through a human experiment. This experiment aims to determine how the head rotation range changes when the robot is worn. The robot’s range of motion (ROM) was calculated and compared to the head movements of the human recorded with the motion capture (VICON camera) system data. With an embedded encoder of servomotors, the position of the joint was calculated. Servomotors were turned off, but they moved with the subject and measured the position of the joints. A healthy adult subject was asked to give three anatomical movements of the head by wearing the robot. The movements were performed in two cycles. The head orientation and translation were calculated using this data and solving the forward kinematic through Simulink. These data were compared with the human head data that was gained with a motion capture system.
Results
This robot is designed to achieve the desired spatial head rotation while having small errors in translation. It is thus important to evaluate the extent of changes in head position due to the structure of this robot when performing different head rotations. The reference point in the head frame is selected to be point Q in Figure 1. For example, the result of lateral bending motion with consideration of head angles in the x-y-z Euler sequence is shown in Figure 6(a), while the translation motion of the end-effector in the x-y-z directions is shown in Figure 6(b). Upon achieving certain head rotations allowed by the robot, the position of the participant’s head slightly differed from the position during natural movement. The average deviation of the change of the head position under two conditions, with and without the robot, are 4.64 ± 2.98 mm for flexion/extension, 4.53 ± 3.05 mm for lateral bending, and 4.14 ± 3.24 mm for axial rotation.
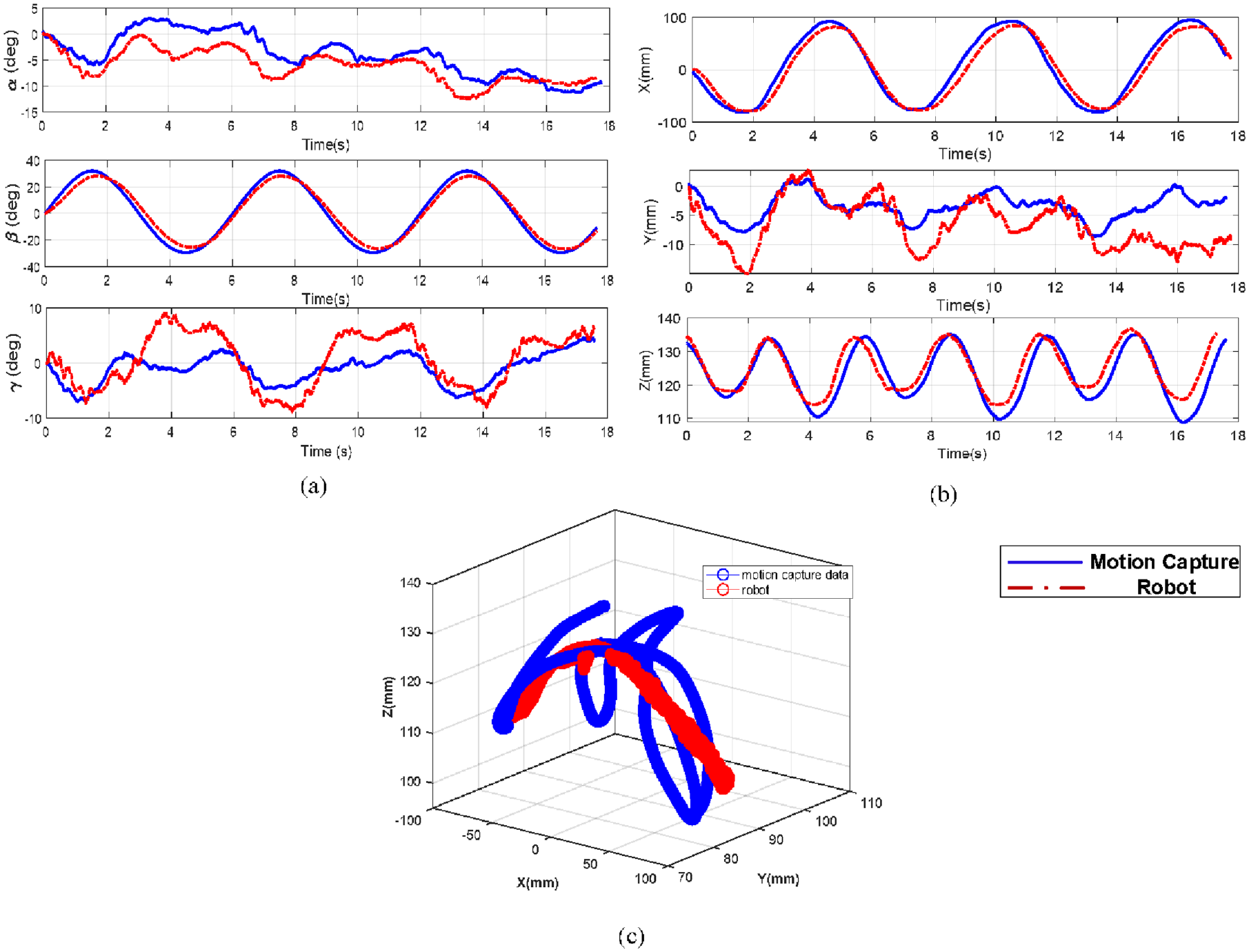
Comparing head angles and movements during lateral bending gained by motion capture system and robot: (a) head angle comparison in x-y-z sequence, (b) head movements in x, y, and z directions, and (c) isometric view of head motion.
After the subject performed all of the motions correctly, the ROM of the robot in three anatomical planes was calculated. As indicated in Figure 7, the range of the head rotations allowed by this robot are 70.7% in flexion-extension, 99.6% in lateral bending, and 84.3% in rotation. Therefore, a person wearing this robot can achieve approximately 85% of his natural head rotations. Due to manufacturing errors in the robot structure, the robot’s movements are not symmetric, as seen in the rotational movement in Figure 7.
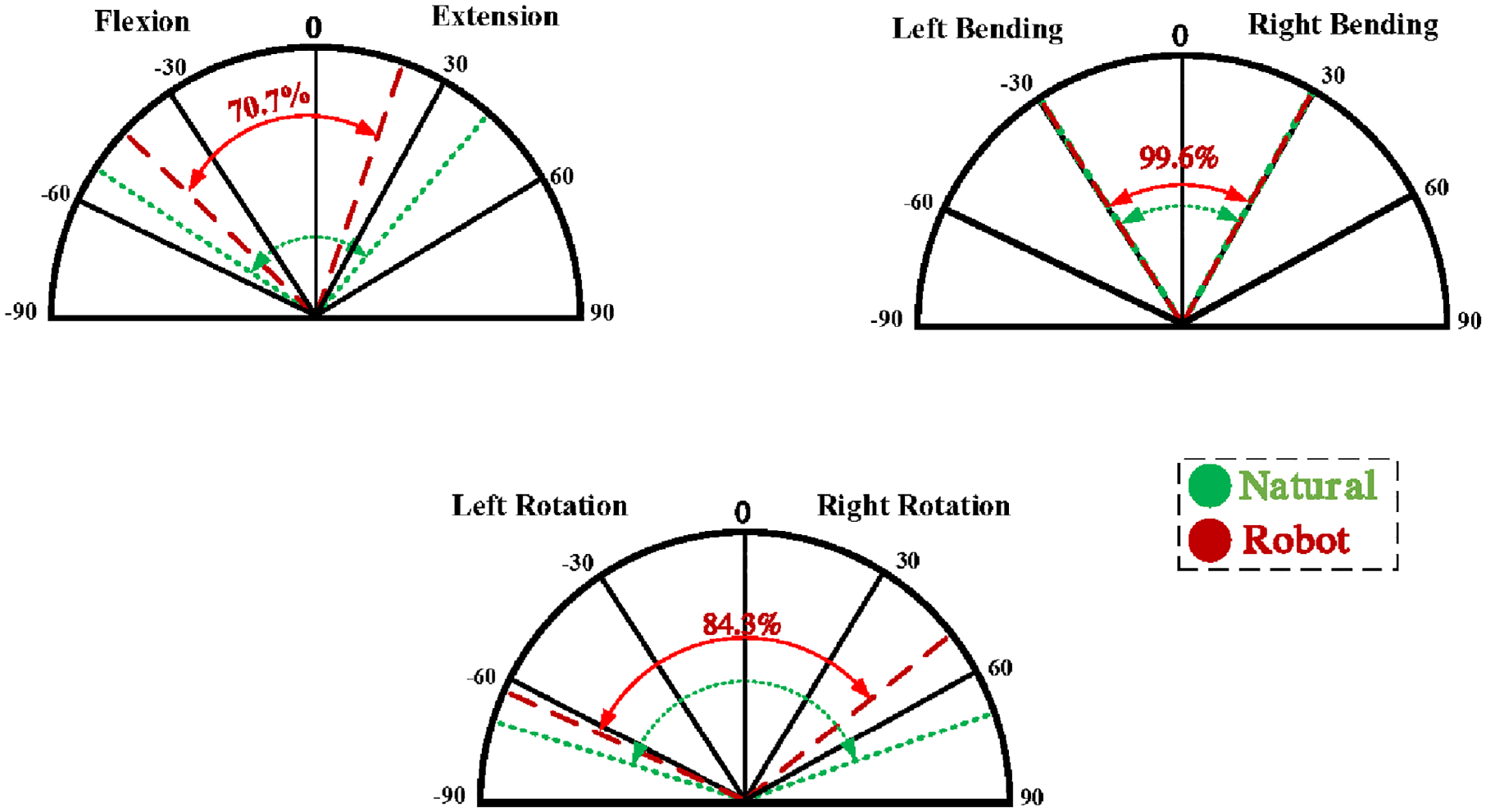
The robot’s range of motion in three anatomic planes of head-neck.
Human study
Human tests were conducted to evaluate the robot’s assistant capabilities in head movement training.
Ten healthy subjects were recruited to participate in the experiment in our laboratory (characteristics are given in Table 2). The study protocol was approved by the Institutional Review Board (IRB) at Tarbiat Modares University, with protocol number IRB2022-5067. Approval was obtained on 10 February 2022. All participants provided informed consent before participating in the study.
The subjects’ characteristics.
Methods
The experiment aimed to evaluate the robot’s effectiveness in rehabilitation training using the compliance control method. Two conditions, active and passive, were considered. In the passive condition, the subject wore the robot and performed the motion under the guidance of a physiotherapist. The robot’s servo motor was turned off, and the encoder collected the position of joints while the subject received visual feedback from the physiotherapist. In the active condition, the robot with compliance control assisted the subject in moving their head. To familiarize the subject with the robot and assess initial performance, a pilot study was conducted. In this study, the physiotherapist helped the subject move their head smoothly and correctly. After a 1-min rest, two training trials and a post-evaluation session were performed. Each training trial and post-evaluation session lasted for 30 s, and a 1-min break was provided between sessions to prevent muscle fatigue. The desired trajectory for the head movement was chosen as lateral bending, which was coupled with rotational motion. The trajectory was designed as a sinusoidal function with a frequency of 0.16 Hz and an amplitude of 30°. At the start, the head was in the right neutral position, and during the movement, it moved away from the neutral position and then returned to the initial position. During the experiments, surface electromyography (EMG) signals were collected to measure muscle activity. EMG electrodes were placed on both sides of the splenius capitis (SC) muscle in the neck (Figure 8(a)). Prior to electrode placement, the skin was cleaned and shaved following standard procedures for surface electromyography. After preparing the electrodes, the robot was mounted on the subject’s shoulder and aligned in the neutral configuration (Figure 8(b) and (c)).
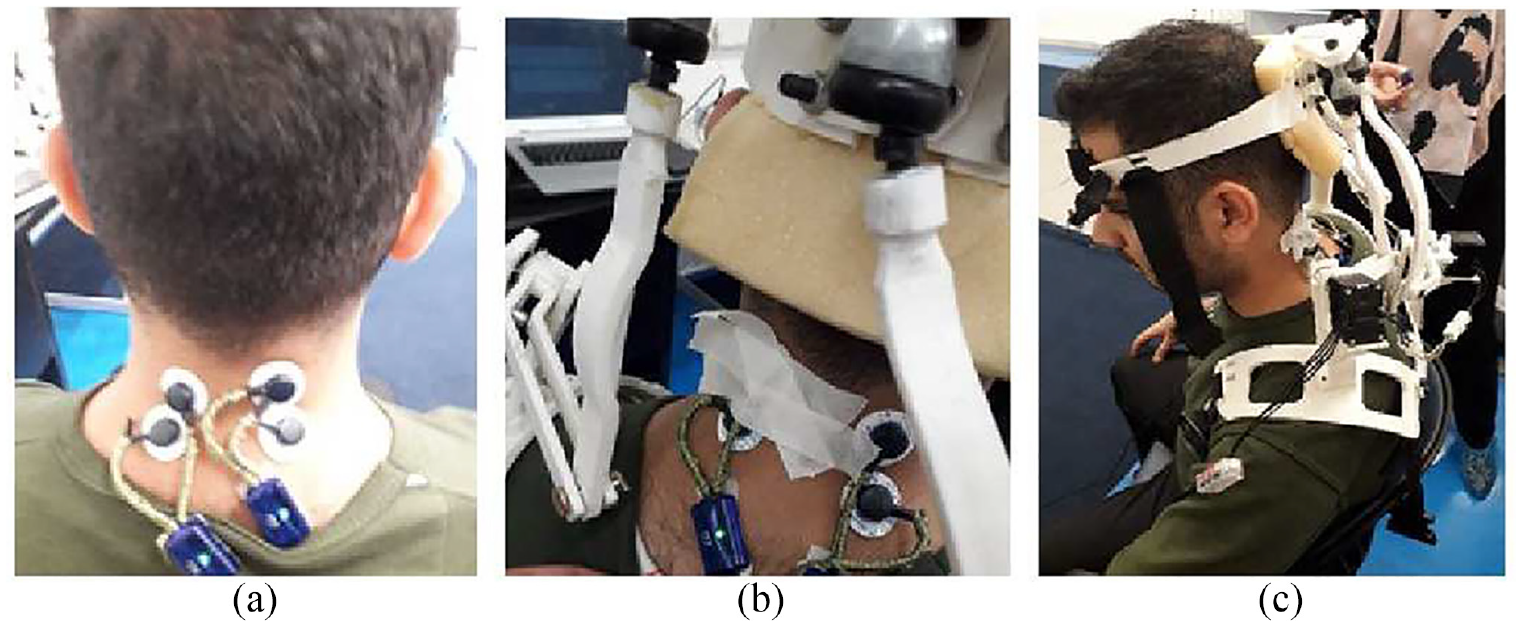
The experiment of a subject: (a) Electrode placement on muscles, (b) robot mounted on the shoulders of the subject, and (c) lateral bending movement under physiotherapist supervisor.
Data processing
The kinematic parameter, the position of the joints, was considered to check the robot’s performance in two conditions. With the position of the joints, the head angles represented by the x-y-z Euler sequences were calculated from the forward kinematic in Simulink. Here we used the RMS error of head angles, defined as the difference between desired and actual angles of the end-effector.
The EMG signals were recorded wirelessly (Myon aktos, Switzerland), sampled at 2048 Hz by the sEMG signals acquisition system, and synchronized. In this study, raw surface EMG signals were bandpass filtered by a fourth-order Butterworth filter with cut-off frequencies of 30–450 Hz and rectified. RMS of the EMG signal was computed with a window size of 500 ms, and finally, its normalization with the maximum voluntary isometric contraction (MVIC) method was extracted. To determine the coordination of the muscles, onset times of EMG were used during a movement cycle. Data recording of EMG was synchronized using accelerometers with a sampling frequency of 0.005 ms. The subjects’ head front and physiotherapist’s hands were fitted with accelerometers. Upon the physiotherapist’s command and the start of the subjects’ movement, accelerometers sent signals to the acquisition system device to detect the onset of EMGs. The time difference between these two moments was defined as the onset time.
Using a two-way analysis of variance (ANOVA) with the Welch correction, we investigated the impact of two factors: the conditions (passive and active) and the trials (training and post-evaluation) on each outcome variable, namely mean angle error, muscle activity levels, and onset times of electromyography (EMG) signals. To further examine the differences between groups, post-hoc analysis was conducted using Tukey’s method.
Results
Representative result
In this section, we present a representative example of the results obtained from the participants. In the passive condition, when the subject performed lateral bending motions, there were errors observed in other planes as well. Figure 9(a) shows that the coupled error during the trial training session was significant. After the post-evaluation session, the errors in flexion and rotation were relatively large as well (17.34 ± 0.5 and 11.74 ± 0.23, respectively).
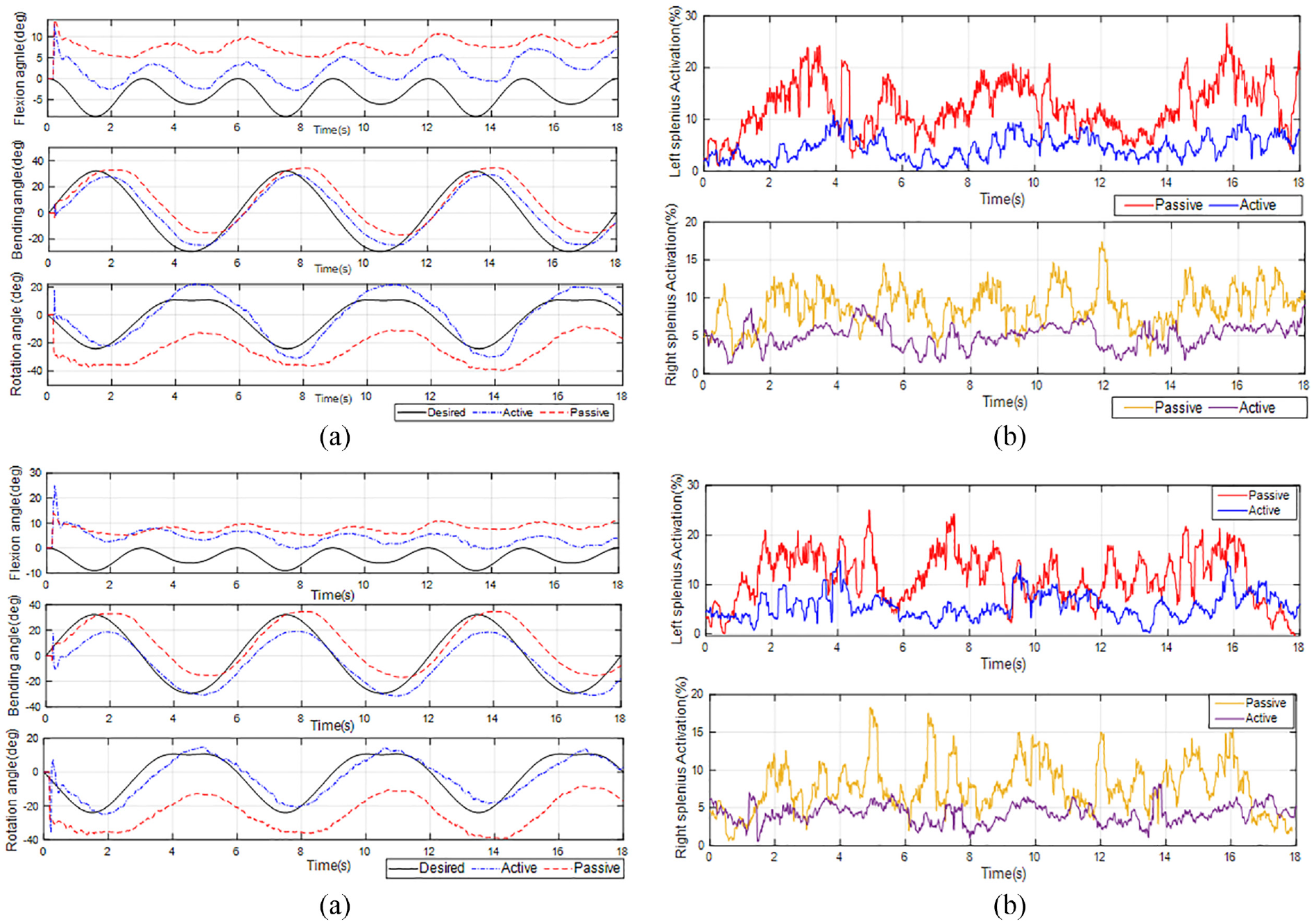
Results of the second subject in (a) head angle error in two conditions of active and passive in trial training, (b) muscle activity percentage in both left and right splenius capitis in the training, (c) head angle error in two conditions of active and passive in post-evaluation session, and (d) muscle activity percentage in both left and right splenius capitis in the post-evaluation.
In the active state, the kinematic data of the bending error during the trial training session was similar to that of the post-evaluation. However, as depicted in Figure 9(c), it is evident that the coupled error was significantly reduced in both sessions. Additionally, with the robot assistant mode, the rotation error slightly decreased in the post-evaluation (2 ± 0.05). Overall, after the trial training to post-evaluation, the root mean square (RMS) error decreased to 9.5 ± 1.
Figure 9(b) and (d) display the percentage of activity in the splenius capitis muscles. In both sessions, when the subject received assisted-as-needed force from the robot, the activity level of the muscles decreased. Although the activity range of the left muscle was slightly higher than that of the right muscle, the specific pattern of splenius capitis activity was evident in both conditions. The proximity of the muscle positions, as shown in Figure 8, results in the co-activation of both muscles when the subject turns their head to one side. According to Figure 9(b) and (d), both muscles exhibit a similar pattern when the head moves from the right to the left. This is because both muscles need to work together to move the head in a particular direction. When the head is turned to one side, both muscles contract simultaneously to produce the desired movement, leading to the observed co-activation. In both cases, the specific pattern of splenius capitis activity is evident. However, the mean muscle activity level is approximately 10% lower in the active state compared to the passive state. The onset times of the splenius capitis muscles slightly changed after training in the active condition. Overall, the activation of the splenius capitis was not significantly affected by the sessions, and after training in the active state, the magnitude of splenius capitis activation remained within the same range.
Group results
Figure 10 depicts the average performance of the robot in terms of muscle activity levels, while Figure 11 illustrates the mean angle error.
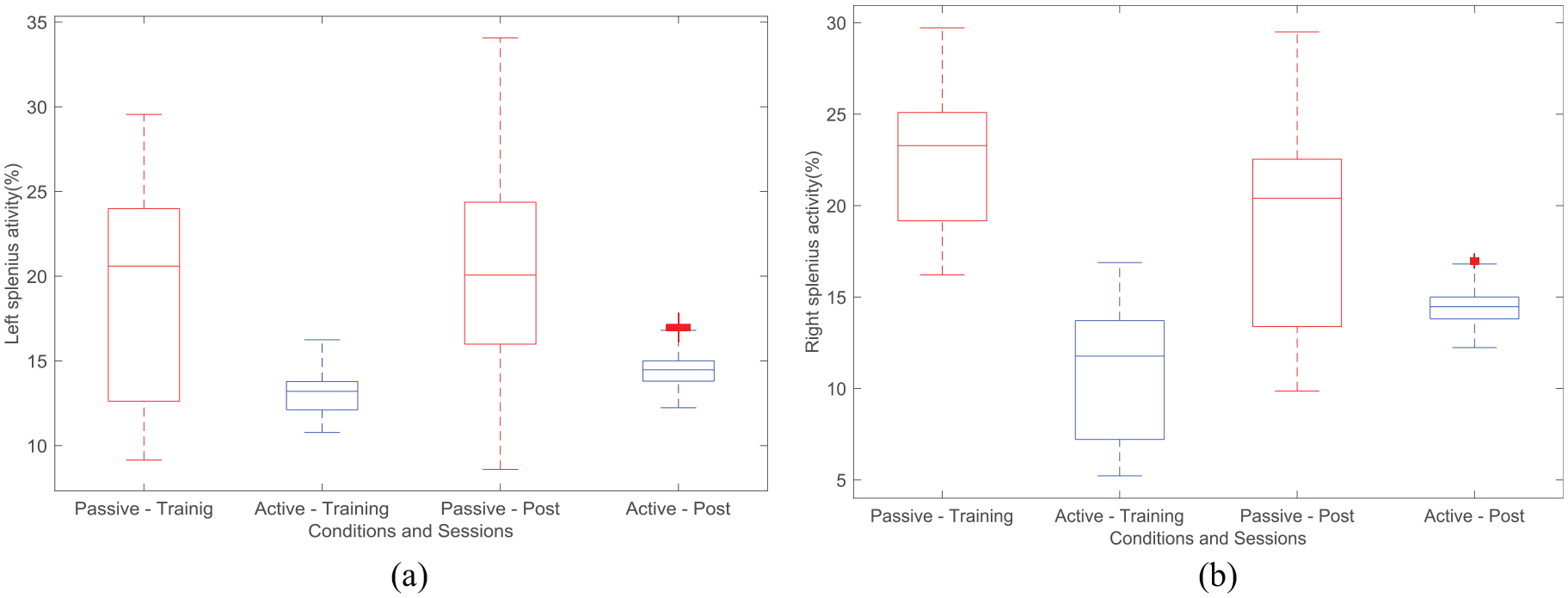
Comparison of average Normalized Electromyography (EMG) Data of : (a) right Splenius Capitis Muscle, and (b) left Splenius Capitis Muscle in both conditions and sessions.
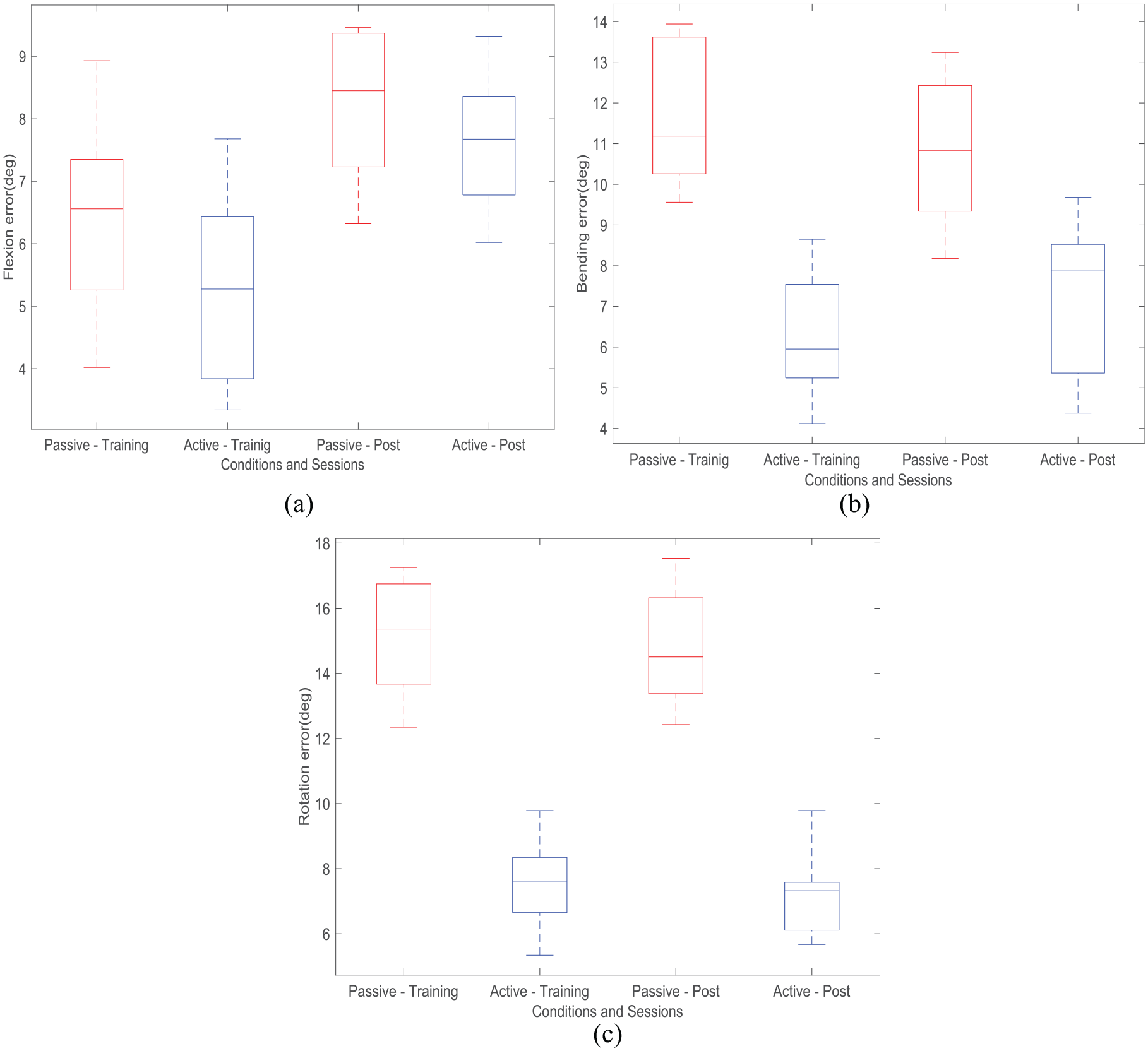
Average Root Mean Square (RMS) error of head angles in lateral bending motion, represented in X-Y-Z Euler sequences, with (a) flexion error, (b) bending error, and (c) rotation error. The data is presented for both passive and active conditions, across trial training and post-evaluation sessions.
The analysis of muscle activity levels revealed that the average normalized values of the muscles were significantly influenced by the conditions (active and passive) (p < 0.05). However, no significant impact was observed for the sessions (trial and post-evaluation) (p > 0.05) (Figure 10). Specifically, in the active condition, the mean normalized values were lower compared to the passive condition. Notably, the mean normalized values were not affected by the specific trial or post-evaluation sessions. For instance, in Figure 10(b), the average normalized of the right muscle during the trial training was higher to that of the post-evaluation in the passive condition. However, in the active condition, the value increased during the post-evaluation session. Overall, the conditions significantly influenced the mean normalized values (Figure 10), whereas the sessions did not exhibit a consistent pattern (p > 0.05).
Regarding the mean angle error, both the conditions and sessions demonstrated significant effects (p < 0.05) (Figure 11). In the case of flexion, both conditions (passive and active) significantly reduced the mean error compared to the baseline (p < 0.05). However, a significant increase in error was observed between the sessions (p < 0.05). Notably, the bending motion demonstrated a considerable influence on the conditions (p < 0.05), despite a slight increase observed in the active condition during the post-evaluation session. Trial training conducted under active conditions resulted in significantly lower rotational errors (p < 0.05) compared to trials conducted with physiotherapist assistance. In general, there were no interactive effects of both condition and session groups on the mean angle error (p > 0.05). Although some participants displayed changes in muscle electromyography activity patterns, there was no correlation between the conditions and sessions in terms of the onset times of muscle EMG (p > 0.05).
Discussion
This article aims to develop an assistive device specifically designed to aid patients with neck disorders in regaining dynamic head-neck movement. The device incorporates essential features that address the unique needs of individuals with neck-related impairments to gain head-neck movements, empowering patients to regain strength and mobility, and making the rehabilitation process easier for both the physiotherapist and the patient. Our design was inspired by a parallel structure which is modified to accomplish neutral head range motion. Our primary focus was on an optimization structure that could cover most head motions. Utilizing the condition number index, the optimal robot’s structure was found through the genetic algorithm method. After the simulation of the robot and finding its motion results, the robot’s structure was developed through a 3D print device. When comparing the range of neutral head movement based on human data with the head movement range achieved by our robot, we observed that the robot’s wearability enables a substantial range of head motion. In comparison to previous work, 22 we found that our robot’s structure, derived from optimization results, allows for a greater range of head movements, approximately 85%, whereas the previous work achieved only around 70%. Additionally, our optimization process resulted in a structure that exhibited the lowest translational error during head translation movements. It is observed that there is an asymmetric range movement in the robot’s rotational movement, which stems from lower fabrication accuracy or even deformation of the mechanical component. As outlined in the compliance control plan, the assist-as-needed method was incorporated as well as ensuring safety in an environment similar to that of a clinical trial. We used a human study to evaluate the performance and ability of the robot in assisting some healthy subjects by considering the head kinematic parameter and the surface EMGs of the muscles during a simple single-plane movement. Decreasing coupling error, rotational and bending angles error when the subject is using the robot, as it is evaluated in Zhang et al., 44 expresses a movement with higher accuracy and justifies the robot’s role in rehabilitation instead of human assistance. It is expected that the head trajectory will be relatively similar between healthy subjects and patients because the robot guides the movement of the head.
During the test, we observed EMG signals from splenius capitis muscles reduction in muscle activities when subjects wore the robot. According to Zhang and Agrawal 23 and Xiao et al. 45 reduction in splenius capitis muscle’s activities states that the robot supplies desired force to the patient, which they can perform tasks with less effort.
Clinical studies have demonstrated that robotic devices capable of providing appropriate interaction and assistance on the upper limb significantly improve rehabilitation outcomes, particularly for individuals with severe cases. These devices enhance the range of motion of disabled limbs during execution, thereby contributing to more effective rehabilitation.46–48
Conclusions
This paper presents the development of a wearable system to rehabilitate neck-impaired patients. Despite the conventional process of head-neck rehabilitation, the robot can be practical to use in varying environments and conditions due to its structural design and components. We checked the performance of the robot with a healthy subject. It was obtained that the robot can provide about 85% of the neutral head-neck movement. An experiment was conducted using the compliance control method to evaluate the robot’s assistant ability. As a result of the experiment, a kinematic parameter known as head angle error was measured. In addition, EMG signals were used to show the muscle power level in two active and passive conditions. The results show that the mean absolute head angle error was reduced when the robot helped the subject move. Bending and rotation angles error were reduced considerably with the robot, which means the robot with this compliance control method hinders the out-of-plane motion.
Furthermore, splenius capitis muscle activations significantly decreased in the active mode. It expresses robot can assist the subject during training and approves the theory that the users need less muscle power when they wear the robot.
To obtain more accurate and comprehensive results, future studies will involve larger participant groups and collect a greater amount of data. As this work represents a prototype, our evaluation was conducted with a small group of healthy subjects. However, these results provide valuable insights into the robot’s performance and reliability, aligning with other research studies. In future analyses, we aim to assess the relationship between our model and its application in clinical tests, incorporating assessments such as the Fugl-Meyer Assessment (FMA) and evaluating factors like movement speed and the involvement of different muscles, including the sternocleidomastoid. Furthermore, it will be essential to investigate the robot’s ability to effectively cooperate with patients and determine its overall effectiveness in a clinical setting.
Footnotes
Acknowledgements
This work was supported by the AMIC (Applied Mechatronic innovation center) lab at Tarbiat Modares University. Thanks to Professor Majid M. Moghaddam and Doctor Majid Sadedel for coworking and support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
All authors confirm that this study was performed according to the Ethics principles. There are no misconduct cases in this work, and they approve of the journal upholding the integrity of the scientific record.
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Consent for publication
The authors affirm that human research participants provided informed consent for the publication of the images in Figures 2 and ![]() .
.