
Abstract
Stroke is a leading cause of disability worldwide. In this paper, a novel robot-assisted rehabilitation system based on motor imagery electroencephalography (EEG) is developed for regular training of neurological rehabilitation for upper limb stroke patients. Firstly, three-dimensional animation was used to guide the patient image the upper limb movement and EEG signals were acquired by EEG amplifier. Secondly, eigenvectors were extracted by harmonic wavelet transform (HWT) and linear discriminant analysis (LDA) classifier was utilized to classify the pattern of the left and right upper limb motor imagery EEG signals. Finally, PC triggered the upper limb rehabilitation robot to perform motor therapy and gave the virtual feedback. Using this robot-assisted upper limb rehabilitation system, the patient's EEG of upper limb movement imagination is translated to control rehabilitation robot directly. Consequently, the proposed rehabilitation system can fully explore the patient's motivation and attention and directly facilitate upper limb post-stroke rehabilitation therapy. Experimental results on unimpaired participants were presented to demonstrate the feasibility of the rehabilitation system. Combining robot-assisted training with motor imagery-based BCI will make future rehabilitation therapy more effective. Clinical testing is still required for further proving this assumption.
Introduction
Stroke remains a leading cause of adult disability all over the world. In the United States, each year there are more than 795,000 people experiencing a new or recurrent stroke [1]. Approximately 80% of acute stroke survivors lose arm and hand movement skills. Although the optimal therapy for patients who suffer from stroke is still a point of discussion, one theory is that patients will recover better and faster when having intensive physiotherapy directly after the accident and the first 3 to 6 months are the most crucial periods as this is the period of maximal neurological recovery. Differential rates of recovery occur for various types of impairments. In general, motor functions (mobility, walking, upper limb function, hand function, activities of daily living (ADL)) recover faster than cognitive or language impairments which may recover over 12 months [2].
Unfortunately, traditional stroke rehabilitation therapy is labor-intensive and requires one to one manual interactions with therapists. Moreover, hospitals and therapists become insufficient to support these patients suffering form stroke. In addition, the evaluation of patient's performance and progress is usually difficult. In recent years, there is a rapid growth in the use of robots for rehabilitation therapy. Many groups have developed robot-assisted rehabilitation therapy systems, such as MIT-MANUS [3], MIME [4], ARM Guide [5] and Bi-Manu-Track [6]. The MIT-MANUS, which allows unrestricted movements of the shoulder and elbow joints, and the MIME, which enables the bilateral practice of a 3-DoF shoulder-elbow movement, show that the recovery can be improved through additional therapy aided by robot technology. The ARM Guide, which assists reaching in a straight-line trajectory, and the Bi-Manu-Track, which is designed to train distal arm movements by practicing bilateral elbow pronation and supination as well as wrist flexion and extension in a mirror or parallel fashion, show also use of simple devices makes possible intensive training for post-stroke patients with positive results.
In addition, many different methods utilizing electromyographic (EMG) signals to control robots have been proposed for rehabilitation therapy. For example, Cheng et al. developed an assistive torque system which utilizes homogenic surface EMG signal to improve the elbow torque capability of stroke patients [7]. The assistive torque provided by the system is proportional to the difference between the weighted biceps and triceps EMG signals. Dipietro et al. developed an EMG-based rehabilitation training system for the upper limb movement of the stroke patients [8]. In this system, the onset of the patient's attempt to move is detected by monitoring EMG signals in selected muscles. In Ref. [9], a myoelectrically controlled robotic system was designed to assist elbow training in a horizontal plane with intention involvement for people after stroke. The system could provide continuous assistance in extension torque, which was proportional to the amplitude of the subject's EMG signal from the triceps, and enabled the subjects to perform rehabilitation training beyond their initial voluntary range-of motion.
As compared to the traditional rehabilitation, robot-assisted rehabilitation can provide high-intensity, repetitive, and task-specific therapy for body parts impaired by neurological conditions. Also, it can track the patient's progress and make recommendations to the therapists whenever necessary.
Although many studies have demonstrated the advantages and efficacy of existing robotic rehabilitation systems for assessing and treating motor impairments in both the upper and lower extremities, there is no direct communication between the patient's mind or motor volitional thinking and the rehabilitation system. Even though some sensors are used to detect the patient's weak movement, it never knows when and how the patient desires to move. In most cases, the patient can only passively follow the predefined program, which may not fully explore the patient's motor initiatives and potential or attention processes.
Brain-computer interface (BCI) provides a new communication or control channel that does not depend on brain's normal output of peripheral nerves and muscles [10]. It enables people to control the environment using only thoughts or brain's activity. In recent years, BCI research has explored many applications in different fields: environmental control, communication and playing games. Wolpaw et al. developed a BCI system based on the variations of electroencephalography (EEG) rhythmic activity and the EEG signals were utilized to control the movement of a cursor on a computer screen [11]. In Ref. [12], a BCI-based humanoid robot was developed in order to locate and manipulate object. The ASPICE Project of Santa Lucia Fundation in Rome, Italy controlled an AIBO robot of Sony through a BCI interface [13]. Geng et al. designed an asynchronous BCI system allowing subjects control the robot to circumnavigate obstacles and reach small targets in separate rooms [14]. However, most studies in this field only consider replacing dysfunctional body parts by artificial actuators or controlling external device. Instead, noninvasive BCI systems can also be applicable to directly facilitate rehabilitation of body parts impaired by neurological conditions and show the most promise in practical rehabilitation therapy [15]. While robot-assisted rehabilitation plays an important role in rehabilitation after stroke, noninvasive BCI has also been shown to have a beneficial effect in stroke rehabilitation [16],[17]. Combining robot-assisted training with BCI can be expected to have a large impact on stroke rehabilitation, particularly for severely impaired stroke patients. Using the motor imagery EEG to trigger the robot to perform rehabilitation training may offer the following advantages.
It will allow the rehabilitation system to explore the patient's motor initiatives. It allows high-impaired patients to activate robot. Severely impaired stroke patients may not be able to produce sufficient movement or generate EMG signals to activate robot. It triggers the robot earlier than triggering based on kinemaitic or EMG signals. It may provide data critical to understand the processes of rehabilitation therapy.
Currently, the neural correlates of motor learning are mainly monitored by the following methods: EEG, magnetoencephalography (MEG), electrocorticography (ECoG) and functional magnetic resonance imaging (fMRI). Among these methods, the EEG is widely used in BCI research due to its inexpensiveness and non-invasiveness. From wax and wane oscillations of the brain, movement-related EEG components are mostly found in the mu (7–12Hz) and beta (18–25Hz) rhythms. These rhythms can display either an event-related desynchronization (ERD), which is an amplitude decrease or an event-related synchronization, which is an amplitude increase [18]. In relation to the movement, motor imagery is an internal reproduction of a specific motor action without any overt motor output. A number of studies suggest that motor imagery shares the same neural mechanisms with actual movement and practicing motor imagery should have an impact on motor learning performance [19].
The adult brain is capable of reorganizing itself by forming new neural connections between intact neurons throughout our lifetime. If one hemisphere of the brain is damaged, the intact hemisphere may take over some of its functions. The brain's reorganizing ability is commonly known as neuroplasticity. Neuroplasticity enables the neurons in the brain to compensate for injury and disease and to adjust their activities in response to new situations. By repeating learning, neuroplasticity can move the position of a given function form one location to another in the brain. Since stroke patients suffer from neurological damage, the portion of the brain that is responsible for generating ERD/ERS could be compromised.
In this work, an online robot-assisted upper limb rehabilitation system based on motor imagery EEG is designed, including hardware, software, feature extraction and classification algorithm, and rehabilitation robot. The rehabilitation system translates the mental imagination of upper limb movements into commands to trigger a rehabilitation robot to manipulate the affected upper limb in a similar way as during a physical therapy exercise. Combination of robot-assisted rehabilitation and motor imagery-based BCI will fully explore the patient's motor initiatives and guide the stroke patient to perform rehabilitation training effectively.
Overview of the rehabilitation robot
Fig. 1 shows the mechanical structure of the rehabilitation robot. Fig. 2(a), (b) and (c) are the three different operation modes of the rehabilitation robot. The first and second operation mode is designed for the purpose of performing upper limb rehabilitation training in horizontal and vertical plane, respectively. The third operation mode can be use to perform lower limb rehabilitation exercises for stroke patients. In this paper, only the first operation mode with passive recovery training is utilized.

Mechanical structure of the rehabilitation robot.
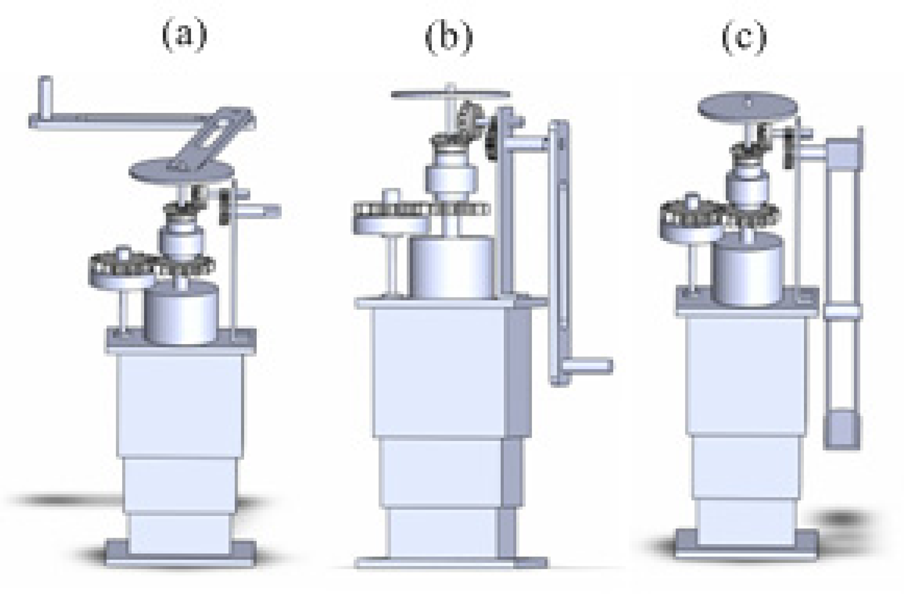
Three different operation modes of the rehabilitation robot. (a) and (b) are for the purpose of performing upper limb rehabilitation training in horizontal and vertical plane, respectively. (c) is for performing lower limb rehabilitation exercise.
Torque motor and magnetorheological (MR) damper are installed in parallel via straight gear. Torque motor is utilized in the mode of passive recovery training, and the MR damper is used in order to produce reliable and safe damping force in the mode of active recovery training. A MR damper is a damper filled with MR fluid, which has the ability to reversibly change from a free-flowing, linear viscous fluid to a semi-solid with controllable yield strength in milliseconds when exposed to a magnetic field [20]. MR damper offers highly reliable operation, which is very important in designing a robot-assisted rehabilitation training system, and can be viewed as fail-safe. Fig. 3 illustrates the architecture of a MR damper, which is a product from Lord Corporation. Besides, torque sensor is installed in series with the torque motor for the purpose of measuring the force between the arm of the stroke patients and the robot arm. Position sensor is mounted under the motor and connected with the shaft of the motor so as to measure the angle of arm rotation. According to the recommendations of the therapists, the length of the robot arm is 0.3 to 0.4 meters and the rotation angle of robot arm is −90° to +90°.

Magnetorheological damper (a) and its architecture (b).
The robot-assisted upper limb rehabilitation system manly includes the functions of online motor imagery EEG signal acquisition, online pattern recognition algorithm, and rehabilitation robot control. The hardware of the system consists of EEG amplifier with universal serial bus (USB) interface, PC, and rehabilitation robot (Fig. 4). The recording uses our specially-made EEG Amplifier and Ag/AgCl electrodes. Two differential inputs of the EEG Amplifier are used to measure signals over C3 and C4 according to the international 10–20 standard electrode placement. The electrode impedances are kept below 10kΩ. The EEG is sampled with 128Hz and band-pass filtered between 0.5 and 30Hz.
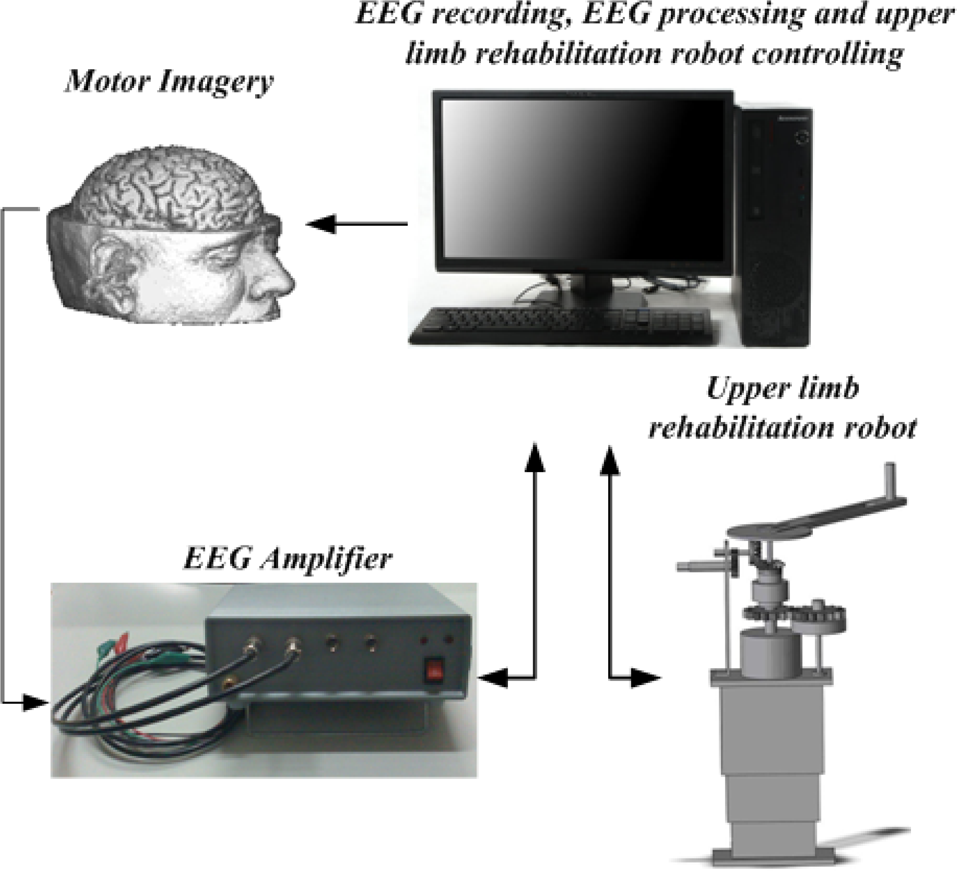
Robot-assisted upper limb rehabilitation system based on motor imagery EEG
Feature extraction based on harmonic wavelet transform
The harmonic wavelet transform (HWT), developed by Newland in 1993 [21]–[23], has been designed to achieve exact band separation in the frequency domain. Thus, it is suitable for extracting features from motor imagery EEG because it can be used to locate the frequency bands of interest.
Harmonic wavelets are orthogonal wavelets. In the frequency domain, the harmonic wavelets are simple structured as:

where m and n are real but are not necessarily integers. So the harmonic wavelets can be related to the ideal bandpass filter.
By taking the inverse Fourier transform of W m,n (ω), the time domain expression of the harmonic wavelet is obtained as:

where
If the harmonic wavelet is translated by a step k / {n − m), in which k is the translation parameter, a generalized expression that is centered at t = k / (n − m) with a bandwidth of
Based on the generalized expression, the HWT of a signal x(t) can be performed as:

Where *demotes complex conjugate and hwt(m,n,k) is the harmonic wavelet coefficient.
According to the frequency bands of alpha and beta rhythms, motor imagery related alpha and beta waves are extracted by harmonic wavelet transform. Fig. 5 together with Fig. 6 show alpha and beta waves extracted from EEG signals of C3 and C4 channel during left upper limb motor imagery, while Fig. 7 together with Fig. 8 illustrate alpha and beta waves extracted from EEG signals of C3 and C4 channel during right upper limb motor imagery. When the subject performs a left upper limb motor imagery, it is obvious that alpha and beta waves of channel C3 are enhanced while alpha and beta waves of channel C4 are suppressed. Conversely, when the subject perform a right upper limb motor imagery, it is clear that alpha and beta waves of channel C3 are suppressed while alpha and beta wave of channel C4 are enhanced. These results are consistent with the phenomenon of ERD and ERS which are caused by motor behavior or mental imagery [18]. These properties would be very useful features for pattern recognition of motor imagery EEG.
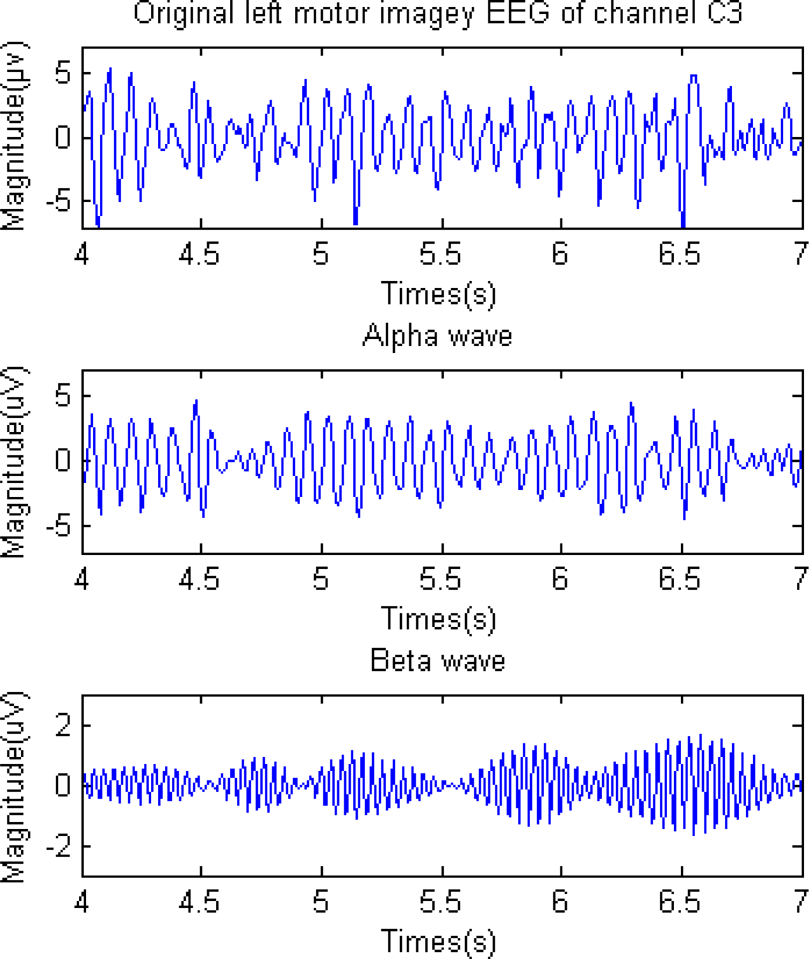
Alpha and beta waves extracted from an EEG signal of C3 channel during left upper limb motor imagery.

Alpha and beta waves extracted from an EEG signal of C4 channel during left upper limb motor imagery.
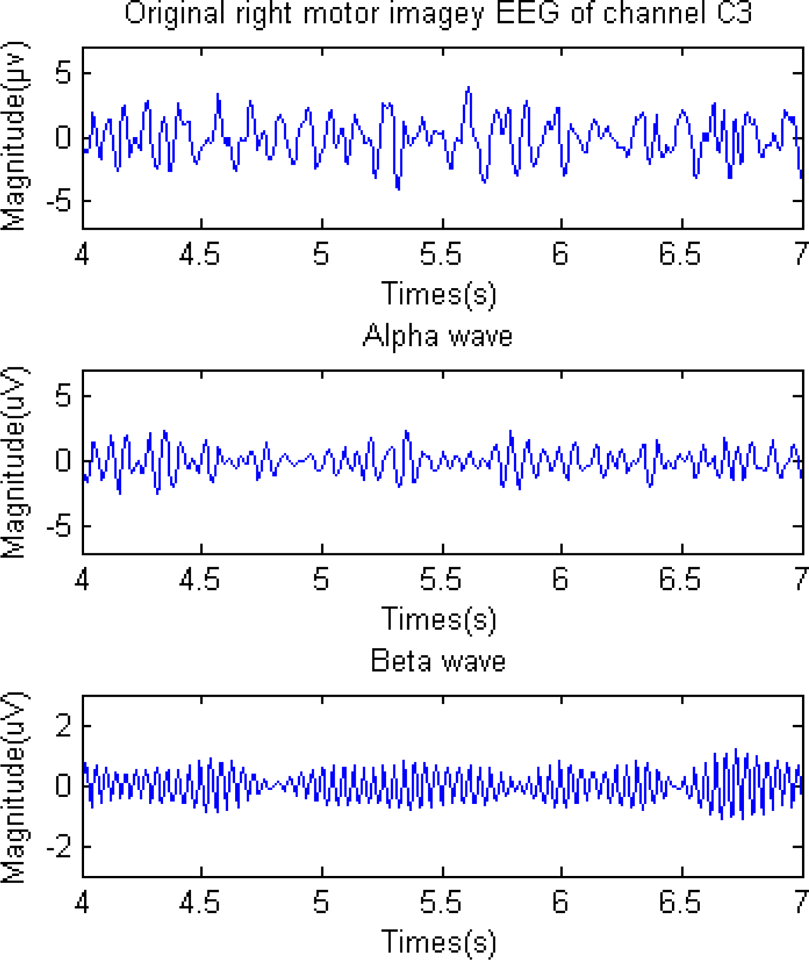
Alpha and beta waves extracted from an EEG signal of C3 channel during right upper limb motor imagery.
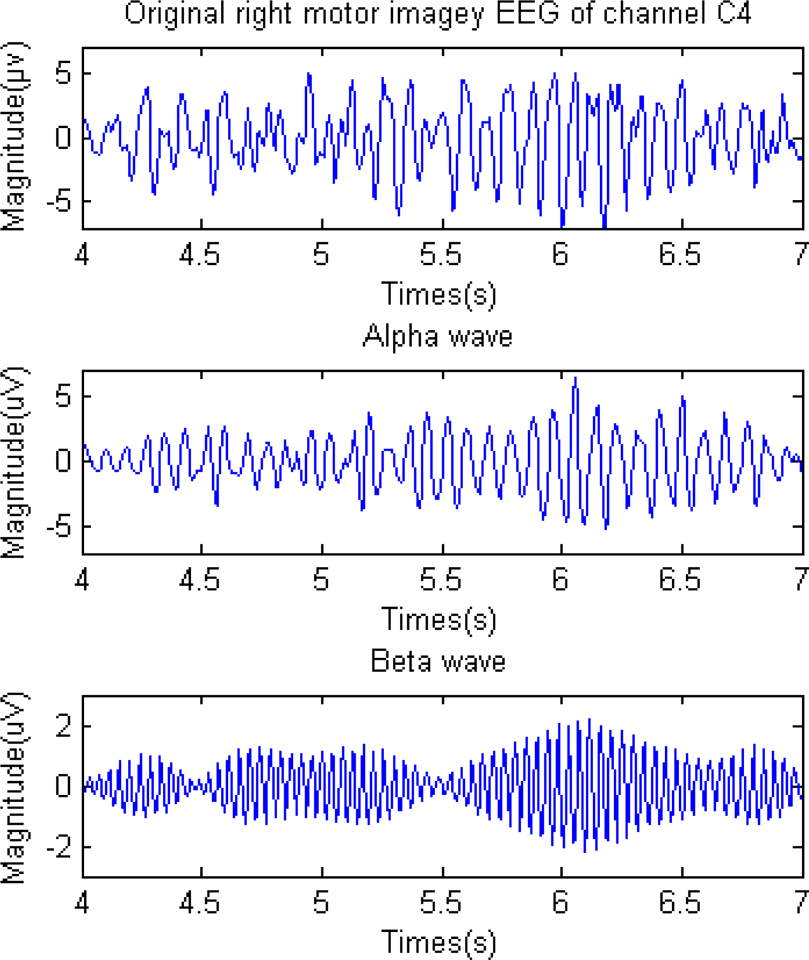
Alpha and beta waves extracted from an EEG signal of C4 channel during right upper limb motor imagery.
Statistics over the set of harmonic wavelet coefficients were computed for the purpose of reducing the total dimension of the feature vectors. Mean of the harmonic wavelet coefficients, standard deviation of the harmonic wavelet coefficients, and average power of the harmonic wavelet coefficients were used. These features represent the frequency distribution and the amount of changes in frequency distribution. Thus 6 statistical features of harmonic wavelet coefficients were extracted from alpha and beta bands for each channel, giving a total of 12 harmonic wavelet features for a motor imagery task.
Autoregressive model (AR) has been extensively used to model many electrophysiological signals. AR model is well suited for EEG for several reasons. Firstly, EEG is essentially comprised of the superposition of mass single unit activity through volume conduction, which can be considered as a filtered white noise process. This filtering of a white noise process is the basis for AR model and therefore it is a reasonable model for EEG. Secondly, EEG is highly non-stationary and must be analyzed using short time segments over which the data are presumed to be stationary. The spectral resolution of AR model is not explicitly limited by the length of the input process and therefore it is capable of providing superior resolution for short data segments [24].
EEG signal can be considered as the output of a linear filter driven by a white noise in quasi static approximation. This filter, referred to as AR, is a linear combination of the previous output itself. A zero-mean, stationary, autoregressive process of order p is given by

Where p is the model order, x(n) is the signal at the sampled point n, a p (i) are the AR coefficients and ε(n) is a zero-mean white noise. In application, the values of the a p (i) have to be estimated from the finite samples of data x(1), x(2), x(3), …, x(N).
The first important thing involved in using AR model is determining the optimal AR model order. The spectrum may exhibit spurious peaks when the model order is too high for the input process. On the contrary, an overly smooth spectrum results are obtained when the model order is too low to model the input process. Here order six was used based on the suggestions [25], [26].
Then, the Burg's method is used to estimate the AR coefficients. This method is more accurate and yields better resolution as compared to other methods such as Levison-Durbin as it uses the data points directly. Next, the AR coefficients were computed and six coefficients were got for each channel, giving a total of 12 AR coefficients features for a motor imagery task.
For a comparison of different classifiers, neural network (NN) classification method (offline), support vector machine (SVM) classification method (offline), and linear discriminate analysis (LDA) classification method (online) were selected to classify computed features into different categories that represented the left or right upper limb movement imagination. This section briefly introduces the NN, SVM and LDA classifiers.
NN models have achieved human-like performance over traditional artificial intelligence techniques. NN is an assembly of several artificial neurons which enable us to produce nonlinear decision boundaries [27]. In this paper, we focus on the most widely used NN for BCI, which is the multilayer perceptron (MLP).
The MLP is composed of several layers of neurons: an input layer, one or several hidden layers and an output layer [27]. The input layer has the same size of the input feature vector, the output layer has many neurons as classes to classify, and the neurons in hidden layers are determined empirically.
There are many training algorithms for MLP neural networks, such as gradient descent error backpropagation and gradient descent with adaptive learning rate backpropagation. A theoretical foundation of backpropagation can be found in [28]. Ln this paper, the training algorithm utilized is the gradient descent with momentum and adaptive learning rate backpropagation.
SVM is another tool used in BCI research for the classification. Using a kernel function, the SVM maps input vectors into a higher dimensional space [29]. Thus SVM is also called support vector networks. The output of SVM classifier can be computed by the following expression:

where {x i , y j } N i=1 are the training samples, a i are the Lagrangian multipliers obtained by solving a quadratic optimization problem, k(x i , x j ) is the kernel function, and b is the bias. The kernel generally used in BCI research is the Gaussian or radial basis function (RBF):
The corresponding SVM is known as Gaussian SVM or RBF SVM.
LDA is one of the most effective linear classification methods. This method maximizes the ratio of between-class variance to the within-class variance in any particular data set thereby guaranteeing maximal separability. As for the LDA method, feature vector X is classified by the following linear transformation:

Where w is the normal vector, and b is the threshold, w and b are determined by maximizing the ratio of between-class variance to with-class variance [30]. The between-class variance matrix is defined by:
Where u c is the mean of the entire training sample set, K is the number of classes, and u i represents the mean vector of the class i. The with-class variance matrix is defined by:
Where N i represents the number of samples with-class i.
If D(x) is larger than 0, x is assigned to class 1; if D(x) is smaller than 0, x is assigned to class 0. However, D(x) = 0 indicates all elements x are part of the separating hyperplane. In this study, NN and SVM method were used for comparison. We utilized TDA method in the EEG-based robotic rehabilitation system.
Control scheme of the EEG-based robot-aided rehabilitation training system is shown in Fig. 9. It is designed as a two-level scheme, namely the high-level and low-level. The high-level controller is implemented on a PC and the low-level controller is realized on the control board.
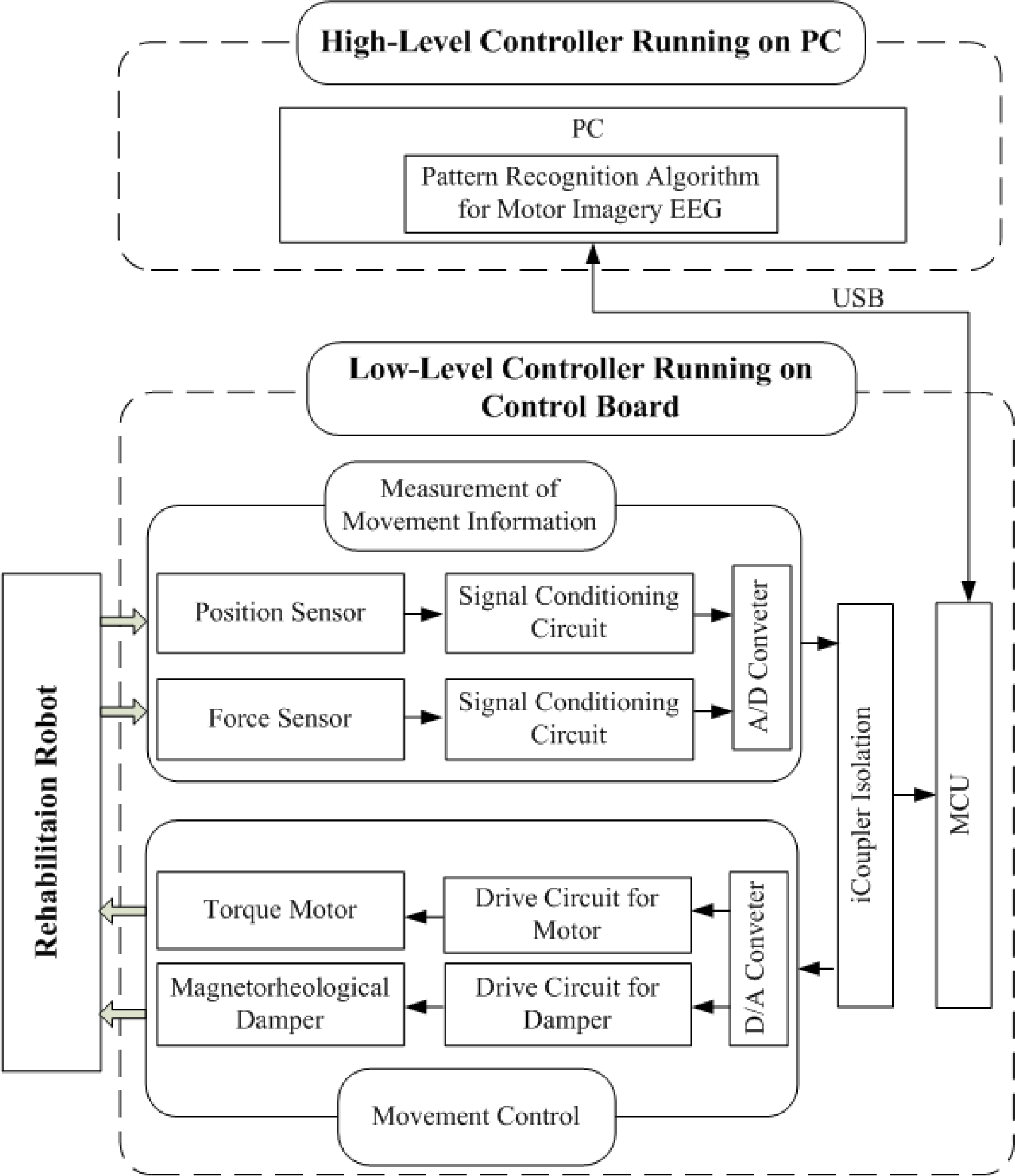
Control scheme of the EEG-based robot-aided upper-limb rehabilitation system
The high-level controller of robotic rehabilitation system is implemented under our BCI research platform and provides control board with trigger commands for performing rehabilitation exercises. The research platform which allows several BCI applications to be included into one single system is made up of three core modules: Recording module records the data of multiple experiments according to the experimental timing; Training module extracts features from training data saved by recording module and calculates the parameters of the classifier so as to be used in the testing module; Testing module records each experimental data and classify the feature vector. According to the result of the classification, PC transfers the trigger command to the low-level controller.
The lower-level controller of the EEG-based upper-limb rehabilitation system is realized on the control board and is responsible for receiving the commands from high-level controller, and controlling the rehabilitation robot arm. Control loop running on the control board monitors the motor angles and torques continuously for the purpose of providing a smooth and safe motion of the robot arm. In order to improve the stability of the control system, chips based on iCoupler technology are chosen to serve as isolators of control signals between microcontroller and analog circuit. Following the high-level command, the affected upper limb of the subject will be manipulated by the rehabilitation robot and performs various physical exercises.
The experiments were carried out with eight right-handed subjects aged between 23 and 29 (four females, four males). None of the subjects had previous experience with motor imagery. All the subjects were volunteers from Southeast University in Nanjing, China. The study had been approved by local committee.
Experimental procedures
Participants were seated upright, watching a 19’ monitor screen at a distance of lm with black background. The first 2s was quiet. At t=2s, a cross “+” was displayed for Is to indicate the beginning of the trial. Then, at t=3s, three dimensional animation of left or right upper limb movement was displayed as cue. At the same time, the subject was asked to image left or right upper limb movement in according with the cue. Finally, PC triggered the upper limb rehabilitation robot and gave the feedback of virtual upper-limb movement according to the classification result of online pattern recognition algorithm.
The experiments consisted of 10 sessions for each subject and each session was conducted on a different day. Each session was made up of 4 runs for training and 5 runs for testing. Each run consisted of 10 trials. Participants were allowed to take rest at the end of each run.
Experiment Results
Using this rehabilitation system based on motor imagery EEG, online experiments have been conducted on 8 subjects. For the left upper-limb robotic rehabilitation, if the left upper-limb movement imagination is detected correctly, the rehabilitation robot will manipulate the affected left upper-limb in a similar way as during a physical therapy exercise. If the right upper-limb movement imagination is decoded correctly, feedback of virtual right upper-limb movement is given by PC so as to reinforce the motor imagery process. Conversely, for the right upper-limb rehabilitation therapy, if the left upper-limb movement imagination is detected correctly, PC gives the feedback of virtual left upper-limb movement for the purpose of enhancing the motor imagery process. If the right upper-limb movement imagination is decoded correctly, the impaired right upper-limb will be stretched by the robot arm to perform recovery training.
As discussed in the Section 2.3.1 and Section 2.3.2, the following hybrid features were used:
Six statistical features of wavelet coefficients. Six coefficients of the AR model.
Channel C3 and C4 were used for feature extraction and only the data between t=4s and 7s was selected in order to get the segment that contained the most obvious difference between the two motor imagery tasks. Hence, six statistical features of harmonic wavelet coefficients and six AR coefficients were obtained for each channel, giving a total of 24 features for a motor imagery task during upper limb rehabilitation exercise.
Fig. 10 demonstrates the classification accuracies of the first session online experiments for eight subjects where LDA classifier was used for all runs of the session. None of the subjects had previous experience with motor imagery and they were able to reach a classification accuracy between 80.00% and 92.00% in the first session. Moreover, average error rate is as low as 13.5%

The classification accuracies obtained of the first session for the eight subjects, where LDA classifier was used for all runs of the session.
Fig. 11 illustrates the average recognition rates obtained for all subject during 10 sessions. NN classifier (offline), SVM classifier (offline) and LDA classifier (online) were applied to classify the motor imagery EEG based on the proposed features. The NN is composed of an input layer, a hidden layer and an output layer. The input layer has 24 nodes for the features, the hidden layer has 19 nodes and the output layer has 2 nodes. The training algorithm utilized is the gradient descent with momentum and adaptive learning rate backpropagation. The SVM with Gaussian kernel was used. It is observed that the performance of NN and LDA are similar, but the SVM is a little inferior. LDA gets the satisfactory results with an average error rate as low as 10.10%.
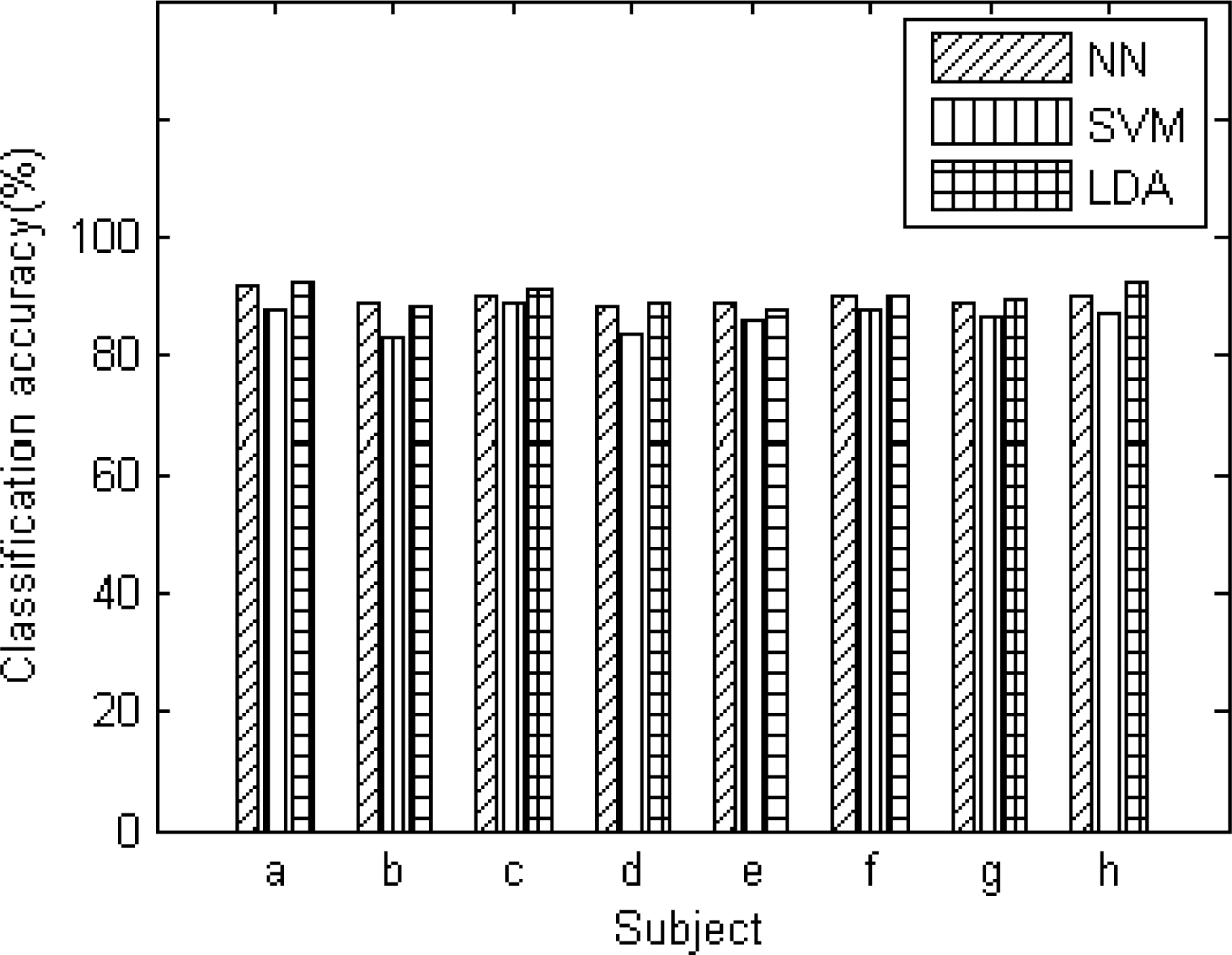
The average recognition rates of 8 subjects. Results were obtained using NN, SVM and LDA classifiers.
Fig. 12 shows the average classification accuracies of LDA among harmonic wavelet features (offline), AR features (offline), and a combination of them (online). Harmonic wavelet and AR feature extraction methods with the LDA classifier obtained the average classification accuracy of 83.30% and 81.22% respectively. So both HWT and AR model are the effective tools to extract features from motor imagery EEG. However, the recognition rate is greatly improved when using the combined feature vectors and more information of the motor imagery EEG is obtained.

Results obtained using LDA classifier. The features are calculated respectively using harmonic wavelet features, AR features and a combination of them.
Additionally, experimental results on 8 unimpaired participants with the proposed EEG-based upper limb rehabilitation system demonstrate that the following design aims have been achieved.
Mechanical design, safety consideration, controller design and drive mode of the rehabilitation can meet the requirements of rehabilitation exercises. By providing direct communication between the patient's mental process and the upper limb rehabilitation system, the patient's motor initiatives can be fully explored and the stroke patients can perform recovery training effectively. Following the trigger command of the high-level controller, the rehabilitation robot is able to manipulate the patient's affected upper limb to perform physical exercise. Moreover, the arm of the robot moves stably and smoothly and it can reduce the vibration and chattering phenomena caused by the change of the patient's physical condition. Rehabilitation robot can be adjusted to fit for patients with different height, weight and muscle tone. Physiological parameter is saved in order to better understand the process of rehabilitation therapy.
In this paper, we present a new approach to offer rehabilitation training for stroke patients. The feasibility of combing robot-assisted rehabilitation with motor imagery based BCI was investigated. We integrated the rehabilitation robot with BCI platform and the patient's EEG of upper limb movement imagination is translated into commands to trigger the rehabilitation robot to manipulate the affected upper limb in a similar way as during a physical therapy exercise.
By providing communication between the patient's mental process and the robotic system, the rehabilitation system can fully explore the patient's motor initiatives and guide the stroke patients to perform rehabilitation training effectively. The functional outcome of rehabilitation is expected to improve. Preliminary results on unimpaired participants demonstrate the feasibility of the rehabilitation system under online operation.
Based on the promising results of this pilot study clinical study is currently made on the therapy effect of our upper limb rehabilitation system for a larger group of stroke patients. Moreover, we are also looking into converting the synchronization motor imagery tasks to be asynchronous whereby the patient can perform rehabilitation training without the visual stimulus cues.
Footnotes
5.
This work was supported by the Natural Science Foundation of China (No. 61104206, No. 61075068), the National Key Technology R&D Program (No. 2008BAI50B00), the Key Project of Ministry of Education of China (No. 107053), the Key Project of Natural Science Foundation of Jiangsu Province (BK2010063), the National Science Foundation for Post-doctoral Scientists of China (No. 20100481090), and the Science Foundation for Post-doctoral Scientists of Jiangsu Province, China (No. 1002014B).