
Abstract
Background
Robotic-assisted rehabilitation technologies (RAT) are promising tools for stroke recovery, offering repetitive, task-specific, and feedback-driven training. Yet, their integration into routine clinical practice in Saudi Arabia remains limited. This study examined healthcare professionals’ awareness, perceptions, and adoption of RAT for stroke rehabilitation in Jeddah.
Methods
A cross-sectional survey was conducted among 210 healthcare professionals (neurologists, physical therapists, occupational therapists) from major hospitals in Jeddah. Data were collected using a validated questionnaire covering demographics, awareness, perceptions, adoption, and future outlook regarding RAT. Descriptive and inferential statistics were applied, with p < 0.05 indicating significance.
Results
Overall, 59.7% of participants had heard of RAT, but only 50% reported moderate understanding. Perceptions were generally positive, with 54.5% rating RAT as effective and 54% as safe. However, clinical adoption was low (30.4%), and usage was mostly rare (59.4%). Adoption was significantly associated with age, professional role, and years of experience (p < 0.05). Key barriers included high cost (32.4%), limited availability (23.8%), insufficient training (23.3%), and lack of awareness (20.5%). More than half of respondents (53%) believed RAT would play a pivotal role in future stroke rehabilitation, citing improved accessibility, cost reduction, and enhanced training as key facilitators.
Conclusion
Awareness and perceptions of RAT among healthcare professionals in Jeddah are moderate to positive, yet clinical adoption remains limited due to cost, training, and accessibility barriers. Enhancing knowledge, providing targeted training, and developing supportive policies are essential to align RAT implementation with Saudi Arabia’s Vision 2030 objectives for advanced healthcare innovation.
Introduction
Stroke is a major public health concern and a leading cause of long-term disability worldwide. Its impact on patients’ physical, psychological, and social well-being underscores the need for effective rehabilitation strategies to enhance quality of life and reduce the burden on healthcare systems. 1
Robotic-assisted rehabilitation technologies (RAT) have gained attention for their potential to improve motor recovery and independence in stroke survivors by enabling repetitive, task-specific training, providing precise feedback, and reducing the physical demands on healthcare professionals, thereby promoting neuroplasticity.2–4 In this study, RAT refers collectively to both upper-limb systems, which target arm and hand function, and lower-limb systems, commonly called robotic-assisted gait training, which focus on mobility; both share principles of high-intensity, task-specific repetition with real-time feedback. 5 RAT has shown meaningful improvements in functional outcomes for both upper- and lower-limb stroke recovery, offering intensive, task-specific, and feedback-driven training that supports neuroplasticity. Recent evidence also highlights the importance of personalized rehabilitation approaches that account for individual differences among stroke survivors, emphasizing the role of motivation, engagement, and patient-centered therapy in optimizing recovery.6–8 Technologies such as robotic systems can enhance patient involvement and provide tailored interventions, supporting healthcare professionals -particularly physiotherapists-in delivering more precise, consistent, and effective treatment aligned with each patient’s needs.
Healthcare professionals’ awareness, perceptions, and adoption of emerging rehabilitation technologies have been widely examined across diverse healthcare systems. International studies consistently show that clinicians’ acceptance of robotic and digital rehabilitation technologies is influenced by factors such as perceived effectiveness, safety, usability, cost, institutional backing, and training access.9–11 While many clinicians acknowledge the potential of robotic-assisted rehabilitation to enhance motor recovery and therapy efficiency, real-world adoption remains variable and often limited, even in well-resourced healthcare settings.12,13 These findings highlight a persistent gap between technological advancement and clinical implementation, underscoring the need to better understand contextual and professional determinants of adoption.
Most existing evidence on robotic-assisted rehabilitation originates from high-income Western countries, with limited data from Middle Eastern healthcare systems. In Saudi Arabia, where stroke prevalence is estimated at 29.8 per 100,000 individuals and rehabilitation services remain largely reliant on conventional physiotherapy, empirical research on healthcare professionals’ awareness, perceptions, and adoption of robotic-assisted rehabilitation technologies is scarce.14–16 Previous studies have identified barriers to RAT adoption, including high costs, limited availability, insufficient training, and low awareness among healthcare providers. 17 Overcoming these barriers is essential to modernize stroke rehabilitation and supports the objectives of Saudi Vision 2030, which emphasizes healthcare innovation, technological advancement, and improved patient outcomes. 18
To address these gaps, this study investigates healthcare professionals’ awareness, perceptions, and adoption of RAT for stroke rehabilitation in Jeddah, Saudi Arabia. Specifically, it assesses participants’ level of awareness, explores perceptions regarding the effectiveness, safety, and perceived cost of these technologies, and identifies barriers and facilitators that may influence their integration into clinical practice. The ultimate goal is to provide insights that can guide strategies to enhance RAT adoption and support improved rehabilitation outcomes for stroke patients.
Methods
Study design and setting
This cross-sectional study was conducted in Jeddah, Saudi Arabia, targeting major hospitals with established stroke rehabilitation programs, including Saudi German Hospital, Dr. Soliman Fakeeh Hospital, Dr. Soliman Habib Hospital, International Medical Center, and Andalusia Hospital. Data were collected at a single point in time using structured questionnaires. The study was designed and reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines for observational studies.
Participants and sampling
A total of 210 healthcare professionals participated in the study. Participants were recruited using convenience sampling from the selected hospitals, based on accessibility and involvement in stroke rehabilitation programs. Eligible participants included neurologists, physical therapists, and occupational therapists currently engaged in stroke care. Healthcare professionals not directly interacting with stroke patients were excluded.
The required sample size was determined using G*Power software (v.3.1.9.7) with a priori χ2 tests for goodness-of-fit. Input parameters included an effect size (w) of 0.3, alpha error probability of 0.05, power of 0.95, and degrees of freedom set to 5. The calculation yielded a required sample size of 220, ensuring adequate statistical power. 19 Our study included 210 respondents, slightly below the target, which may marginally affect statistical power but remains adequate for exploratory analysis.
Data collection
Data were collected using a structured questionnaire adapted from previously validated instruments.20,21 The questionnaire underwent expert review by professionals in rehabilitation technologies and stroke care to ensure content validity. Internal consistency was confirmed with a Cronbach’s alpha of 0.7.
The questionnaire comprised the following sections: Demographics (age, gender, education level, years of experience, and professional role); Awareness (2 questions assessing understanding of RAT and its applications); Perceptions (2 questions evaluating views on effectiveness and safety of RAT); Adoption (3 questions on clinical use and perceived barriers); and Future Outlook (2 questions on the anticipated role of RAT and factors encouraging its adoption).
The questionnaire was intentionally designed to be brief, particularly for the awareness and perception domains, to minimize respondent burden and maximize participation and completion rates among busy healthcare professionals. This concise structure was considered suitable for capturing overall assessments within a cross-sectional survey while maintaining acceptable internal consistency.
Ethical considerations
Ethical approval was granted by the Ethical Committee of Batterjee Medical College, Jeddah, Saudi Arabia (Reference No. RES-2025-0005). Written informed consent was collected from all participants. For online surveys, participants provided electronic consent prior to participation, and signed consent forms were collected when applicable.
Statistical analysis
Data were analyzed using IBM SPSS Statistics version 28. Descriptive statistics (frequencies, percentages, means, and standard deviations) summarized demographics and survey responses. Awareness and perception were treated as ordinal variables, while adoption was categorical. Associations with demographic variables were examined using Chi-square, Kruskal-Wallis, Mann-Whitney U, and Spearman’s rank correlation tests as appropriate.
The analysis focused on descriptive and bivariate statistical methods to explore associations between adoption of robotic-assisted therapy and selected demographic and professional characteristics. Multivariable analysis was not performed, as the study was exploratory in nature and the sample size of RAT users was relatively limited. Therefore, the findings should be interpreted as associations rather than independent predictors.
Statistical significance was set at p < 0.05.
Results
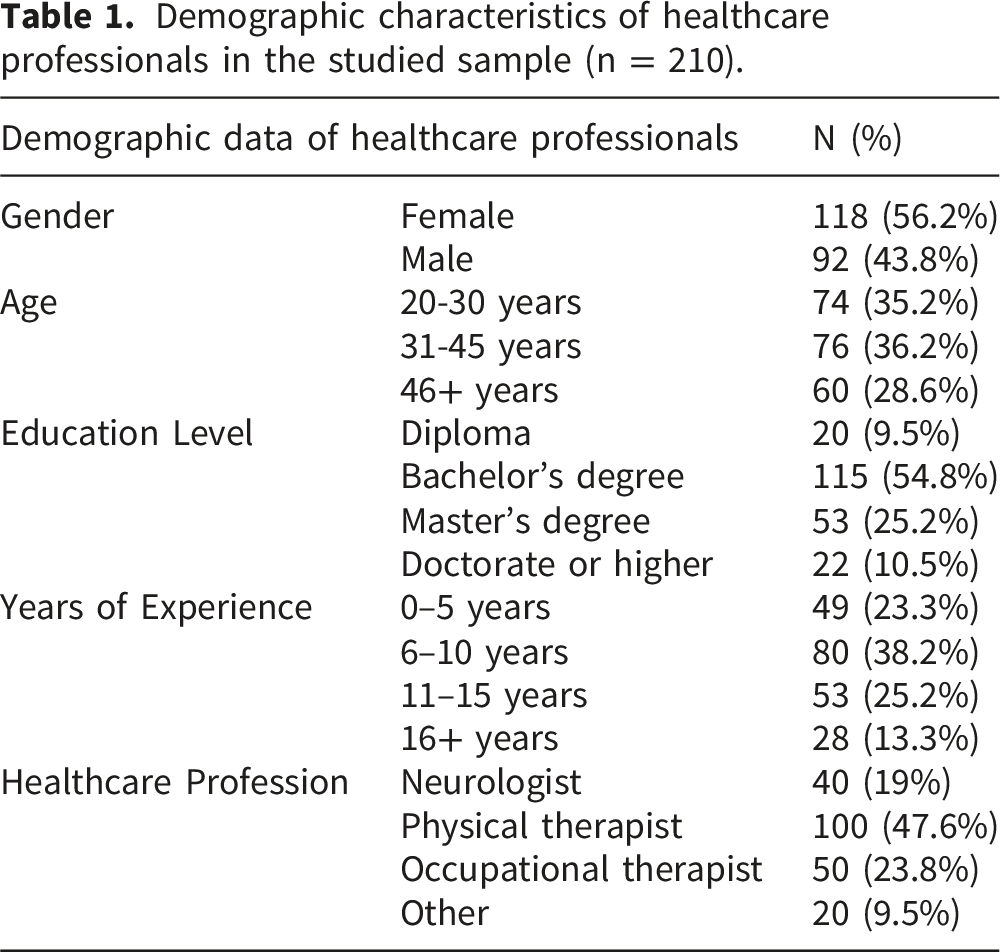
Demographic characteristics of participants
Demographic characteristics of healthcare professionals in the studied sample (n = 210).
Awareness and perceptions of robotic-assisted therapy
Awareness and perceptions of robotic-assisted technologies among healthcare professionals (n = 210).

The overall mean awareness score was 1.25 ± 0.49, indicating moderate awareness, while the mean perception score was 2.41 ± 0.57, reflecting generally positive perceptions toward RAT. Awareness scores were significantly associated with age, educational level, and years of experience (all p < 0.05). Similarly, perception scores, including views on effectiveness and safety, were significantly associated with profession, gender, and years of experience (all p < 0.05), with more experienced professionals and those in specific disciplines demonstrating higher perception scores.
Clinical adoption of robotic-assisted therapy
Clinical practice and adoption of robotic-assisted technologies among RAT users (n = 64).
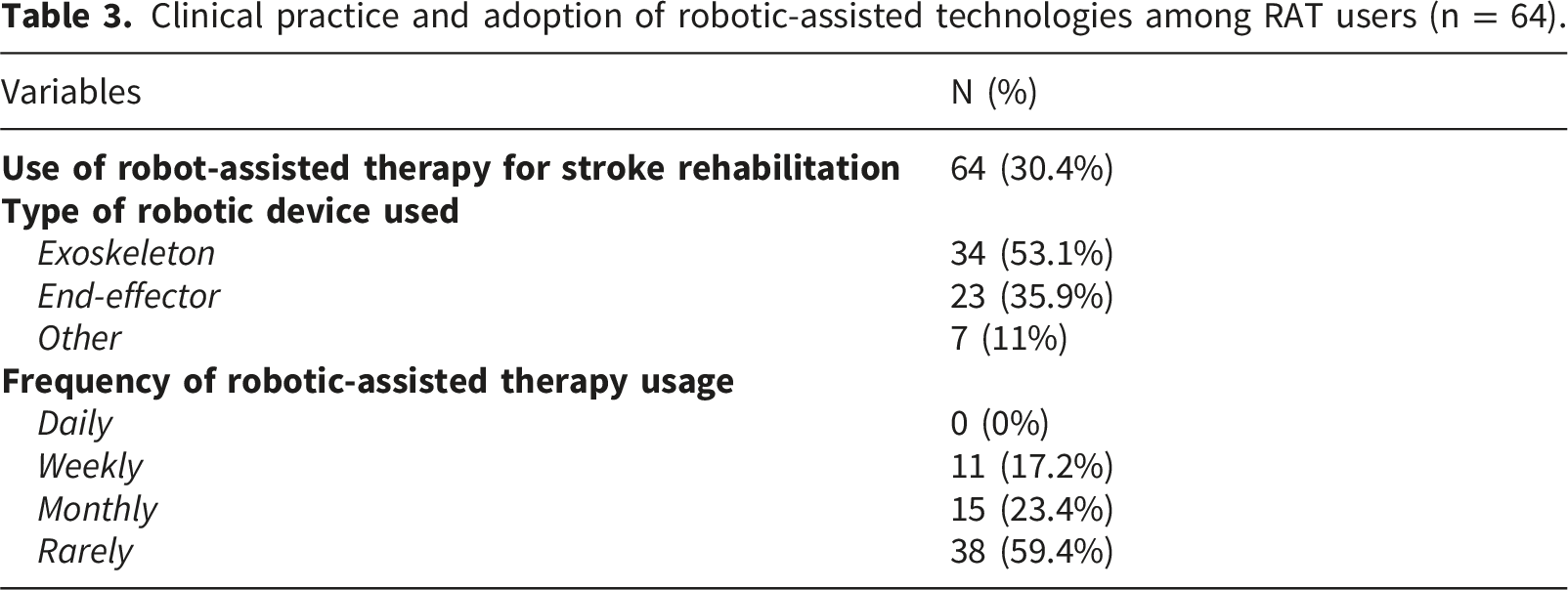
Clinical adoption (actual use of RAT) was significantly associated with age (p < 0.01), profession (p < 0.05), and years of experience (p < 0.001), with older and more experienced professionals showing greater adoption. Major barriers to adoption included high cost (32.4%), limited availability (23.8%), insufficient training (23.3%), and lack of awareness (20.5%) (Figure 1). Main barriers to the use of robotic-assisted therapy in stroke rehabilitation (n = 210).
Future outlook of robotic-assisted therapy
More than half of the respondents (53%) believed that RAT will play a pivotal role in the future of stroke rehabilitation in Saudi Arabia. Key factors perceived to encourage adoption included improved accessibility (38%), reduced cost (27.5%), enhanced training opportunities (24.2%), and increased awareness and education (10.3%) (Figure 2). Key factors facilitating adoption of robotic-assisted therapy among healthcare professionals (n = 210).
Discussion
This study offers one of the first insights into healthcare professionals’ awareness, perceptions, and clinical adoption of robotic-assisted therapy (RAT) for stroke rehabilitation in Saudi Arabia. Findings indicate moderate awareness and generally positive perceptions, but relatively low clinical adoption, highlighting barriers that limit RAT integration into routine practice.
The study showed that only a portion of participants had heard of RAT, and merely a few reported high understanding. These findings highlight a substantial knowledge gap, consistent with prior studies in low-to middle-income regions, where awareness of advanced rehabilitation technologies remains limited.14,21 Similar trends have been observed globally, with awareness levels rarely exceeding moderate levels among clinicians in comparable healthcare settings.17,22 The significant associations between awareness, age, education, and years of experience in this study align with previous evidence indicating that senior professionals and those with higher educational attainment are more likely to engage with emerging technologies.15,23,24 Targeted educational programs-integrated into continuing medical education (CME)- could enhance familiarity with RAT’s evidence base and practical applications. 25
Perceptions of RAT were generally positive, with many participants viewing it as effective and safe. This optimism mirrors findings from recent studies where healthcare workers acknowledged RAT’s potential to improve motor outcomes, reduce therapy workload, and enhance patient engagement.3,16 However, the persistence of uncertainty-nearly one-quarter rated RAT as moderately effective or moderately safe-suggests lingering concerns about cost-effectiveness, training adequacy, and safety standards. 26 These concerns may stem from limited exposure to RAT in routine practice and a lack of national guidelines supporting its implementation. Integration of evidence-based frameworks, such as the Technology Acceptance Model (TAM), has been recommended to address these perceptions, emphasizing ease of use, perceived benefit, and institutional support. 10
Despite positive perceptions, actual adoption was low, with only a portion of respondents incorporating RAT in practice-most using exoskeletons- and most reporting rare usage. This reflects a global trend where RAT remains underutilized despite promising clinical outcomes.27,28 Barriers identified, such as high cost, limited availability, insufficient training, and lack of awareness, are consistent with previous studies highlighting financial and infrastructural constraints as primary impediments in resource-limited healthcare systems.29,30 Cost concerns may be particularly relevant in Saudi Arabia, where advanced rehabilitation facilities remain concentrated in tertiary centers, limiting patient access and clinician exposure.31,32 Strategies to address these barriers include government-subsidized programs, integration of RAT modules into rehabilitation curricula, and structured hands-on workshops to enhance competence and confidence in using robotic systems. 33
Over half of the respondents believed RAT will play a pivotal role in the future of stroke rehabilitation in Saudi Arabia. This finding reflects expectations rather than confirmed implementation and should be interpreted cautiously due to the cross-sectional design and reliance on self-reported data. Although these views align with national healthcare innovation strategies, they do not necessarily indicate current readiness for widespread adoption.
This forward-looking perspective is consistent with international projections anticipating increased adoption as technologies become more accessible and cost-effective.29,34 Participants identified improved accessibility, reduced costs, enhanced training, and awareness campaigns as key facilitators, paralleling findings from recent implementation studies in which these factors significantly predicted successful integration.29,35 Notably, the emphasis on training aligns with evidence from multiple healthcare contexts demonstrating that clinician upskilling is associated with more favorable perceptions and a greater willingness to adopt new technologies.12,36
Although this study was conducted in Jeddah, Saudi Arabia, the identified barriers and facilitators to robotic-assisted rehabilitation adoption are consistent with those reported in international settings, supporting the broader relevance of the findings.
This study has several
Conclusion
Awareness of robotic-assisted therapy among healthcare professionals in Jeddah is moderate, and perceptions are generally positive; however, clinical adoption remains constrained by high costs, limited availability, insufficient training, and lack of awareness. Adoption also varies with age, experience, and professional background. These findings underscore the need for targeted policy interventions, including investment in training programs, increased accessibility of RAT, and strategies to raise awareness, to support the integration of robotic-assisted therapy into routine stroke rehabilitation in Saudi Arabia.
Future directions
Future research should employ longitudinal designs to monitor changes in awareness, perceptions, and adoption following educational or infrastructural interventions. Comparative studies across regions in Saudi Arabia and the Gulf could elucidate geographical and institutional disparities. Incorporating mixed-method approaches, including qualitative interviews, can provide nuanced insights into clinician attitudes and contextual barriers. Cost-effectiveness analyses are needed to guide policy and encourage investment in RAT technologies.
Footnotes
Ethical considerations
Ethical approval was granted by the Ethical Committee of Batterjee Medical College, Jeddah, Saudi Arabia (Reference No. RES-2025-0005). Participants provided informed consent prior to beginning the online survey, in accordance with ethical guidelines. Artificial intelligence (AI) tool, Quillbot, was employed exclusively to enhance language clarity and style. It was not involved in the creation of content, data analysis, interpretation of results, or development of research ideas.
Author contributions
Ahmed E. Altyar supervised the research, provided continuous guidance throughout the study, and reviewed the final manuscript. Iffat Fatima Abdullateef conceived the research idea, carried out the practical component of the study, and contributed to drafting sections of the manuscript. Mai Albaik, as the main supervisor, oversaw the student’s work, obtained ethical approval, performed data analysis, and contributed to writing and critically revising the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Guarantor
Dr. Mai Albaik is the guarantor of this work and takes full responsibility for the integrity of the study and the accuracy of the data analysis and reporting.