
Abstract
Keywords
Introduction
Background
Worldwide, 12,2 million people suffer stroke annually, and of these 5 million are in great need of rehabilitation. 1 These numbers are expected to increase over the next century, due to a growing ageing population. 2 Stroke is a neurological disorder characterized by blockage or leakage of blood vessels in the brain, causing insufficient blood flow and neuronal dysfunction. 3 Most stroke patients survive the initial injury, however long-term disabilities affecting activities of daily living and participation are common. 4 Along with lesion location and lesion size, the effect of rehabilitation activities can affect degree of recovery. 4 Rehabilitation after stroke is therefore of outmost importance to potentially alleviate and regain the functions lost. Importantly, upper limb paresis has been reported to appear in around 70% of stroke survivors 5 and regaining this function is essential in stroke rehabilitation to gain independence in activities of daily living (ADL).
Interventions for motor recovery appear at different levels of the International Classification of Function and disability (ICF) categories such as body functions and structures, activities and participation. Motor learning principles such as task- and context-specific training related to patient goals are widely accepted. Indeed, rehabilitation aiming at repetitive utilization of motor function mimicking specific tasks in the patients’ environment have been shown to be beneficial. Intensive, high-repetitive task-specific training is therefore recommended and regarded best practice in motor rehabilitation.6,7,8
Advances in non-invasive robotic assisted rehabilitation have given promise to augment and facilitate these mechanisms during recovery after stroke. Several studies have shown that robot-assisted exercise can ensure a higher number of repetitions within a therapy session, compared to conventional therapy, suggesting superior effectiveness. 9 However, discrepancy in how these protocols are applied and reported makes interpretation and generalization regarding results difficult.
Robot-assisted exercise
The use of robotics in rehabilitation of motor functions has increased exponentially in the last decades. 10 Many of the newly developed robotic systems have a virtual reality-aspect simulating real-life ADL and providing encouraging feedback, which may motivate patients to endure more repetitions. 11 Another positive aspect of this novel approach is the fact that a single therapist can assist several patients in their robotic training, simultaneously. This potentially increases the amount of therapy that stroke survivors are offered in a rehabilitation setting. 12
Numerous studies have investigated the effectiveness of robot-assisted hand and arm training, compared with conventional therapy.12,13 Results indicate beneficial effects on upper limb recovery, strength, motor control as well as ADL when rehabilitation is robot-assisted.6,14,15,16 These studies have evaluated the effectiveness of a wide range of robotic systems, which differ in the number of joints/directions used (degrees of freedom), type of visual feedback and type of device (end-effector/exoskeleton). Some of these systems are still under development while others are fully commercialized. Previously published systematic reviews and meta-analysis have not differentiated between commercially available and none-commercially available assistive robotic devices, used in stroke rehabilitation.16,17,18
Besides the differences in technical specifications of the robotic systems used, the intervention protocols (dosage) used, differ widely. The duration of a single session (number of minutes), the duration of the intervention period (number of weeks), the frequency (times a week) and intensity (energy expenditure) vary considerably in studies evaluating the effects of robot-assisted arm training. 6 Robotic arm training represents a promising and novel rehabilitation trajectory, thus more knowledge is needed regarding dose–response relationship before developing evidence-based guidelines.
Rationale for this systematic review
Several systematic reviews suggest positive effects of robot-assisted arm training on the arm and hand function in stroke survivors compared to conventional treatment.7,18,19 However, literature is lacking regarding effectiveness of different types of commercially available robotic devices, as well as impact of duration, frequency and intensity in performing such training. The objective of the present study was to evaluate the effectiveness of arm exercise performed with commercially available robotic devices on arm and hand function in stroke survivors.
Methods
The Cochrane collaboration’s method guidelines for systematic reviews were followed, 20 and to ensure transparent and complete reporting of the review, the PRISMA guidelines were used to guide the process. 21 The protocol for this review can be accessed via the Current Research System In Norway (CRISTIN: www.cristin.no; project-ID number 2,545,837).
Eligibility criteria
Eligibility was phrased using the PICOS approach
20
:
For inclusion in this study, the full-text articles had to be in a Scandinavian language or in English. We excluded literature reviews and systematic reviews, studies with less than five included subjects, as well as studies performed before 2005.
Systematic search of literature
Literature was systematically searched in the electronic databases Medline, Embase, CINAHL, AMED and the Cochrane Central Register of Controlled Trials (Cochrane Library), conducted by a research librarian. The different databases were searched for eligible studies from 2005 until January 2022. The specific search strategies were created in collaboration with a research librarian with expertise in systematic review searching and were independently peer reviewed by another librarian according to the 2015 PRESS guideline statement 22 (Appendix 2.). Primary search terms that were used to define stroke were Stroke*, Stroke rehabilitation, Subacute stroke, Cerebrovascular Accident, Cerebrovascular Accidents, CVA* (Cerebrovascular Accident), Cerebrovascular Apoplexy, Apoplexy, Cerebrovascular, Vascular Accident, Brain, Brain Vascular Accident, Brain Vascular Accidents, Vascular Accidents, Brain Cerebrovascular Stroke, Cerebrovascular Strokes, Apoplexy, Cerebral Stroke*, Acute Stroke. Each of the primary terms was paired with secondary terms defining the intervention: Robotics, Robots, Robotic arm rehabilitation, Robotic rehabilitation, Robot-assisted therapy, Robot-aided system, End-effector, Upper limb rehabilitation robot, Arm exoskeleton, Upper limb exoskeleton, Exoskeleton device, Armeo spring, Diego, Armeo Power, Amadeo, ARMin, InMotion, MIT-manus, Barrett UE Robotic Trainer. These terms were paired with a third set of terms related to measure outcome: upper extremity, upper limb, muscle strength, mobility, range of motion, recovery of function, activities of daily living, ADL, arm, hand, finger, wrist, forearm, shoulder or elbow. The search strategy was adapted to the syntax and subject headings of the different databases. Embase classic search strategy is included in Appendix 1.
Study selection
After removal of duplicates, titles and abstracts were screened according to the eligibility criteria by two of the reviewers (TJ and LS), independently. Each robotic device was considered to be commercially available if it was possible to obtain the robot through sales representatives or find price information from websites. The included references were retrieved in full-text and again reviewed by the same authors, that is, reviewed by one author (TJ) and double-checked by the second author (LS). Any disagreements between the two reviewers were resolved by consensus or in consultation with a third reviewer (MFW), if needed.
Data extraction and management
The extracted data was transferred to predefined summary tables by one of the authors (TJ) and verified by one of the others (MFW or LS). Extracted data included type of stroke; robotic device; age, sex, number of participants; duration of intervention; duration of intervention period; outcome measures; title, main author, publication year, journal name, country of origin, publication language; and setting.
Risk of bias assessment
The risk of bias in the individual studies were assessed by using the Cochrane Collaborations Risk of Bias Tool. 20 To ascertain the validity of the included studies, two reviewers (TJ and LS) independently assessed the risk of bias, including judging the adequacy of randomization and allocation concealment, the blinding of assessors and whether incomplete outcome data or selective reporting seemed likely. Any disagreement was solved by a third author’s (MFW) view of the assessment. The assessment was performed using the Review Manager Software version 5. Risk of bias across studies were assessed using GRADEpro Guideline Development Tool. 23
Summary measures and synthesis of results
We conducted four separate random effects meta-analysis to synthesize the results. One for the primary outcome (hand and arm function) and one for each of the secondary outcomes (strength, ADL, spasticity). The choice of a random effects model was based on the heterogeneity of effect in our set of studies, the difference in the sample population considering that we had a range of participants from sub-acute to chronic stroke and the use of multiple different outcome measures used in the studies included.
In cases where the same outcome was measured using different, but comparable tools on a continuous scale, the outcome measures were converted to a standard format by calculating the standardized mean difference (SMD; Cohen’s d), that is, the effect size. 20 When reporting the results, we used the rule of thumb described by Cohen, suggesting that a SMD of 0.2 represents a small effect, a SMD of 0.5 represents a medium effect and a SMD of 0.8 represents a large effect. 24 Three of the analyses were performed with SMD because the included studies utilized different outcome measures, while one analysis (spasticity) used mean difference (MD) since all included studies used the same outcome measure.12,25,26,27,28,29,30
In studies where multiple outcome measures for hand and arm function were included, we established a hierarchy system for the different outcome measures and added data from the outcome measure highest on the hierarchy system. Two clinicians that were not involved in the study made the system, both having expertise in outcome measures regarding hand and arm function for stroke survivors. This system was established to avoid risk of bias when pooling results of two or multiple outcomes from one study.31,32
In studies with missing data, we contacted the corresponding authors to request the desired information (n = 12),12,13,26–30,33–38 for example, standard deviation (SD) for the difference in means. In cases where it was not possible to obtain this data, we calculated SD from p-values, a method recommended in the Cochrane Handbook for Systematic Reviews of Interventions. 20
In studies where p-values were not reported, we calculated correlation coefficients from other studies included in this review that utilized the same outcome measure and used this to calculate SD from the difference in means that was reported, as recommended in the Cochrane Handbook. 20
Additional analyses
To assess associations between treatment effects and duration of intervention, as well as intensity and frequency of treatment, separate linear models was estimated for individual dosage, length of intervention period and treatment frequency during intervention. Data was analyzed using the metareg-package in the R-framework. 39 The meta-regression was performed on the primary outcome only. Due to high degree of correlation between the different independent variables, one model was estimated for each variable separately. To correct for multiple comparisons, we utilized false discovery rate, as implemented in the stats package in R. 40
The subgroup analysis of the phases of stroke formed three groups: studies investigating subacute stroke, studies with chronic participants and a group of mixed population. To examine if the robotic type affects the results of the trials, a subgroup analysis was performed with two groups: studies utilizing robots with 1–2 degrees of freedom (DoF) and with 3 DoF and upwards, respectively.
Results
Study selection
The primary search identified 5276 references and after removing duplicates, 2738 references were screened. The search was updated in February 2022, and an additional 257 records were identified. Sixty-eight full text publications were reviewed. Finally, 41 studies were included (Figure 1). Flowchart of study inclusion.
The studies were further categorized into either studies that investigated the effect of robot-assisted exercise only (n = 18), studies comparing two robotic interventions (n = 5),41–45 combination of interventions (i.e., botulinum toxin A plus robot-assisted exercise) (n = 13)46–58 or non-comparable control interventions (n = 4).59–62 One study was excluded due to lack of reporting of results. 63 Eighteen studies were included in the analysis of the primary outcome of hand and arm function. Of these 18, 10 were included in the analysis of strength, nine were included in the analysis of ADL and seven were included in the analysis of spasticity.
Study characteristics
Summary of included studies.

Abbreviations: AMAT = Arm Motor Ability Test, ARAT = Action Research Arm Test, BBT = Box and Blocks Test, BDS = Beck Depression Scale, BI = Barthel Index, CRI = Cognitve Reserve Index, d = Day, DN40 = Neuropathic pain diagnostic questionnaire, FMA = Fugl-Meyer Assessment, FIM = Functional Independence Measure, m = Months, MAL = Motor Activity Log, MAS = Modified Ashworth Scale, MBI = modified Barthel Index, MI = Motricity Index, MRC = Medical Research Council for Muscle strength, NS = Not Stated, PROM = Passive Range Of Motion, RT = Robotic Therapy, SF-36 = SF-36, SIS = Stroke Impact Scale, TAU = Treatment as Usual, UE = Upper Extremity, UK = United Kingdom, w = Weeks, WMFT = Wolf Motor Function Test.
Participants
The total number of participants in the included trials were 1295 with an age ranging from 20 to 95 years of age. All studies included both male and female. Four of the studies investigated chronic stroke patients,25,30,37,38 11 studies subacute stroke patients12,26–28,33–36,64–66 and three studies investigated a combination of the two.13,29,67
Intervention
In all included trials, commercialized robots were used for the experimental interventions. InMotion2® was used in seven trials,13,25–30,38 Amadeo® was used in four trials,12,28,34,64 ReoGo® in three,35,37,65 while ArmAssist®, 66 Fourier®,36 H-Man®67 and Armeo Spring®33 was used in one trial each. 10 of the trials utilized a robot with 2 degrees of freedom,13,25–27,29,30,36,38,66,67 six used a robotic device with five degrees of freedom,28,34,35,37,64,65 while two studies investigated a robot with seven degrees of freedom.12,33
The intervention dosage (duration x frequency) used in the trials varied considerably. The total dosage provided in the studies ranged from 450 min to 2400 min in total, with a mean of 1375.33 min. Weekly dosage ranged from 135 min to 600 min per week, with a mean of 247.48 min. While daily dosage ranged from 30 min to 120 min a day, with a mean of 57.2 min. Thirteen trials had matched dosage,12,13,25,26,28,29,30,34,36,64–67 two did not,33,38 while three did not specify if the dosage was matched or not.27,35,37
Comparison
Fourteen of the included trials had specified what the control intervention contained,12,25,26,27,29,30,33,34–36,64–66 including task-oriented exercises, functional reaching tasks, neurodevelopmental training, assisted stretching, spasticity inhibition, constrained induced movement training, fine motor training, pinching and grabbing exercises, item transferring tasks and ADL training. Four studies stated that the control group received traditional occupational- or physiotherapy, or treatment as usual without specifying the content of the therapy.13,28,37,67
Outcome
For the primary outcome, hand and arm function, four different outcome measures were used in the primary studies;
All the included studies that investigated spasticity used the same outcome measure (Modified Ashworth Scale (MAS)). The included studies for strength12,25,27,28,30,33,34,37,64,67 used three different outcome measures, grip strength measured with Jamar, Medical Research Council for Muscle strength and Motrocity index. While studies investigating ADL12,13,29,33,34,36,37,65,66 used two different outcome measures, Functional independence measure and Barthel index.
Risk of bias in individual studies
The assessments of risk of bias for the individual studies are shown in Figure 2 and summarized in Figure 3. The assessments were not blinded to the reviewers. Overall, there were many unclear and high risk of bias factors due to lack of reporting. Cochrane collaboration risk of bias assessment tool. Cochrane collaboration risk of bias assessment tool.
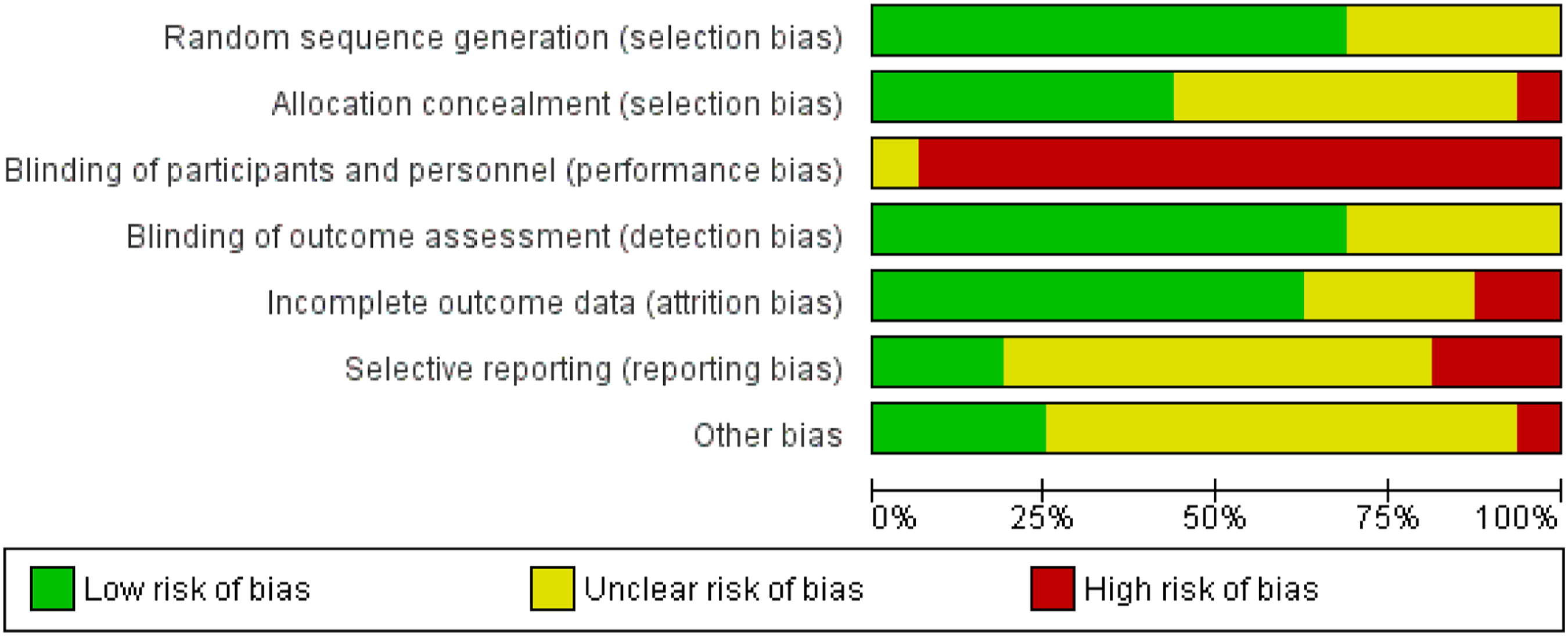
Allocation
We judged the method of random sequence generation to have a low risk of bias in thirteen trials,12,13,25,26–29,33,35,64–67 and to be unclear or not reported in five.30,34,36–38. Eight studies were judged to have adequate concealment of the allocation sequence,12,13,26,27,29,33,35,65 while nine of the trials lacked information and was judged to have unclear risk of bias.25,28,30,34,36–38,66,67 One of the studies were judged to high risk of bias due to explicitly stating that no allocation concealment mechanism was implemented. 64
Blinding
Twelve of the studies had blinded outcome assessors,13,25–28,30,35–37,65–67 and six did not specify if the outcome assessors where blinded or not and was judged to have unclear risk of bias.12,29,33,34,38,64 Blinding of participants and personnel was deemed impossible because of the nature of the intervention, and all studies, but one 34 was therefore judged to have an outcome that was likely to be influenced by lack of blinding.
Incomplete outcome data
Eleven studies had little to no attrition.13,25,27,28,30,33,36,37,64,66,67 Five studies were judged to have unclear risk of bias because of moderate dropout rate,26,29,35,38,65 while two was judged to have high risk due to high attrition rate,12,34 that could affect the outcome and reasons for dropping out was related to the intervention.
Selective reporting
Five studies did not show any risk of selective reporting,12,13,29,64,67 10 was judged to have unclear risk of bias due to not having provided any protocol information.25–28,30,33,36–38,66 Three was judged to have high risk of bias because the primary outcome of the trial was either changed or not pre-specified.34,35,65
Results of individual studies
The overall and individual effects sizes for hand and arm function, muscle strength, spasticity and ADL-activities of the included studies are shown in forest plots (see Figures 4, and 7–9, respectively). Forest plot of the effect of RT versus traditional therapy on primary outcome hand and arm function. CI = Confidence interval, df = degrees of freedom, I2 = measure of heterogeneity, Tau2 = measure of variance, RT = robotic training, SD = Standard deviation.
Synthesis of results
Hand and arm function
Figure 4 shows the results from the random effects meta-analysis comparing robot-assisted exercise (RT) with traditional therapy including 18 studies with a total of 1295 participants. A statistically significant overall effect was found in favor of the RT group, with a SMD of 0.44 (CI = 0.26–0.73, p < 0.0001), indicating a moderate effect size.
There was however a significant heterogeneity among the studies, with an I2 of 65% (p < 0.0001), indicating that the studies do not share a common effect. Since heterogeneity was high, some studies were removed to investigate sensitivity. When removing the four studies with the largest effect size25,26,65,66 from the analysis, the heterogeneity decreased and became non-significant (I2 = 17%, p = 0.27). The effect size remained significant, with a SMD of 0.21 (CI = 0.07–0.34, p = 0.004), indicating a small effect size.
Subgroup analyses of hand and arm function
Phase of stroke
Figure 5 shows the subgroup analysis on type of stroke (subacute, chronic and mixed population) on the effectiveness of robot-assisted exercise versus traditional therapy on hand and arm function. The subgroup analysis revealed a statistically significant effect in favor of RT both for the sub-acute (SMD = 0.50, CI = 0.20–0.80, p = 0.001, I2 = 67%) and chronic phase (SMD = 0.76, CI = 0.13–1.39, p = 0.02, I2 = 59%), but not for the mixed population (SMD = 0.07, CI = −0.26-0.41, p = 0.66, I2 = 47%). There were however no statistically significant differences between the groups (Chi2 = 5.16, p = 0.08), with a higher overall effect size for those in the chronic phase after stroke compared to those in the other groups. The heterogeneity between the groups were however high (I2 = 61.2%). Forest plot of type of stroke for primary outcome hand and arm function. CI = Confidence interval, df = degrees of freedom, I2 = measure of heterogeneity, Tau2 = measure of variance, RT = robotic training, SD = Standard deviation.
Type of robotic device
The subgroup analysis for the type of robotic device, i.e., the number of degrees of freedom, was performed with two groups: studies utilizing robotic devices with 1–2 DoF versus those using robotic devices with 3–7 DoF. There was however no statistically significant difference in arm and hand function between these subgroups (Chi2 = 0.99, p = 0.32). Both groups had significant effect sizes in favor of the robotic group, with the group utilizing robotic devices with 1–2 DoF having the largest SMD of 0.54 (CI = 0.20–0.88, p = 0.002), indicating a moderate effect. Both groups had high heterogeneity, with an I2 of 73% and 51% respectively. (Figure 6). Forest plot of DoF on primary outcome hand and arm function. CI = Confidence interval, df = degrees of freedom, I2 = measure of heterogeneity, Tau2 = measure of variance, RT = robotic training, SD = Standard deviation.
Meta-regression of dose/response
Associations between treatment-effects, and dosage, intensity of treatment, and length of intervention.

Statistics associated with dose/response depending on treatment effect. Nominal significant associations are highlighted, only raw p-values are displayed
Analysis of the secondary outcomes
Muscle strength
A random effects meta-analysis of the studies including strength as an outcome was performed, including 10 studies with 307 participants. The analysis showed a statistically significant difference between the groups in favor of RT, with a SMD of 0.43 (CI = 0.16–0.71, p = 0.002), indicating a moderate effect size (Figure 7) Forest plot of muscle strength. CI = Confidence interval, df = degrees of freedom, I2 = measure of heterogeneity, Tau2 = measure of variance, RT = robotic training, SD = Standard deviation.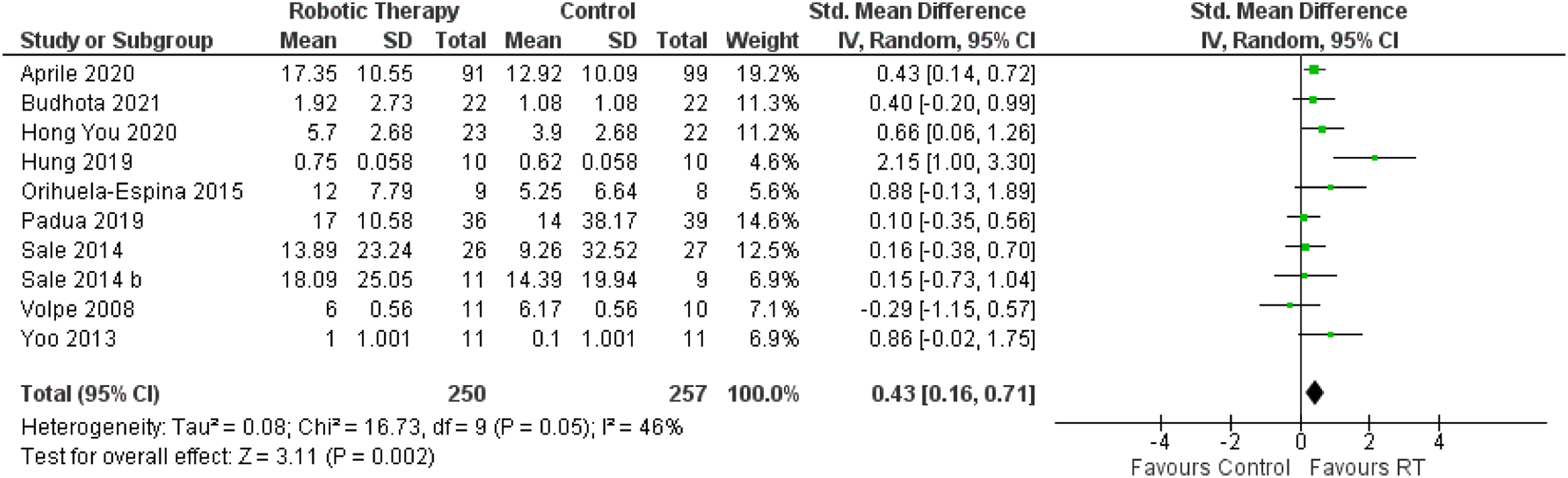
There was substantial heterogeneity among the studies, with an I2 of 46%. The variance indicates that the true effect of the intervention may lay outside of the result of the analysis. One study in the analysis showed that the control group had a greater effect on strength than RT.
Spasticity
The analysis of spasticity was performed using fixed effects meta-analysis of six studies. A fixed effects model was chosen due to all the included studies using the same outcome measure and having similar intervention periods. The analysis showed a statistically significant effect size with a MD of −0.24 (CI = −1.33-0.22, p < 0.00,001) decrease in spasticity in favor of the robotic therapy group. The heterogeneity was considerable, with an I2 of 96%, and variance was significant (Q = 167.18, p=<0.00,001). Forest plot of spasticity. CI = Confidence interval, df = degrees of freedom, I2 = measure of heterogeneity, Tau2 = measure of variance, RT = robotic training, SD = Standard deviation.
Activities of daily living
A random effects meta-analysis to investigate the effect of RT on ADL functioning was conducted of nine studies, with a total of 949 participants. The analysis showed a non-significant effect size, with a SMD of 0.11 (CI = −0.04-0.25, p = 0.17). The included studies had low heterogeneity, and the variance was non-significant (Q = 9.08, p = 0.34). Forest plot of activities of daily living. CI = Confidence interval, df = degrees of freedom, I2 = measure of heterogeneity, Tau2 = measure of variance, RT = robotic training, SD = Standard deviation.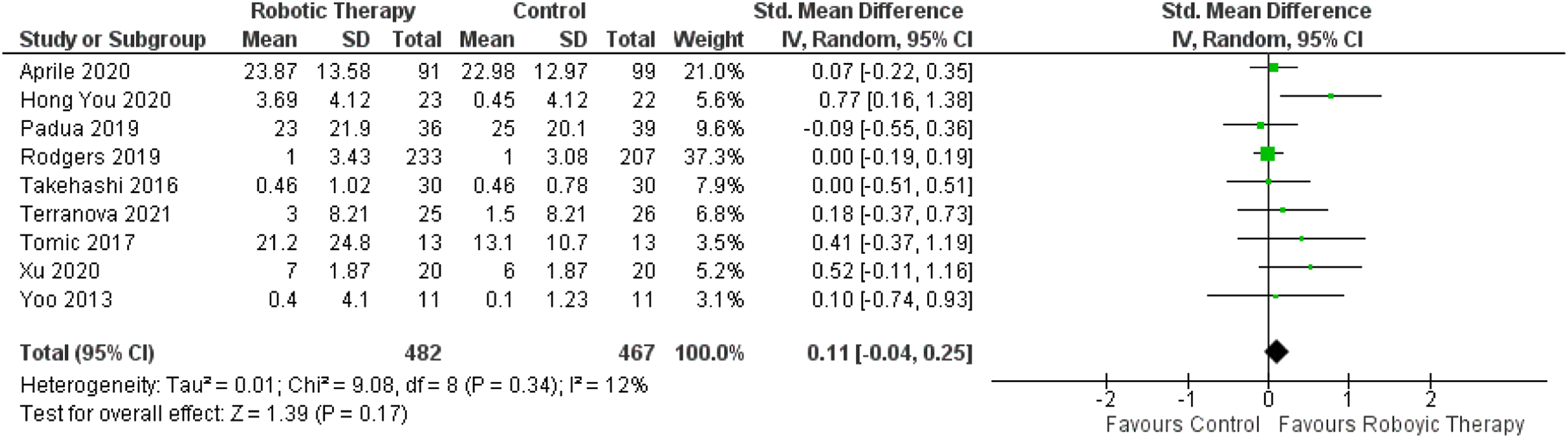
Risk of bias across studies
Assessment of risk of bias across studies, GRADE.

Explanations
Discussion
The aim for the current study has been to evaluate current evidence regarding robot assisted-motor rehabilitation. With the goal of providing ample evidence-based recommendations regarding what phase of stroke would have the most effect of robot-assisted exercise, what kind of robotic devices would give the largest effect and of what dosage would be optimal for the stroke population. Our results, based on 18 separate studies and 1295 participants, showed that RT improved hand and arm function more than traditional therapy, with a similar overall effect size for acute as well as chronic stage. Secondary analyses indicated small but significant positive effects of RT on muscle strength and spasticity in arm/hand, but not on activities of daily living. Our study did not find any significant effects of type of robotic device, nor treatment frequency or duration.
The improved hand and arm function in favor of RT found in our study supports the results of Merholz et al. (2019), 16 who concluded that people who receive electromechanical and robot-assisted arm training after stroke might improve their arm function, and arm muscle strength. This is in line with the assumption that repeated and increased exposure to activity results in increased effect of exercise.
However, and of relevance for rehabilitation value, our study did not find a significant effect on activities of daily living, suggesting that patients are not likely to transfer beneficial training effects to daily life skills. Unlike our study, Merholz et al. included studies on robotic devices being under development, in addition to commercial robotic devices. Studies conducted on developmental projects are performed by the developmental team surrounding the specific robotic device, potentially skewing results. Therefore, they included more studies and their analysis has a larger effect size across outcomes compared to our review. However, we rationalized that summarizing treatment effects for solely commercialized robotic devices leads to less possible publication bias. This because many of the studies on robotics in development Merholz et al., also conclude that future studies should consider and report key patient characteristics, such as stroke severity and level of upper limb impairment, and important parameters in hand/arm rehabilitation interventions, such as repetitions, therapy intensity, frequency and increments. 18
Our study revealed similar treatment effects for acute and chronic stroke patients. Furthermore, we did not a find any significant correlation between the exercise frequency and duration (dose) and treatment effect (response) in none of these groups. This might be due to large variations in the exercise frequencies (3–7 days/week) and durations (30–120 min per session) and total exercise duration, being used in the studies included in this review. Several studies included in our meta-analysis did not match the treatment and control group for exercise.27,33,38 In addition, the fact that exercise intensity being an important factor in dose-response relations, has not been measured in these studies, could explain why no significant correlations were found.
Regarding the phase of stroke that can expect the most effect of the intervention there was a significant difference between the groups, and the chronic group had the largest effect size. However, there was large heterogeneity in both groups and large variance in the results. This makes it impossible to make recommendations based on our analyses. Possible reasons for the large heterogeneity in the analysis is that there is a wide range in both time since stroke onset, degree of impairment, and age in the data included in the current study.
Our analysis of what type of robotic device should be utilized in the stroke population was also inconclusive. There was no significant difference between the two groups and large heterogeneity in the two groups. The included studies utilized many different types of robotic devices, with different number of DoF that could be a factor contributing to the large heterogeneity.
Our results indicated no significant correlations between dose and response. Of note, there are different factors that may affect these results making interpretation difficult. The included studies had a wide variation in dose of the intervention, both in minutes per day, weekly dosage and total duration of intervention. There was a wide range in intervention period duration. These factors can lead to heterogeneity in the analysis, causing lower certainty of the results of the analysis. Robot-assisted arm training could however increase the intensity of arm therapy in stroke rehabilitation. More repetitions during the same therapy time could be achieved with the robot-assisted therapy and thereby be a useful adjunct to conventional therapies. Furthermore, we have not investigated how training intensity affects the results of robot-assisted exercise. This was due to lack of measures regarding either metabolic equivalent of task or heart rate during training in the included studies, which is essential to interpret how intensity potentially affects the intervention.
Even though the analysis showed a significant effect in favor of RT training for hand and arm function, the overall results need to be interpreted with caution. The strength of evidence is low, and one cannot rule out the possibility of publication bias in the studies included. Trials in a relatively new research field are more likely to be published when showing significant findings. To get a truer estimate of the effect of robotic rehabilitation, the studies that does not find any significant differences between two groups needs to be published more often. Half of the studies were relatively small, with under 50 participants. Overestimation of results are more likely in small trials. 68
The analysis reviled high heterogeneity in the included studies, and sensitivity investigations was performed as described in The Cochrane Handbook for Systematic Reviews of Interventions. 20 The four studies with the largest effect size were removed from the analysis, leading to a non-significant low level of heterogeneity. There were some similarities of these studies, such as low number of participants, wide range of age, using the same outcome measure and comparing RT to conventional therapy. However, these similarities could be found in studies that did not affect the heterogeneity of the analysis when removed. Our assumption is therefore that heterogeneity may be a result of statistically underpowered studies, which is likely to be the case in many of the included trials in this study. In addition, according to The Cochrane Handbook for Systematic Reviews of Interventions, 20 the effect of some characteristics of studies may not always be identified using sub-group analyses, since some participant characteristics may vary greatly both within and across trials.
Given the large variance and heterogeneity of the included trials, we have questioned if the results of the studies were comparable enough to pool. There were differences in both the length of intervention periods, in the population investigated and in what kind of robotic device was used. As we chose to pool the results, the reader should be aware of the implications of the high risk of bias and low quality of evidence in the included studies, as these factors may affect the overall interpretation and generalizability of the results. Furthermore, to mitigate large heterogeneity and variance when summarizing study results in a meta-analysis, future studies should thoroughly specify, the participants’ injury-related characteristics, the type of robot being used and the training dose, including exercise intensity. As the review was part of a rehabilitation development project, the protocol was initially not published in Prospero as suggested in PRISMA guidelines. 21 It was however registered in Current research information system in Norway – (CRISTIN: www.cristin.no; project-ID number 2,545,837).
Limitations
This study had some limitations. Firstly, we only included commercial robotic devices. There is no specific definition of what a commercially available robotic device is, but the three authors assessed all robotic devices used in the eligible studies and judged if they were able to be purchased. This process may have led to excluding some studies that should have been included. Secondly, we have divided the different robotic devices into two subgroups of 1–2 DoF and 3-7 DoF. There are other possible ways of dividing the robotic devices, which could have affected the results of the subgroup analysis of type of robot. The stratification is based on the authors’ clinical experience but could be a limitation that should be taken into account when interpreting the results. Thirdly, there was many missing SD of the differences in means, and since we were not able to establish contact with the authors of the original studies, we imputed many missing values. The method used followed the recommendations of Cochrane’s handbook of systematic reviews, 20 but it is also stated here that if many values are missing, the authors should be careful with imputing too many variables because they would be estimates and not actual SD’s. Furthermore, some of the studies only reported on subtests of outcomes, and even though the reporting of only subtests were pre-specified, it can be a factor that affects the outcome of our analysis.
Conclusion
The results of this systematic review and meta-analysis have confirmed the effectiveness of RT over traditional therapy and indicates that the use of robotic devices in the rehabilitation of stroke patients has an (overall) moderate effect on their hand and arm function. However, the results must be interpreted with caution due to high heterogeneity among the studies included and the presence of possible publication bias. As we are now passed the robotic arm rehabilitation as a novel method, it is time for larger, methodologically more robust randomized controlled trials performed on populations that are more homogenic and sufficiently powered. More research is needed on the intensity and dose of the robot-assisted exercise that should be offered and to which stroke subpopulations. Robot-assisted exercise has the potential for being a supplementary method of rehabilitation of hand and arm function for the stroke population, especially as a method to increase the total dosage of rehabilitation.
Supplemental Material
Supplemental Material - Effectiveness of robot-assisted arm exercise on arm and hand function in stroke survivors - A systematic review and meta-analysis
Supplemental Material for Effectiveness of robot-assisted arm exercise on arm and hand function in stroke survivors - A systematic review and meta-analysis by Truls Johansen, Linda Sørensen, Knut K. Kolskår, Vegard Strøm and Matthijs Ferdinand Wouda in Journal of Rehabilitation and Assistive Technologies Engineering
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was partly financed by the DAM foundation (2021/HE1-352596). The DAM foundation has no affiliations connected to any of the companies producing the robotic devices, nor did they have any implication regarding the production of this article.
Guarantor
Matthijs Ferdinand Wouda.
Contributorship
TJ researched the literature, developed the protocol, performed selection of references, assessed bias in the included studies and performed the analyses. In addition, TJ wrote the manuscript. MFW was involved in the development of the protocol, selecting the references assessed bias in the studies and contributed in writing the manuscript. LS was involved in the development of the protocol, selecting the references assessed bias in the studies and contributed in writing the manuscript. MFW, LS and TJ performed the evaluation whether the robotic devices are commercial or not. KK performed the regression part of the analyses. VS assisted in performing the analysis and in imputing missing variables. MFW, LS, KK and VS all was greatly involved in writing the manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.