
Abstract
Background
Some studies have reported differentially altered neutrophil gelatinase-associated lipocalin (NGAL) levels in several malignancies. We evaluated NGAL measured in plasma or urine as both prognostic and diagnostic marker for different types of human tumors.
Methods
We performed systematic electronic searches in Medline, Embase and CRDTAS. Studies were included if they evaluated NGAL as a prognostic or diagnostic marker for human cancers. The selection of the studies, screening of the full texts and data extraction were conducted independently by 2 authors. We used the random-effects model for the meta-analyses. A methodological assessment was completed.
Results
We included 35 studies dedicated to colorectal, pancreas, breast, thyroid, gastric, kidney, endometrial, brain, liver, lung, esophageal, oral and ovarian cancers. Our meta-analyses showed that, in patients with colorectal and breast cancer, positive NGAL expression was associated with a decrease of disease-free survival (hazard ratio [HR] = 2.27, 95% confidence interval [95% CI], 1.54-3.36; HR = 1.78, 95% CI, 1.33-2.38, respectively). NGAL was a negative prognostic marker of overall survival in colorectal (HR = 2.37, 95% CI, 1.68-3.34) and endometrial (HR = 4.38, 95% CI, 1.9-10.12) cancers. Discriminative power of NGAL between cancer patients and control was moderate in colorectal cancer (area under the curve [AUC] = 0.6; pooled sensitivity 0.56; pooled specificity 0.72), acceptable in pancreatic cancer (AUC = 0.8; pooled sensitivity 0.6; pooled specificity 0.8) and good in thyroid cancer (AUC = 0.9; pooled sensitivity 0.85; pooled specificity 0.96).
Conclusions
NGAL determination in plasma and urine could be useful in the prognosis of colorectal and breast cancer, but its prognostic accuracy remains uncertain for other human tumors.
Introduction
Neutrophil gelatinase-associated lipocalin (NGAL) is a small protein, a member of the lipocalins family, which is a heterogeneous group of extracellular glycoproteins binding a variety of hydrophobic molecules, such as hormones, prostaglandins, arachidonic acid and retinoids (1). In spite of the fact that their amino acid sequences may differ greatly, they share the common structure of the “lipocalin fold” which consists of a highly symmetrical structure dominated by a single 8-stranded antiparallel β-sheet, closed back on itself to form a continuously hydrogen-bonded β-barrel, which encloses a ligand-binding site. Due to the diversity of the binding site structure, lipocalins can bind to ligands of different size, shape and chemical character, a property which is the basis of the multitude of their different functions (2). Lipocalins are involved in several physiological processes for cell homoeostasis maintenance, from immune response to bacterial infections, to a general clearance activity of endogenous and exogenous compounds, thanks to their transport capacity (1). NGAL is a costitutive component of neutrophils cytoplasmatic granules and its role in immune response is well known. NGAL chelates bacterial siderophores preventing iron availability for bacterial growth, so exerting a bacteriostatic effect (3). In contrast, in the presence of ferrous iron, NGAL is involved in iron uptake, regulating the iron-dependent growth pathways and blocking hypoxia-inducible factor 1α (HIF-1α) (3). However NGAL is expressed in a variety of cellular types besides neutrophils, and its levels are enhanced in a variety different acute and chronic pathological conditions – in particular, in kidney damage; in inflammatory, ischemic and metabolic diseases; in neurological diseases (4); and in tumor malignancies (5).
Nevertheless, regarding the state of the art, the only clinical use of the detection of NGAL in biological fluids seems to be to diagnose acute kidney damage, as its levels there correlate with the severity of renal injury, both in adults and in the neonatal population (6–8). NGAL concentration in blood and especially in urine seems to be a reliable tool in the early prediction of contrast-induced nephropathy (7). Haase-Fielitz et al concluded that notwithstanding the results of many clinical trials that were strongly in favor of NGAL as a predictive biomarker of acute kidney injury in different settings, further rigorously conducted clinical studies were required to verify the clinical efficacy of NGAL (7).
Recent research has highlighted how NGAL is involved also in the development, proliferation and invasiveness of human cancers. In fact, elevated levels of this protein have been detected in serum or urine of patients affected by different types of neoplasm such as colon, breast, brain, thyroid, esophageal and bladder cancer. NGAL, combining in a complex with matrix metalloproteinase-9 (MMP-9), could endorse cancer development. Obversely, inhibiting HIF-1α, the phosphorylation of focal adhesion kinase (FAK) and vascular endothelial growth factor (VEGF) synthesis, show an anticancer and antimetastatic effect (9). Furthermore, Candido et al reported that NGAL transcript level was higher in patients with solid tumors respect to healthy controls, and this expression corresponded to high protein levels in bladder, colorectal, liver, lung, ovarian and pancreatic cancer (9). In general, high concentrations of NGAL have been associated with advanced cancer and poor prognosis (3).
We evaluated NGAL as a prognostic and diagnostic biomarker in several types of human cancer with the ultimate aim to give a comprehensive picture of scientific findings about the clinical usefulness of NGAL as a biomarker in oncology.
Methods
We performed a systematic review and meta-analysis according to the recommendations indicated in the Cochrane Handbook for Diagnostic Test Accuracy (DTA) Reviews (http://srdta.cochrane.org/handbook-dta-reviews, accessed 28 December 2016), and we report data adapting the preferred reporting items from the systematic reviews and meta-analysis (PRISMA) checklist of Liberati et al (10) to studies of prognostic and diagnostic accuracy.
Search strategy
We searched the following electronic databases: Medline, Embase and the Cochrane Register of Diagnostic Test Accuracy Studies (CRDTAS), to identify all possible eligible studies. The search strategy adopted was carried out using the keywords “ngal,” “neutrophil gelatinase-associated lipocalin,” “LCN2 protein,” “cancer,” “tumour” and “neoplasm.” These were adjusted for all databases. Furthermore, we examined the reference lists of potentially eligible studies. The last search was run in July 2016.
Eligibility criteria
We included studies which conformed to the following eligibility criteria: studies that (i) were randomized or cohort studies; (ii) evaluated NGAL as prognostic or diagnostic biomarkers in human cancer; (iii) enrolled human patients who had not undergone cancer therapy before sample collection; and (iv) used immunoassay methodologies to measure NGAL levels, or immunohistochemical techniques to reveal NGAL expression in tissues. Eligibility was not restricted by type of publication, or patients' ages. We included only papers written in English, Italian, French or Spanish. We excluded studies on animal models and studies that evaluated molecular mechanisms for NGAL. Our approach was very inclusive, so as to obtain a pragmatic overall picture of research in this field.
Study selection
The literature search was performed by 1 author (V.P.). Two authors (L.R., V.P.) independently made a first selection of the elegible papers based on title and abstracts' content for eligibility. Subsequently, after the removal of duplicates, the authors reviewed the full texts of all potentially eligible studies for final inclusion. Disagreements between authors were resolved by consensus.
Data collection
Two authors (L.R., V.P.) independently extracted and entered into the standardized extraction form relevant publication details, regarding the study methods and the results. The authors collected data about (i) study characteristics (i.e., authors, year of publication, title, references, study design, type of cancer); (ii) patient characteristics (i.e., number of enrolled patients, age and sex); (iii) information about the method of NGAL assay; (iv) diagnostic data (i.e., true positive and negative, false positive and negative); (v) data about disease-free survival (DFS) and overall survival (OS); (vi) NGAL concentrations as reported in each study. Disagreements between authors were resolved by discussion.
Outcomes
The primary outcome was DFS and OS in patients with high levels of NGAL compared with those for patients with low or absent levels of marker. Then, we evaluated the diagnostic accuracy of NGAL in human cancer, defined as the number of true positives, false positives, true negatives and false negatives reported in each study. When these data were not available, they were calculated from sensitivity and specificity data.
Quality assessment
The methodological quality of the included studies was assessed independently by 2 reviewers (L.R., V.P.). Any disagreements were resolved through discussion.
We adapted the checklist “Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies” (available at http://www.nhlbi.nih.gov/health-pro/guidelines/in-develop/cardiovascular-risk-reduction/tools/cohort, accessed 28 December 2016). (Assessing Cardiovascular Risk. Systematic Evidence Review From the Risk Assessment Work Group. 2013 U.S. Department of Health and Human Services. National Institute of Health).
In particular, we considered the following questions:
Was the research question or objective in this paper clearly stated?
Was the study population clearly specified and defined?
Were all the subjects selected or recruited from the same or similar populations (including the same time period)?
Were inclusion and exclusion criteria for being in the study prespecified?
Were the outcome assessors blinded to the exposure status of participants?
Were key potential confounding variables measured and adjusted statistically for their impact on the relationship between exposure(s) and outcome(s)?
Were authors free from possible conflict of interest?
Statistical analysis
To investigate the effect of NGAL on OS and DFS, we pooled results in a meta-analysis and expressed the results as hazard ratios (HRs) with 95% confidence intervals (95% CIs) (11).
Given the wide range of patients and human cancers, other than the analytical method, we assumed a potential clinical heterogeneity. We assessed the presence of heterogeneity utilizing the I-squared statistic (I2), which indicated the percentage of variability due to between-study (or interstudy) variability. An I2 value greater than 50% was arbitrarily considered a high level of heterogeneity (12). In the absence of heterogeneity between studies, data were pooled using a fixed-effects model; otherwise, data were pooled using the random-effects model, as described by DerSimonian and Laird, allowing for differences in the effect from study to study (13). Potential sources of heterogeneity were explored through sensitivity analysis, noting whether studies used ELISA or immunohistochemistry to determined NGAL levels.
For diagnostic accuracy studies, we constructed 2 × 2 tables and pooled true positives, false positives, true negatives and false negatives, calculating sensitivity and specificity with 95% confidence intervals. We used random-effects bivariate models to create separate forest plots. We explored heterogeneity first through visual examination of the forest plot and then through the analysis of the receiver operating characteristics (ROCs) plot. Statistically heterogeneity was measured using I2 tests.
All analyses were performed using Review Manager (Rev-Man5), Stata 11 and Meta-Disc software. A p values less than 0.05 was considered statistically significant.
Results
Studies selection
The literature search from Medline, Embase and CRDTAS, after the exclusion of duplicates and irrelevant records, identified 894 bibliographical records. Of these, 819 were discarded because they did not meet the inclusion criteria. Seventy-five articles were considered eligible for inclusion, and their full texts were evaluated for details. Of these, 40 were excluded because they (i) evaluated NGAL as a marker of acute kidney injury (n = 4); (ii) evaluated the complex NGAL/MMP-9 (n = 6); (iii) studied only NGAL expression (n = 16); (iv) performed proteomic or correlation analysis (n = 2); (v) were reviews (n = 12). Finally, 35 studies were included (Fig. 1).
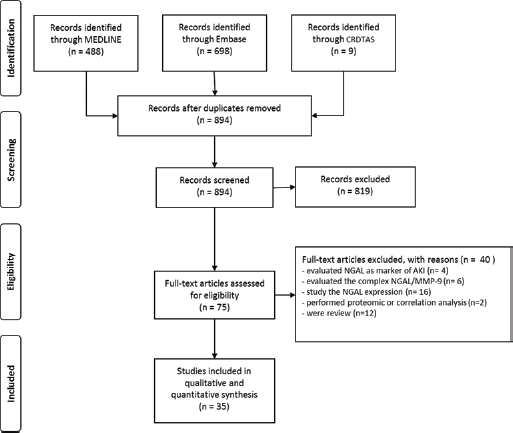
Flow diagram of study selection.
Characteristics of studies
We included 27 cohort studies, of which 5 utilized a prospective design (14–18), 6 utilized a retrospective design (19–24) and 16 were simply defined as cohort studies (25–40). We also included 7 diagnostic accuracy studies (41–47) and 1 case-control study (48). We evaluated studies on colorectal (n = 9), pancreatic (n = 5), breast (n = 4), thyroid (n = 3), kidney (n = 3), endometrial (n = 2), gastric (n = 2), ovarian (n = 2), brain (n = 1), liver (n = 1), lung (n = 1), esophageal (n = 1) and oral (n = 1) cancers. The included studies enrolled a total of 4,199 cancer patients, of which 54% were women. The number of participants ranged from 16 to 651, and their ages ranged from 3 to 91 years. All studies were conducted between 2008 and 2015. All studies assessing NGAL levels in biological fluids used an immunoassay; 12 of them reported the increment of NGAL in serum or urine of patients affected by breast (n = 2), colorectal (n = 2), ovarian (n = 1), pancreatic (n = 4) and renal cancer (n = 2) (data not shown). One study on gastric cancer assessed NGAL levels in tissue homogenates (18). Eleven studies out of 12 performed substantially the same ELISA assay to quantify total NGAL levels, while 1 out of 12 performed an immunoassay based on superparamagnetic beads coated with analyte-specific antibody (26), but this study did not report data for diagnostic accuracy, and accordingly it was not included in our valuation of diagnostic accuracy. The main characteristics of the included studies were reported in Table I.
Characteristics of included studies
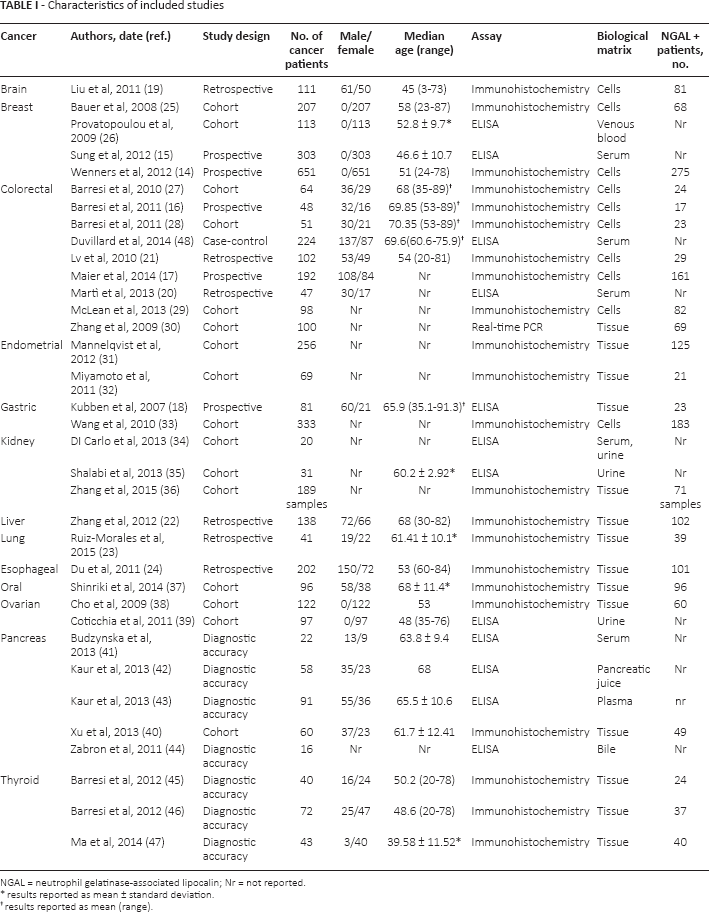
NGAL = neutrophil gelatinase-associated lipocalin; Nr = not reported.
results reported as mean ± standard deviation.
results reported as mean (range).
Quality assessment
Overall, most of the evaluated studies respected the criteria we considered for the methodology quality assessment. All authors reported the research question or the study's objective clearly. The study's population was clearly specified in 13 studies (37%), whereas the remaining studies reported this information partially. In 23 studies (65.7%) the patients' enrolment was performed satisfactorily, and in 11 studies, the information was only partially reported. The inclusion criteria were reported in only 4 studies; in 25 studies (71.4%), they were not reported and in 6 studies, they were partially reported. In the half of the studies (n = 17) the outcome assessor was blinded. Likewise, potential confounding variables were measured in 17 studies, but 18 studies did not consider them in the statistical analysis. In 20 studies (57%), the authors declared they did not have any conflict of interest, while in 15 studies they did not report whether they had any conflict of interest (see Supplementary Table I, available online at www.biological-markers.com – Evaluation of methodology quality of included studies).
Prognostic role of NGAL
High levels of NGAL, as determined by immunohistochemistry, were associated with a decrease of DFS in patients with colorectal cancer (HR = 2.27, 95% CI, 1.54-3.36; p<0.001, I2 = 0%, n = 2) (Fig. 2). In patients affected by breast cancer, the effect was not statistically significant (HR = 1.44, 95% CI, 0.94-2.20; p = 0.09, I2 = 83%; n = 3) (Fig. 3). In sensitivity analysis, after exclusion of the study by Sung et al (15), the effect was statistically significant for studies using immunohistochemistry to determine NGAL levels (HR = 1.78, 95% CI, 1.33-2.38, I2 = 0%, p<0.00001, n = 2).

Effect of NGAL expression on disease-free survival in patients with colorectal cancer.
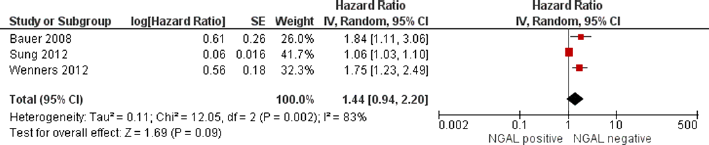
Effect of NGAL expression on disease-free survival in patients with breast cancer.
Meta-analyses revealed, also, a significant association between overexpression of NGAL, as determined by immunohistochemistry, and OS in patients with colorectal (HR = 2.37, 95% CI, 1.68-3.34, p<0.001, I2 = 25%; n = 3) (Fig. 4) and endometrial (HR = 4.38, 95% CI, 1.90-10.12; p = 0.0005, I2 = 0%; n = 2) (Fig. 5) cancers. In 2 studies that evaluated gastric cancer, using both assay methodologies, the association was not statistically significantly different (p = 0.65). A positive association between NGAL overexpression and OS was reported also in single studies on breast, kidney, liver, lung, esophageal, oral and pancreatic cancers (see Supplementary Figure I, available online at www.biological-markers.com – The effect of NGAL on overall survival in all evaluated cancers).
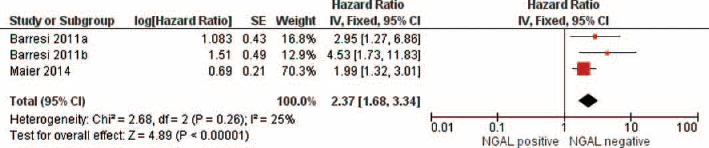
Effect of NGAL expression on overall survival in patients with colorectal cancer.

Effect of NGAL expression on overall survival in pat.
Valuation of the diagnostic accuracy
The diagnostic accuracy of NGAL measurement was evaluated in 7 diagnostic accuracy studies and 4 cohort studies on colorectal (16, 20, 30, 48), pancreatic (41–44) and thyroid (45–47) cancers.
In studies on pancreatic cancer using the ELISA method, the pooled sensitivity and specificity were 0.61 (95% CI, 0.54-0.68, I2 = 90.6%) and 0.77 (95% CI, 0.66-0.85, I2 = 66.6%), respectively, with substantial heterogeneity, whereas the AUC was 0.84 (SE = 0.035).
Studies on thyroid cancer determined NGAL with immunohistochemistry and reported a better diagnostic accuracy to discriminate patients with cancer; in fact pooled sensitivity was 0.85 (95% CI, 0.76-0.91, I2 = 0) and pooled specificity was 0.96 (95% CI, 0.9-0.99, I2 = 34.9%), while the AUC was 0.89 (SE = 0.13).
Discussion
This is the first systematic review that has evaluated the prognostic and diagnostic role of NGAL in several human cancers. Usually, the glycoprotein NGAL is considered as a biomarker for early detection of acute kidney injury in different clinical settings, such as cardiac surgery, contrast procedures, intensive care units and emergency departments (49), nevertheless some limitation to its use have been reported (50, 51).
The mechanisms underlying the way NGAL promotes human cancer has been explored in several studies (3, 5, 9), highlighting how NGAL furthers iron uptake from the extracellular space within the malignant cells to maintain multiplication of neoplastic cells (52). Growing evidence of NGAL playing a role in oncological diseases has opened up a new challenging field of scientific research. Surprisingly, this small protein shows both protumoral and antitumoral actions according to different types of cancer, and it has a heterogeneous expression in human cancers. NGAL has been found to be up-regulated in some types of cancer and to be down-regulated in others; thanks to the possibility of being detected both in blood and in urine, researchers have started focusing on NGAL as a novel noninvasive biomarker for cancer.
Two previous systematic reviews (53, 54) explored the overall accuracy of NGAL detection for the diagnosis and prognosis of breast and colorectal cancers. The authors reported a relationship between the up-regulation of NGAL and both types of cancer, suggesting NGAL as a potential diagnostic and prognostic biomarker, nevertheless its role needs to be further investigated.
Our systematic review summarizes the current available scientific evidence on NGAL evaluated as a biological marker for the diagnosis or prognosis of several human cancers. The meta-analysis showed that positive NGAL expression was associated with a decrease of DFS in patients affected by breast and colorectal cancers, advancing a predictive role of malignancy recurrence.
Likewise, our results revealed a significant association between NGAL overexpression and OS for colorectal and endometrial cancers, suggesting that it could be a useful marker to predict patient survival in these kinds of disease. This finding is also coherent with the positive association reported in single studies on liver, lung, esophageal, oral, pancreatic and kidney cancers. In contrast, our meta-analysis did not find any meaningful association between overexpression of NGAL and OS for gastric cancer.
The eligible papers allowed us to evaluate the diagnostic accuracy of NGAL in colorectal, pancreatic and thyroid cancers. In general, a moderate sensitivity and specificity, together with a moderate discriminative power of the ROC curve, was found in colorectal and pancreatic cancers. Instead, NGAL seems to perform better as a diagnostic biomarker for thyroid cancer. Four studies focusing on colorectal cancer reported data for diagnostic accuracy (16, 20, 30, 48): 2 of these quantified total NGAL in serum with different commercial ELISA assays (20, 48) and the other 2 were based on an immunohistochemical method (16) and real-time PCR (30). All 4 diagnostic accuracy studies on pancreatic cancer used the same commercial ELISA assay; diagnostic studies on thyroid cancer were based on an immunohistochemical methodology. This characteristic probably did not affect the meta-analysis but may explain, at least in part, the low sensitivity we found for colorectal and pancreatic cancers. Moreover the cutoff used to discriminate the NGAL concentration in serum or urine of the healthy population from patients was not always specified, or it was different.
Overall, NGAL levels were measured using the same ELISA in 9 out of 11 studies (15, 18, 34, 39, 41–44, 48); while in 2 cases it was performed using a different commercial kit (20, 35), 1 study was based on an immunoassay using superparamagnetic bead technology, which was performed on a fully automated platform (26). Conversely, as far as we can deduce from the papers, it is likely that the immunoassays were all performed manually. ELISA technology applied to peptide and protein hormones determination has nowadays reached high sensitivity and specificity levels, and when performed on automatic analyzers, accuracy improves. It is well known that, in general, differences in results obtained by different immunoassays are mainly due to lack of standardization and to different assay design. Nevertheless, the assay has been used to detect the analyte in different biological fluids but a consensus on the most suitable biological matrix for testing and, the related diagnostic threshold are still an open question. Moreover, the existence of different molecular forms of NGAL and their expression in various disease states further complicates the interpretation of the results; the immunoassays used in the studies seem to detect the total NGAL; nevertheless, one form of the hormone may be predominant in a different matrix, affecting the clinical performance of the assay according to the antibody configuration.
Despite these methodological issue, there is a substantial consistency in the conclusions reported by studies. Indeed, studies on breast disease suggest the usefulness of NGAL in monitoring disease progression (26) and the association of NGAL with reduced survival (15). NGAL levels were found to increase in patients with colorectal cancer (20, 48) even though it does not seem to be suitable as a diagnostic biomarker (48). Obversely it can have a prognostic utility in metastatic patients (20). NGAL levels in gastric tumor tissue are associated with worse survival (18). In kidneys, NGAL is not useful for diagnosing renal cell carcinoma (34), but it may be helpful to select a proper therapy in cases of metastatic disease without the need for pretreatment biopsy (35). NGAL can be a diagnostic biomarker of advanced or recurrent ovarian cancer (38). Finally, biliary NGAL has a potential role in distinguishing benign from malignant biliary obstructions (41, 42, 44), and it can be a serum diagnostic biomarker of pancreatic cancer (43). All authors agree on the need for further validation of their findings.
Our meta-analysis presents some limitations that should be considered. First, studies that matched the inclusion criteria were very few, and we included single studies for liver, lung, esophageal, oral, pancreatic and kidney cancers, limiting the overall evaluation of NGAL. Second, the sample size of the studies included was small, reducing the statistical power to evaluate the effect. Third, the studies included lacked some important information, especially about clinically outstanding confounders such as previous therapeutic treatments and comorbidities. Indeed, NGAL is enhanced in a variety of pathophysiological conditions such as diabetes, systemic infections, urinary tract infections and, more generally, in all conditions inducing inflammation and activation of neutrophils. Fourth, the definition of immunostaining scores and related cutoffs for the definition of positive expression of NGAL was not always homogeneous between studies.
The interpretation of our meta-analyses needs prudence. In fact, for most of the human cancers evaluated, the inclusion of single studies enrolling a limited number of patients influenced the results by overestimating the effect size. A previous study showed that the effect of small trials is prominent in meta-analyses, in as much as small studies exaggerate the effect (55). Furthermore, small studies are affected, usually, by lower methodological quality compared with large studies, and this issue must be taken into consideration in the interpretation of the results.
In conclusion, NGAL is expressed differently in several human cancers. Our analysis showed that high NGAL levels in biological fluids could be useful to predict DFS for patients affected by colorectal and breast cancer, but its prognostic and diagnostic accuracy remains uncertain for other human tumors.
Footnotes
Financial support: No specific funding was received for this work.
Conflict of interest: The authors state that there are no conflicts of interest regarding the publication of this article.