
Abstract
Background
Serum biomarkers may help to discriminate malignant from benign adnexal masses with equivocal features on imaging. Adequate discrimination of such tumors is crucial for referring patients to either a specialized cancer center or a nonspecialized gynecology service.
Aim
We aimed to investigate whether the preoperative level of serum C-reactive protein (CRP), alone or combined with CA125 and menopausal status in the Ovarian Score (OVS), is useful in the prediction of malignancy in women with ovarian tumors.
Methods
This cross-sectional study included 293 patients who underwent surgery in a tertiary cancer center. Receiver operating characteristic (ROC) areas under the curves (AUC) for CRP, CA125 and OVS were calculated in different scenarios, as well as their sensitivity and specificity, using standard cutoff points (for CRP, 10 mg/L; for CA125, 35 U/mL).
Results
CA125 and the OVS performed significantly better than CRP alone in the differentiation of benign disease from epithelial ovarian cancer (EOC) (AUC = 0.86 for CA125, 0.79 for OVS, and 0.73 for CRP). OVS and CRP alone were superior to CA125 only in the differentiation of borderline ovarian tumors from advanced stages of EOC and non-EOC. Sensitivity and specificity were 52.5% and 83%, respectively, for CRP, 77.9% and 66.7% for CA125, and 71.3% and 67.8% for OVS.
Conclusions
OVS is as good as CA125 in the differentiation of benign tumors from ovarian cancer. The addition of CA125 and menopausal status to CRP enhanced the relatively low discriminatory power of isolated CRP.
Introduction
Ovarian cancer (OC) remains the most lethal gynecological cancer worldwide, with 238,719 estimated new cases and 151,917 deaths each year (1). The majority of patients are diagnosed at advanced stages and less than 30% of them survive after 5 years (2). Proinflammatory processes elicited by ovulation, endometriosis, pelvic inflammation and polycystic ovarian syndrome have been proposed as potential pathways involved in the pathogenesis of OC (3, 4). The inflammatory response promotes carcinogenesis by the induction of genomic instability and epigenetic alterations, leading to inappropriate gene expression, which stimulates angiogenesis, cell proliferation and inhibition of apoptosis in cancer cells. A similar chronic inflammation environment is often found in tumor tissues (5, 6).
Serum biomarkers can be useful to assist in the diagnosis of a benign or malignant ovarian tumor together with clinical and ultrasound exams. Although OC is a rare entity, pelvic masses are a relatively common finding in pre- and postmenopausal women, being more frequent in premenopausal women. Moreover, it is estimated that 5%-10% of women will be submitted to surgery due to a pelvic mass in their lifetime (7) and approximately 30% of postmenopausal women referred to surgery will be diagnosed with a malignant tumor (8). Preoperative identification of malignant tumors allows patient referral to a tertiary hospital, where they can be operated on by a gynecological oncologist, with improvement of survival, while benign tumors may be surgically removed with a minimally invasive approach (laparoscopy) in a secondary center (9–11).
Serum C-reactive protein (CRP) is a sensitive indicator of acute and chronic inflammation, and is used routinely in several acute and chronic inflammatory diseases. Its production by hepatocytes as part of the inflammatory response is expected when tissues are damaged by an infection, trauma or malignant disease (4, 5). Some studies have already investigated the elevated circulating levels of CRP in OC settings. These studies showed a positive correlation between CRP and OC; however, it must be emphasized that they evaluated prediagnostic serum to assess the cancer risk, but were not designed to examine whether women with adnexal masses should undergo surgery (4, 12–15). Higher levels of CRP are related to advanced disease, worse prognosis (16), and decreased progression-free survival and overall survival (17), but little is known about the role of the biomarker in the preoperative setting (18, 19).
CA125 is a well-established biomarker that is used in the management of women with epithelial ovarian cancer (EOC). It has been useful in monitoring response to chemotherapy, in the diagnosis of OC recurrence, and in the prediction of disease prognosis. It also plays a role in the discrimination of malignant from benign pelvic masses in preoperative settings (20, 21). However, because of its low specificity, mainly in premenopausal women (as it presents higher concentrations in many benign gynecological diseases and conditions such as menstruation, uterine myoma and endometriosis), other biomarkers have been tested to enhance the performance of CA125 alone. In addition, the CA125 level is elevated in 85% of advanced OCs but shows low sensitivity in the initial stages of the disease, which account for about 50% of cases (22).
The association of different systemic inflammation-related biomarkers in the evaluation of women with OC is useful to assess treatment response and prognosis; however, as a preoperative test, we should choose more simple associations of biomarkers, considering the costs, availability and reproducibility in clinical practice, especially in underresourced settings.
The goal of this study was to determine the role of CRP measurement in the prediction of malignancy in women with ovarian tumors compared to the gold-standard biomarker for ovarian tumors, CA125. In addition, the Ovarian Score (OVS), comprising CRP, CA125 and menopausal status, was used to ascertain whether this association is superior to the biomarkers alone.
Patents and methods
Patients
This cross-sectional study was conducted from January 2010 to November 2014 at the Women's Hospital (CAISM), State University of Campinas, a tertiary cancer center specialized in gynecological malignancies. The University Research Ethics Committee (number 1092/2009) approved the study. Women referred to the pelvic oncology clinic because of pelvic or adnexal masses were included in this study after having given their signed consent, and were submitted to the study protocol. In brief, patients underwent pelvic examination including ultrasound examination of the pelvis. The following ultrasound parameters were used to decide which women should undergo surgical treatment: largest diameter of the lesion; maximum diameter of the largest solid part; if unilocular or multilocular; number of papillary projections; acoustic shadows; presence of ascites; color-Doppler blood flow. Blood samples were collected for serum marker measurement and archival purposes. When indicated, diagnostic and/or therapeutic surgical procedures were scheduled. When surgery was not indicated, women were scheduled for clinical follow-up. Women with tumors more likely to be benign waited for nonpriority surgeries. Those with a moderate or high risk of malignancy underwent surgery earlier, as previously described (23).
From 785 consecutively enrolled women, we excluded those with no surgical indication (306 women), those without CA125 and/or CRP results (149), and those who had extraovarian tumors (37), whether benign (uterine leiomyoma, tubal cysts, sactosalpinx) or malignant (pseudomyxoma peritonei, carcinomas of gastrointestinal origin). The biopsy specimens of these extraovarian tumors were collected from sites other than the ovaries. Percutaneous biopsies of pelvic masses or abdominal implants were performed in 22 cases of nonresectable ovarian tumors. Bilateral tumors were found in 64 women; for categorization purposes, the tumor with the worst prognosis was taken into account. Postmenopausal status was defined as >1 year of amenorrhea or ≥50 years of age in the case of a previous hysterectomy.
As proposed by Nik et al (24), we classified as type I EOC low-grade endometrioid, low-grade serous, clear cell, and mucinous carcinomas. Type II EOCs were high-grade serous and endometrioid carcinomas, undifferentiated carcinomas, and carcinosarcomas.
Methods
Blood samples collected from patients were stored in serum separator tubes. They were left to clot for at least 30 minutes before centrifugation. Blood samples were centrifuged at 1300g for 10 minutes, and serum was separated into aliquots and stored at -80°C until the analysis of biomarkers. The mean time elapsed between blood collection and surgery was 69 days, ranging from 24 hours or less for emergency procedures to a maximum of 119 days (90% central range = 40 to 75 days).
C-reactive protein
Serum CRP was measured by means of the high-sensitivity CRP test, a method using the immunoturbid metric assay in an automatic analyzer (MODULAR ANALYTICS P800 Module; Roche Diagnostics GmbH). Values were expressed in mg/L.
CA125
Serum CA125 was determined by means of the CA125 II test, using the chemiluminescence technique in the Cobas e 411 automatic analyzer (Roche Diagnostics GmbH) according to the manufacturer's instructions. Values were expressed in U/mL.
Statistical analysis
Data were analyzed using the R Environment for Statistical Computing software (25). Statistical calculations were performed using 95% confidence intervals (CIs), considering p values <0.05 as significant. Ovarian tumors were classified into nonneoplastic, benign, borderline ovarian tumor (BOT), malignant, and metastatic according to the histopathological diagnosis (Supplementary Figure S1 - Ovarian tumors stained with hematoxylin and eosin from women with elevated serum CRP levels. Available online at www.biological-markers.com). For analytic purposes, tumors were grouped into benign (nonneoplastic and benign) and malignant (BOT, malignant and metastatic). The clinical characteristics of the groups classified as benign or malignant were compared using the chi-square test. A simple score recently described by Watrowski and Zeillinger (18) was modified in our study to OVS, in order to test the association of CA125 and CRP levels and menopausal status. These 3 parameters were dichotomized according to CA125 (35 U/mL as cutoff), CRP (10 mg/L as cutoff) and menopausal status, assigning a score 1 to marker values above cutoff and to postmenopausal status. OVS thus ranged from 0 to 3, with scores 0-1 classified as negative and scores 2-3 classified as positive. Next, we calculated the receiver operating characteristic (ROC) areas under the curves (AUC) for CRP, CA125, and OVS in different scenarios. We compared the AUCs using the DeLong method (26). We then calculated the sensitivity and specificity for CRP, CA125 and OVS using the standard cutoff points above. We next depicted the ROC curves for CRP and CA125 for the complete cohort, and then for the pre- and postmenopausal subsets of women.
Results
Among the studied sample of 293 women, 41.6% presented malignant tumors. Women with malignant ovarian tumors were significantly older (mean 55.4 vs. 47.2 years, p<0.01) and significantly more often postmenopausal (66.9% vs. 48%, p<0.01). Neither body mass index nor a history of close relatives with breast cancer or OC were related to tumor malignancy. Most malignant (74.6%) and benign (39%) tumors were epithelial. In women with nonneoplastic masses, 19 were diagnosed with endometriomas, 9 with functional cysts, and 10 with other minor categories. Of the malignant tumors, 54.1% were at stage I or II. The distribution of histological types in women with stage I-II tumors was 49.2% EOC, 26.2% BOT and 24.6% non-EOC. In women with stage III-IV tumors, 63.6% were EOC, 23.6% metastases, 9.1% BOT and 3.6% non-EOC. Most women with malignant tumors had elevated levels of CA125 (77.9%) compared to those with benign tumors (33.3%) (p<0.01). The same was true for CRP levels: 52.5% of women with malignant tumors had elevated levels of the serum marker compared to only 17% of the women with benign tumors (p<0.01). Most women with ovarian metastases had elevated levels of CA125 (≥35 U/mL) (84.6%) and CRP (>10 mg/L) (61.5%) (Tab. I).
Key clinical features of women by tumor type (benign or malignant)
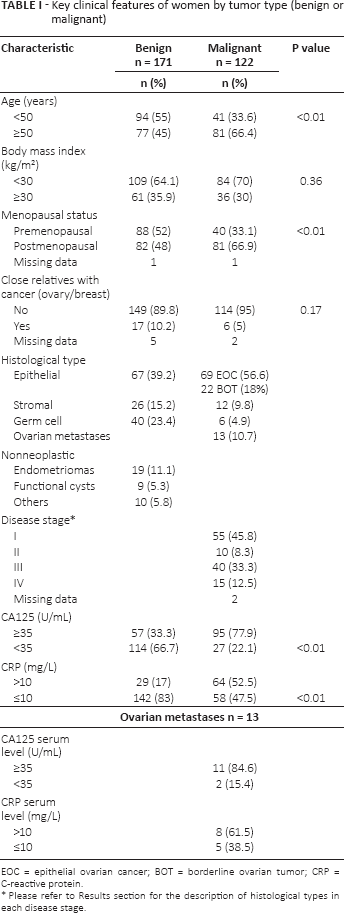
EOC = epithelial ovarian cancer; BOT = borderline ovarian tumor; CRP = C-reactive protein.
Please refer to Results section for the description of histological types in each disease stage.
In Table II, the median (with interquartile range) and mean (with standard deviation) serum concentrations of CRP and CA125 are presented according to the histological classification of the tumors. Table III shows the significance values for pairwise comparisons of the CA125 and CRP levels in the different histology strata. CRP levels were significantly higher in women with metastatic tumors when compared to EOC, non-EOC, BOT, benign and nonneoplastic tumors (p<0.01). In addition, CRP levels in women with EOC were significantly higher than those in women with benign and nonneoplastic tumors (p<0.01). CA125 levels were also significantly higher in women with EOC than in women with benign and nonneoplastic tumors (p<0.01).
Serum concentrations of CRP and CA125 according to histological diagnosis
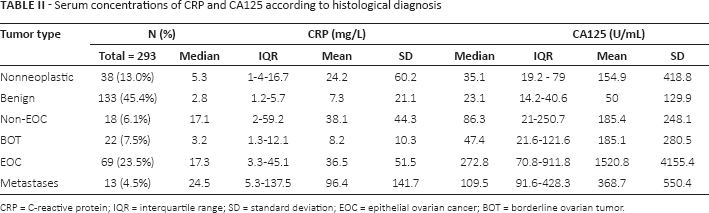
CRP = C-reactive protein; IQR = interquartile range; SD = standard deviation; EOC = epithelial ovarian cancer; BOT = borderline ovarian tumor.
Significance values for pairwise comparisons of serum marker levels in different histological strata
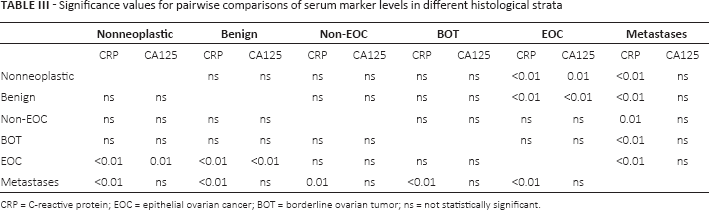
CRP = C-reactive protein; EOC = epithelial ovarian cancer; BOT = borderline ovarian tumor; ns = not statistically significant.
In Table IV, we show the AUCs for CA125, CRP and OVS calculated for the discrimination of different subsets of histological diagnoses. P values comparing the AUCs for CA125, CRP and OVS were calculated using the DeLong method (26). CA125 and OVS performed significantly better than CRP in the differentiation of benign ovarian diseases from OC + BOT, as well as in the discrimination of benign tumors from EOC. CA125 alone was superior to OVS in the differentiation of benign tumors from BOTs. CA125 and OVS performed better in the discrimination of benign tumors from type II EOC, although only CA125 was superior to CRP in the discrimination of benign tumors from type I EOC. CA125 performance was superior to OVS in the differentiation of BOT from early-stage OC. Of note, CRP and OVS performed significantly better than CA125 in the differentiation of BOT from advanced-stage OC. CA125 was superior to OVS in the discrimination of metastases from OC both at early and advanced stages. CA125 performed better than CRP in the differentiation of metastases from advanced-stage OC.
Polytomous discrimination performance of CA125, CRP and OVS
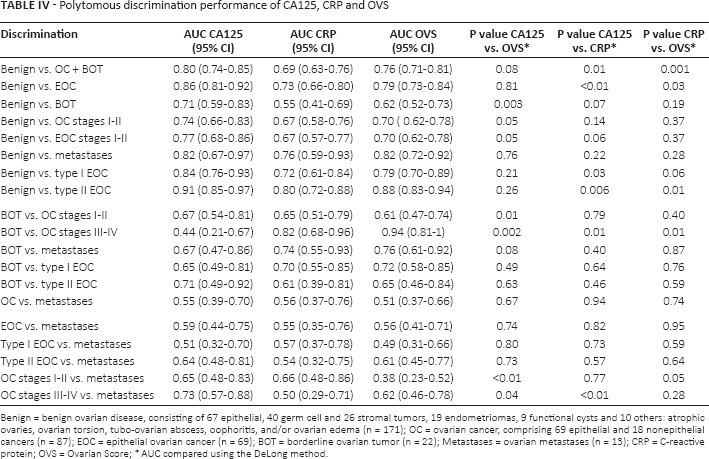
Benign = benign ovarian disease, consisting of 67 epithelial, 40 germ cell and 26 stromal tumors, 19 endometriomas, 9 functional cysts and 10 others: atrophic ovaries, ovarian torsion, tubo-ovarian abscess, oophoritis, and/or ovarian edema (n = 171); OC = ovarian cancer, comprising 69 epithelial and 18 nonepithelial cancers (n = 87); EOC = epithelial ovarian cancer (n = 69); BOT = borderline ovarian tumor (n = 22); Metastases = ovarian metastases (n = 13); CRP = C-reactive protein; OVS = Ovarian Score;
AUC compared using the DeLong method.
For the discrimination of benign from malignant ovarian tumors, CRP had a sensitivity of 52.5% and a specificity of 83%, compared to 77.9% and 66.7%, respectively, for CA125, and 71.3% and 67.8%, respectively, for OVS.
Figure 1 shows the comparison of ROC curves for CA125 and CRP for the discrimination of benign from malignant ovarian tumors in the whole cohort and in the subsets of pre- and postmenopausal women. The best AUC for CRP was obtained in postmenopausal women (AUC = 0.73 compared to 0.66 in premenopausal women and 0.69 in the entire cohort), although CA125 performed better than CRP in all studied situations.
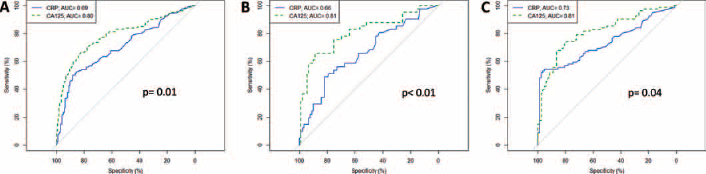
ROC curves for CA125 and CRP in the complete cohort (A), premenopausal (B) and postmenopausal (C) women. ROC = receiver operating characteristic; CRP = C-reactive protein; AUC = area under the curve.
Discussion
Our study shows that measurement of CRP, a low-cost, widely available serum biomarker test, when associated with CA125 and menopausal status, may be of some clinical value for women with adnexal masses. In general, biomarkers can be useful in the preoperative evaluation of adnexal masses, helping to decide whether surgery or surveillance is more appropriate, considering that most operated pelvic masses are benign and the morbidity of surgical procedures is significant.
Similar to other biomarkers, it is not correct to classify any value as “normal” for CRP. A minor elevation (3-10 mg/L), found in a third of Americans, is associated with dietary patterns and noninflammatory conditions that can lead to mild tissue injury. The latter phenomenon may precede disease onset. Consequently, this minor elevation of CRP is related to an increased risk in healthy people of developing diseases, and it predicts a worse prognosis and mortality in healthy and diseased people (27). Moreover, ethnic variations are responsible for different values of CRP among studies. In Chinese populations, the mean serum concentration of CRP in patients with EOC was 14.32 mg/L (16), while in a report of Caucasian cases it was 36 mg/L (28), which is similar to our findings (36.5 mg/L).
Hefler-Frischmuth et al (19) in a retrospective study observed a doubled CRP serum level in women with malignant tumors (1 mg/dL) compared to those with benign tumors (0.5 mg/dL). In our analyses, women with benign tumors had CRP levels similar to women with BOTs (3.2 mg/L), whereas women with EOC (17.3 mg/L) had significantly higher levels of CRP. Hefler-Frischmuth et al obtained similar results to ours in the differentiation of benign tumors from EOC, AUC = 0.90 for CA125 and AUC = 0.73 for CRP (19). However, we were unable to reproduce their results when CRP, CA125 and age were combined in a ROC curve, with an AUC of 0.92. They found that CRP levels were independently associated with the prediction of malignancy, suggesting that this biomarker could be a useful tool in the differential diagnosis of pelvic masses (19).
Watrowski's score was an association of preoperative platelet count, CRP, fibrinogen and CA125 levels (18). The association of these 4 parameters resulted in a higher specificity (94% for Watrowski score and 80% for CA125) but lower sensitivity than CA125 alone (76% for Watrowski score and 93% for CA125). Higher sensitivity is crucial in the preoperative setting, since false negatives in this case are related to delay in appropriate treatment and worsening of disease prognosis. In our study, we obtained a sensitivity for OVS of 71.3%, slightly inferior to that for CA125 alone (77.9%), with the same specificity (67.8% for OVS and 66.7% for CA125). However, our study population differs from that studied by Watrowski and Zeillinger (18), as our sample presented a higher number of BOTs and stage I-II OC. Another notable difference is that we included ovarian metastases in the analyses. Our study also differs from Watrowski-Zeillinger's in the cutoff points used for CRP (5 mg/L in their study, 10 mg/L in our study). In addition, we chose to use menopausal status, as we obtained an improvement in the performance of isolated CRP in the discrimination of pelvic masses in this subgroup of women.
In 2004, Shih and Kurman first proposed a dualistic model of epithelial ovarian carcinogenesis – type I and type II – based on morphological and molecular genetic analysis (29). The same authors (30) suggested that risk factors for type I and type II are endometriosis and lifetime ovulation cycles, respectively, both being associated with inflammation. Regarding the differentiation of benign from type I tumors, one could expect that CRP would have a determinant role; however, CA125 alone was superior to CRP in this scenario. In addition, we found that CA125 and OVS were superior to CRP alone in the differentiation of benign tumors from type II EOC.
A weak point of our study was that, unlike other authors (4, 14), we did not exclude women who were using hormonal therapy. The use of oral estrogen replacement enhances CRP levels by a first-pass hepatic effect (31), which could be a potential confounding factor. In addition, CRP and CA125 tests can give false positive results; we must therefore interpret any test results with caution, always taking into account imaging, clinical examination and the possible presence of conditions and diseases that may enhance biomarker levels.
It is important to emphasize that our sample was relatively rich in stage I-II tumors (54.1%), which is an uncommon feature in OC studies. Early-stage OC is potentially curable, and we provide a reliable estimate of CRP and CA125 behavior in this subset of women. In our study, CA125, CRP and OVS showed similar performance in the differentiation of benign ovarian disease from stage I-II OC. In the differentiation of BOTs from early-stage OC, CA125 performed better than OVS but was equivalent to CRP.
The correct discrimination between primary ovarian neoplasia and ovarian metastases is also key to the correct referral of women with ovarian tumors. In the case of suspected ovarian metastases, complementary exams such as colonoscopy, computed tomography of the abdomen, mammography and magnetic resonance should be requested (32).
Our results showed a predisposition to elevated CRP levels in women with ovarian metastases. CRP elevation has been reported as a risk and prognostic factor in other cancers such as colon (33, 34), breast (35) and uterine (36) carcinomas, which were the primary tumors of our ovarian metastases sample. If we consider that CRP levels increase as the disease progresses, as reported in OC studies (16, 28), the fact that metastatic disease expresses higher levels of CRP was already expected.
In conclusion, OVS is as good as CA125 for the differentiation of benign adnexal masses from OC. In this setting, the addition of CA125 and menopausal status to CRP enhanced the relatively low discriminatory power of isolated CRP. However, CRP and OVS may be useful in the even less frequent situation of women with disseminated, nonresectable intraabdominal disease and a pathological diagnosis of BOT. For these cases, elevated CRP levels may suggest that invasive disease was missed during surgical/pathological evaluation, and chemotherapy may be considered as a treatment option.
Footnotes
Abbreviations
Financial support: The São Paulo Research Foundation, FAPESP number 2012/15059-8, funded this study.
Conflict of interest: The authors declare that they have no conflict of interest.