
Abstract
Objective
To analyze the utility of carbohydrate antigen (CA)125 and human epididymis protein 4 (HE4) to detect malignancy in women with ovarian endometriosis, when ovarian cancer is suspected and ultrasonography results are inconclusive.
Methods
Women who underwent surgery between 2015 and 2019 for ovarian endometriosis or for adnexal masses, with a final diagnosis of ovarian carcinoma (clear cell and endometrioid) were included in this retrospective study. The women were divided into three groups: ovarian endometriosis (OE), ovarian carcinoma without endometriosis (OC), and ovarian carcinoma with endometriosis (OC + E). Adnexal masses were assessed preoperatively by transvaginal ultrasonography according to the International Ovarian Tumor Analysis (IOTA) simple rules, and CA125 and HE4 blood levels were obtained.
Results
Of 208 women, 45 had malignancy, 16 in the OC + E group and 29 in the OC group. According to transvaginal ultrasonography, 13 were classified as undetermined risk of malignancy: OC group: 3, OE group: 3, and OC + E group: 7. When we compared the tumor biomarkers, significant differences in HE4 but not in CA125 levels were found between the groups.
Conclusions
When ovarian malignancy is suspected in patients with ovarian endometriosis, HE4 is a more useful tumor biomarker to diagnose OC when ultrasonography results are inconclusive.
Keywords
Introduction
Ovarian cancer is the seventh most common cancer in women and the eighth leading cause of cancer death worldwide. 1 More than 70% of ovarian cancer cases are diagnosed at an advanced stage, and no tools are available for detecting ovarian cancer at an early stage. 2 Although endometriosis is a benign condition, it shares pathophysiological features with cancer, 3 and ovarian cancer can occur in 0.5% to 1% of patients with endometriosis.2,4,5 Epithelial ovarian cancer, known as endometriosis-associated ovarian carcinoma, is the most frequent cancer and includes serous clear cell and endometrioid carcinomas. Clear cell carcinoma and endometrioid carcinoma are the subtypes that are most likely to coexist with endometriosis.2,4
Because ovarian cancer and endometriosis may occur concomitantly, it is very important to discriminate suspected malignancy from endometriosis. Imagining techniques, such as transvaginal ultrasonography, are the gold standard for the study and diagnosis of adnexal masses. The International Ovarian Tumor Analysis (IOTA) group ultrasonography rules for ovarian masses classify ovarian masses into benign, malignant, or inconclusive using a simple set of ultrasonography-based rules; 6 nonetheless, the diagnosis in up to 25% of masses is inconclusive. 7
Apart from imaging, several tumor markers for epithelial ovarian cancer have been described for use in ovarian cancer diagnosis and follow-up, and carbohydrate antigen 125 (CA125) is most widely used. 8 Nevertheless, high levels of CA125 have been found in patients with endometriosis without malignancies. Considering that patients with endometriosis have an increased risk of developing ovarian cancer, and that endometriosis alone can increase CA125 levels, additional tumor markers are needed. In the last decade, the human epididymis protein 4 (HE4) biomarker has shown higher specificity than CA125 (0.93 vs 0.75, respectively), and improved the detection of malignancy in patients with adnexal masses.9–12 HE4 levels are not affected by the menstrual cycle, hormonal treatment, or endometriosis. 13 Therefore, HE4 could be a helpful tumor marker in patients with endometriosis and suspected malignancy as an add-on assessment to ultrasonography. Many algorithms have been reported in the literature to better assess the risk of ovarian cancer. One of these is the risk of ovarian malignancy algorithm (ROMA), which includes CA125, HE4, and menopausal status, and which has high sensitivity and specificity. 14 However, there are limited data regarding the role of ROMA in endometriosis patients.
The aim of this study was to analyze the utility of CA125 and HE4 to detect malignancy in patients with ovarian endometriosis, when ovarian cancer is suspected and ultrasonography results are inconclusive.
Material and methods
Study design and participants
This study was conducted in a tertiary university hospital. Patients comprised all women with ovarian endometriosis who underwent surgery with histologic confirmation of ovarian endometriosis (study group) between 2017 and 2019. The control group comprised women who underwent surgery for adnexal masses with the histopathological diagnosis of endometrioid or clear cell ovarian cancer between 2015 and 2019. All data were recorded prospectively. The only exclusion criterion was the presence of renal impairment.
According to the pathological results, patients were divided into three groups: ovarian carcinoma (OC) without endometriosis, ovarian carcinoma with endometriosis (OC + E), and ovarian endometriosis (OE) without malignancy.
The reporting of this study conforms to the STROBE guidelines 15
HE4 and CA125 analysis and ROMA risk calculation
Preoperative HE4 and CA125 levels were recorded for all patients, and both markers were measured using a chemiluminescent enzyme immunoassay (EIA) (Architect® Analyzer; Abbott Laboratories, Chicago, IL, USA) according to the manufacturer’s instructions. For CA125, the upper limit of normal was 40 U/mL, and for HE4, the upper limit was 70 pmol/L for premenopausal women and 150 pmol/L for postmenopausal women, all according to cut-offs reported by the assay manufacturer. ROMA risk was calculated according to the manufacturer’s calculator, with a cutoff value of ≥11.4% in premenopausal women and ≥29.9% in postmenopausal women.
Transvaginal ultrasonography
All transvaginal ultrasonography was performed in the same hospital by two trained ultrasonographers (MR, CR), using a microconvex endocavity probe (type RIC5-9, Voluson-V730 Expert; GE, Munich, Germany). The examinations were interpreted in real-time. Adnexal masses were evaluated and interpreted according to the IOTA group directions and were classified according to the simple rules for ovarian masses described by this group. 6
Level of risk assessed by transvaginal ultrasonography and tumor biomarker levels were compared between the three groups.
Statistical analyses
Statistical analysis was performed with the SPSS software package (version 19.0; IBM Corp., Armonk, NY, USA). Values from quantitative parameters were expressed as mean and standard error (SE), or median and interquartile range (IQR); and values from qualitative parameters were expressed as number and frequency. Continuous variables were analyzed using Student’s t-test or the Mann−Whitney test, as appropriate. Categorical variables were analyzed using Fisher’s exact test and were expressed as odds ratios with 95% confidence intervals, using the Mantel–Haenszel test. Results were considered statistically significant with p < .05 (two-sided).
Ethical approval
The Ethics Committee of the Hospital Clínic de Barcelona approved the study (approval number: HCB/2019/1152), and written informed consent was obtained from all participants.
In accordance with the journal’s guidelines, we will provide our data for the reproducibility of this study in other centers, if requested.
Results
A total of 208 patients were included in this study, with a mean age of 41.57 ± 12.30 years. According to the pathological reports, 29 (14%) patients had OC, 16 had OC + E (8%), and 163 had OE (78%). A summary of the patients’ demographic and clinical data is shown in Table 1. OC and OC + E patients were significantly older than the OE patients at surgery (p < .001). Accordingly, patients with OC were more frequently in menopause than patients with OE (82.8% vs. 4.9%, respectively; p = .02). No differences regarding smoking status or parity were found.
Characteristics of the women included in this study.

*When the surgery was performed.
OC, ovarian carcinoma; OC + E, ovarian carcinoma with endometriosis; OE, ovarian endometriosis; ns, non-significant; SE, standard error.
Pathological findings
Forty-five patients had malignancy in the final pathological report: 29 patients had endometrioid carcinoma (64.4%), and 16 patients had clear cell carcinoma (35.6%). Among the 45 patients, it is noteworthy that 16 patients (35.6%) had concomitant endometriosis findings; i.e., OC + E. In this subgroup of patients, 11 (68.8%) had endometrioid carcinoma, and 5 (31.2%) had clear cell carcinoma.
Ultrasonographic findings
For discriminating presurgically between benign and malignant adnexal masses, the patients were evaluated according to the IOTA simple rules for ovarian masses. Overall, 25 patients (86.2%) in the OC group and 7 patients (43.8%) in the OC + E group where at high risk of malignancy vs. no patients in the OE group (Table 2). Thirteen patients were classified as “undetermined risk of malignancy”; thus, requiring further evaluation. Of these patients, 3 had OC, 7 had OC + E, and 3 had OE (p < .01).
Risk of malignancy according to the IOTA simple rules in the three groups.

IOTA, International Ovarian Tumor Analysis; OC, ovarian carcinoma; OC + E, ovarian carcinoma with endometriosis; OE, ovarian endometriosis.
Tumor biomarkers: CA125 and HE4, and ROMA risk.
To further elucidate the diagnosis, the levels of the tumor biomarkers for epithelial ovarian cancer were measured prior to surgery, and the ROMA risk was evaluated (Table 3). Among all of the patients, CA125 levels were elevated in 101 (48.5%) patients, and 52 patients (25%) showed elevated levels of HE4. The mean serum CA125 and HE4 levels in the OC and OC + E patients were significantly higher than those in the OE patients. Most of the patients in the OC (89.6%) and OC + E (93.7%) groups had a high risk of malignancy according to ROMA, whereas nearly 10% of the patients in the OE group had a high risk.
Serum CA125 and HE4 levels and high-risk ROMA status in patients with OE, OC, or both.

ROMA, risk of ovarian malignancy algorithm; IQR, interquartile range; OC, ovarian carcinoma; OC + E, ovarian carcinoma with endometriosis; OE, ovarian endometriosis; CA125, carbohydrate antigen 125; HE4, human epididymal protein 4.
In the OE group, 10 patients (6.1%) had elevated levels of HE4 (p < .05), while 67 patients (41.1%) had elevated levels of CA125 (p = .002) (Table 4). Although both CA125 and HE4 levels were significantly different between the three groups (p < .05); HE4 levels were higher in the OC + E group compared with the OE group (p < .05) (Table 4).
Patients with elevated levels of tumor biomarkers (CA125 and HE4) in the three study groups.
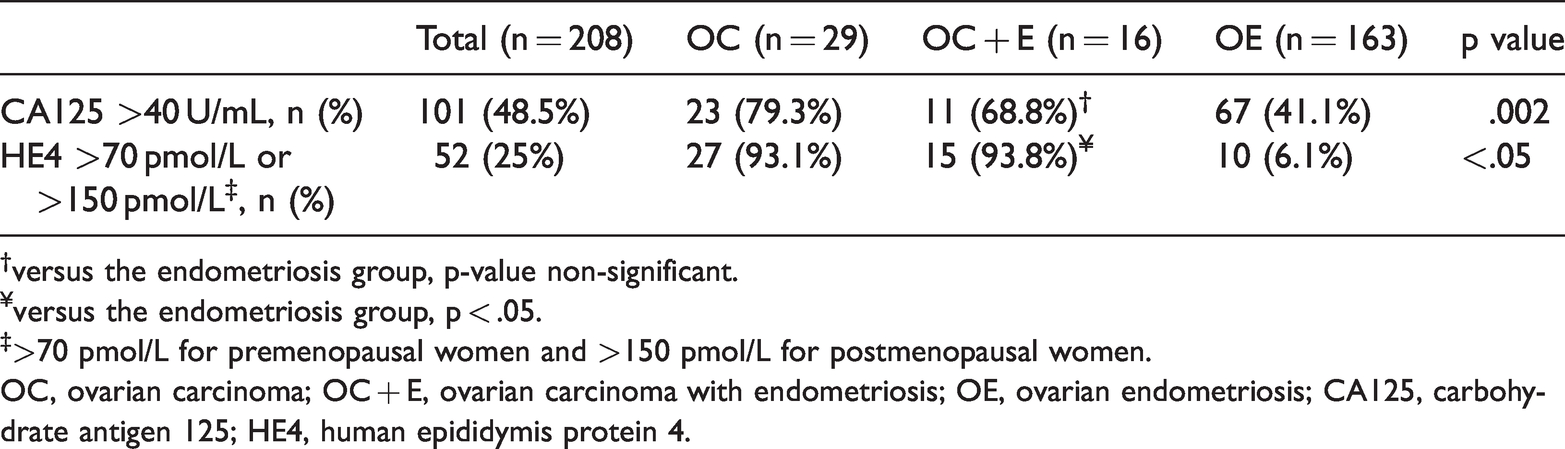
†versus the endometriosis group, p-value non-significant.
¥versus the endometriosis group, p < .05.
‡>70 pmol/L for premenopausal women and >150 pmol/L for postmenopausal women.
OC, ovarian carcinoma; OC + E, ovarian carcinoma with endometriosis; OE, ovarian endometriosis; CA125, carbohydrate antigen 125; HE4, human epididymis protein 4.
Finally, we compared the levels of the tumor biomarkers and ROMA risk in patients with undetermined risk of malignancy according to the IOTA simple rules. Significant differences in HE4 levels (p < .05), but not in CA125 levels nor ROMA risk were found between the groups (Table 5). All OC patients showed elevated levels of both biomarkers, whereas 57% and 85.7% of the OC + E patients showed elevated CA125 and HE4 levels, respectively. No increased levels of HE4 were found in the OE patients.
Distribution of women with undetermined risk of malignancy according to the IOTA simple rules, pathological results, laboratory findings, and high-risk ROMA classification.
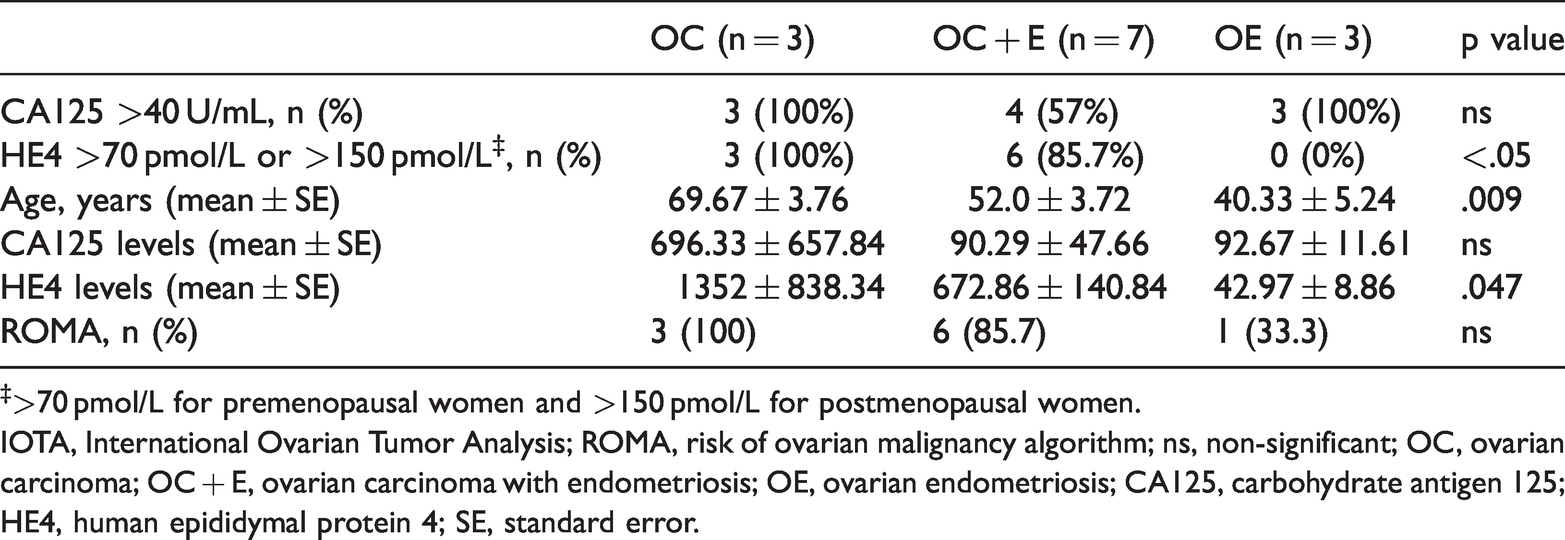
‡>70 pmol/L for premenopausal women and >150 pmol/L for postmenopausal women.
IOTA, International Ovarian Tumor Analysis; ROMA, risk of ovarian malignancy algorithm; ns, non-significant; OC, ovarian carcinoma; OC + E, ovarian carcinoma with endometriosis; OE, ovarian endometriosis; CA125, carbohydrate antigen 125; HE4, human epididymal protein 4; SE, standard error.
Among women with undetermined risk of malignancy by ultrasonography, OC and OC + E patients were significantly older than OE patients; however, differences in HE4 levels were not related to older age (Table 5). Women with suspected malignancy showing undetermined risk of malignancy with ultrasonography and who had OC + E were 52 years old, on average, and the average age in women with OC was 70 years. Although women with endometriosis with undetermined risk of malignancy with ultrasonography were older than the endometriosis patients (40 years), patients with undetermined risk were significantly younger than patients with OC age (p = .009).
Discussion
This study shows that HE4 is a key tumor biomarker in patients with OE and suspected malignancy showing undetermined risk of malignancy with ultrasonography, according to the IOTA simple rules. In this group of patients, low HE4 levels suggest a low risk of malignancy, and, therefore, a more conservative approach can be considered. Discriminating a benign adnexal mass from a malignant one is of utmost importance, not only to choose the best treatment, but also regarding prognosis and to reduce anxiety levels in women with non-malignant conditions.
The IOTA group has published simple and clinically useful rules for discriminating between benign and malignant adnexal masses, which allow classifying adnexal masses as low, high, or undetermined risk of malignancy, with high sensitivity and specificity. 6 In our study, seven patients in the OC + E group, three patients in the OC group, and three patients in the OE group were classified as undetermined risk of malignancy, indicating that further evaluations were required. Most of these patients had elevated levels of CA125, independent of the final pathological report. In contrast, HE4 levels were elevated in the OC and OC + E groups, but levels were normal among OE patients, with a statistically significant difference. ROMA risk did not help classify these patients because only one patient in the OE group had a high risk of malignancy.
CA125 can be elevated in benign conditions, such as endometriosis, and it has even been traditionally proposed as a diagnostic tool for endometriosis patients.16,17 In fact, it is still common among general gynecologists to refer patients with OE and high CA125 levels to oncology units. ROMA is an algorithm that includes HE4 and CA125 levels, and menopausal status. Even though the algorithm and its mathematical equations give higher importance to HE4 than CA125 levels (2.38 × LN [HE4] vs 0.0626 × LN [CA125]), 18 CA125 levels in patients with endometriosis can be elevated and, consequently, these patients have a high risk for malignancy according to ROMA. Considering the results of our preliminary study, the use of CA125 levels and ROMA in patients with OE should be abandoned and replaced with HE4 assessment when malignancy is suspected because HE4 is more specific than CA125 in this group of patients.
Patients with endometriosis have a slightly higher risk of OC,2,4 and 0.5% to 1% of these patients will develop OC (clear cell and endometrioid carcinoma are most frequent); 19 therefore, it is important to discriminate benign and malignant findings. In our study, 35.6% of the patients with malignancy in the final pathological report had endometriosis-associated OC (OC + E). These patients were younger, more frequently premenopausal, and had lower elevated CA125 and HE4 levels compared with patients with OC without endometriosis. These findings are similar to those described by Bas-Esteve et al. 20 The authors compared patients with OC and borderline tumors, and found that OC + E patients were younger, had lower parity, were more frequently premenopausal and, although not significant, had lower CA125 and CA19.9 levels. The authors did not analyze HE4 levels, probably because of the long inclusion period in the study (from 1995 to 2015).
HE4 is a tumor biomarker that is more reliable than CA125, with a specificity of 94%. Its levels are not affected by endometriosis cysts, and it is robust regarding menstrual cycle variations. 21 Kim et al., in a study including 70 patients with OC, also showed that HE4 has a higher sensitivity compared with CA125. 22 Moreover, HE4 is less frequently increased in benign diseases, especially among premenopausal women, 23 and it is more specific than CA125 in premenopausal patients. 24 Consistently, in our study, none of the women with endometriosis and undetermined risk of malignancy showed increased levels of HE4, with a mean age of approximately 40 years.
The incidence of ovarian cancer increases proportionately with age, and invasive epithelial types occur mostly in patients >50 years of age. 25 In our study, the mean age of women with suspected malignancy and undetermined risk of malignancy with ultrasonography and who had OC + E was 52 years compared with the average age in women with OC of 70 years. Women with undetermined risk of malignancy with ultrasonography with endometriosis were older than the endometriosis patients (40 years), but significantly younger than the OC patients.
One of the main strengths of this study is that we compared tumor biomarkers levels in patients with OE, with or without different types, with those with OC + E and those with OC, only, focusing on patients with endometriosis and suspected malignancy and not mixing different benign gynecological diseases. It should be noted that patients with OC included in the study were only the subtypes that most likely coexist with endometriosis; i.e., endometrioid and clear cell cancers. We also took into account ultrasonographic findings, and we analyzed the role of tumor biomarkers in the group with undetermined malignancy risk, where the role of HE4 has been demonstrated as especially relevant.
We are aware of some limitations in our study, and the results must be interpreted accordingly. Although the data were recorded prospectively, the study was retrospective in nature, and results should be interpreted in this context. This study had a limited sample size because only 45 patients with ovarian malignancy were included. These were the patients with endometrioid or clear cell carcinomas who underwent surgery in our center from 2015 to 2019. We decided not to include patients who underwent surgery before 2015 because the ultrasonographic characteristics would have differed. This is because the standardized protocol for the study of ovarian masses in our center was updated at the end of 2014 in accordance with IOTA simple rules after a metanalysis by Nunes et al. was published. 6 Moreover, only 13 patients were classified as undetermined risk after ultrasonography. However, this low number was expected because the IOTA rules were designed to differentiate benign from malignant adnexal masses, and most of the patients included in this study had benign conditions (78%). The scientific community has appropriately accepted that only systematic reviews and meta-analyses combining high-quality evidence from many trials yield robust answers. Individual trials are best viewed as providing important information that contributes to a larger body of evidence. Thus, the number of patients included was small from a biometric point of view, making the study exploratory in nature, only. However, this study is intended to stimulate future multicentric studies to confirm our preliminary results.
In conclusion, in patients with ovarian endometriosis and suspected malignant adnexal masses, HE4 is a more useful tumoral biomarker to diagnose OC when ultrasonography results are inconclusive.