
Abstract
Background
The tumor protein 53 (TP53 or p53) plays an important role in tumor suppression by binding to the regulatory region of its target genes. Single nucleotide polymorphisms (SNP) located in the p53 binding regions are likely to affect the expression of p53 target genes and may contribute to susceptibility to common diseases. The role of the genetic variations in esophageal squamous cell carcinoma (ESCC) has been well explored. However, the role of p53 binding region variations in esophageal cancer is poorly understood.
Methods
We investigated the association of 6 p53 binding region polymorphisms with susceptibility of 400 ESCC cases and 400 cancer-free controls in a Southwest Chinese population using the SNapShot assay. Differences in frequencies of the SPNs genotypes between cases and controls were evaluated using the chi-square test.
Results
We found that the C allele of rs1009316 in Bax and rs762624 in CDKN1A can decrease the risk of ESCC. In the multiple genetic model, we found that the rs2395655 in CDKN1A is related with the risk of ESCC, and that the G allele increases the susceptibility to ESCC (OR: 1.364; 95% CI: 1.104-1.685). We carried out a stratification analysis between alleles and risk of ESCC according to clinical stage. There was no relationship between these SNPs and clinical stage.
Conclusion
SNPs in the p53 binding region may modulate the risk of ESCC in the Southwest Chinese population.
Introduction
Esophageal cancer is the eighth most common malignancy worldwide and its incidence rate is increasing significantly, especially in developing countries (1, 2). Patients with esophageal squamous cell carcinoma (ESCC) have no obvious clinical features and are always diagnosed at moderate or later stages (3). The overall survival of patients with this disease is less than 10%, and the 5-year survival rate is 20%-40% after surgery (1). Therefore, more efforts are needed to find new markers for the early diagnosis of this disease. Esophageal cancer is a complex disease involving genetic and environmental factors, while genetic factors play important roles in ESCC. P53 is the most important tumor suppressor gene, which can prevent cancer onset by maintaining the genomic stability, inducing apoptosis, inhibiting angiogenesis, and by acting in several other ways to regulate many downstream target genes (4–7). P53 as a transcriptional factor can bind to the promoter or intron of its target genes functioning as a cancer suppressor. Additionally, p53 can promote cell apoptosis by upregulating Bax and downregulating Bcl-2 (8–10). Lastly, p53 plays important roles in cycle arrest and genome repair through regulating the expression of the target genes CDKN1A and GADD45A (11, 12).
In this study, we hypothesized that single nucleotide polymorphisms (SNPs) located in the binding regions of p53 may affect its regulatory activity on target genes, thus determining various degrees of tumor susceptibility in carriers of different alleles. Hence, we expected these SNPs in the p53 binding regions to be new markers of risk that can be used for the early diagnosis of ESCC. Our study began with a genome-wide screening of SNPs in the p53 binding regions using data mining. Then, we selected the SNPs found in the Chinese Han population and the tumor-related genes that could be affected by these SNPs. A case-control study design was applied to estimate the relevance of these SNPs for the susceptibility to ESCC in a population of Chongqing Southwest China. At last, we wanted to explore the function of the positive SNPs and provide evidence for their use in the early diagnosis of ESCC.
Methods
Study sample
All subjects were genetically unrelated Han Chinese and were living in Chongqing City in the Southwest China for at least 20 years. The esophageal cancer patients were histopathologically diagnosed and followed at the Southwest Hospital, the first affiliated hospital of the Third Military Medical University. The exclusion criteria were: patients had a previous cancer, metastasized cancer, previous radiotherapy or chemotherapy. The controls were healthy individuals who underwent physical examination in Chongqing, and who had no history of cancer. Each subject participating in this study was scheduled for an interview after written informed consent was given; the interviewers collected the information on demographic data and environmental exposure history using a questionnaire. After the interview, 5 mL of venous blood were collected from each participant.
SNP selection
We began with a genome-wide screening of SNPs in the p53 binding regions in the UCSC (http://genome.ucsc.edu/) and dbSNP (http://www.ncbi.nlm.nih.gov/projects/SNP/) databases. We found 12,301 SNPs located in the p53 binding sites, of which 2,688 are found in the Chinese population according to the HapMap database and were selected as our SNP pool. According to the Gene Ontology database (http://www.geneontology.org/), as well as to previous studies, Bax, CDKN1A, and GADD45A are all genes regulated by p53 and play a critical role in carcinogenesis. Supplementary Figure 1 shows the localization of the genes, the p53 binding regions, and the SNPs. Then, we focused on the SNPs present in the 3 loci and chose SNPs with Minor Allele Frequency (MAF) ≥5% in the Chinese population, based on the HapMap CHB database (Supplementary Tab. I).
Genotyping
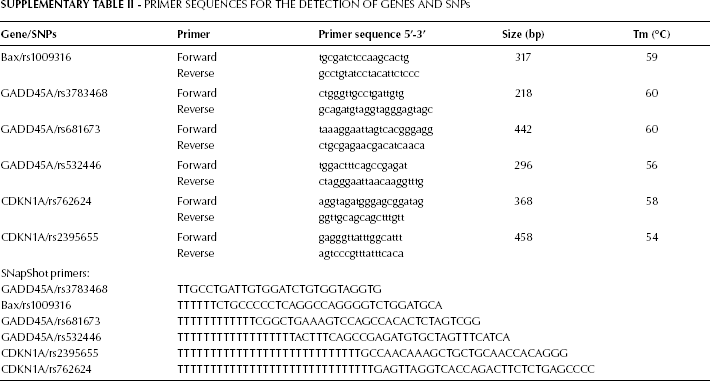
We used the SNaPshot assay to genotype the SNPs. The detailed method can be found in our previous studies (13, 14). PCR and SNaPshot primers are shown in Supplementary Table II. The genotyping results were validated by direct sequencing.
Statistical analysis
The maximum likelihood test for Hardy-Weinberg equilibrium (HWE) was applied to the SNPs among controls (http://ihg.gsf.de/cgi-bin/hw/hwa1.pl). Differences between cases and controls were evaluated by the Student's t test for continuous variables and the x2 test for categorical variables. The associations between SNPs and esophageal cancer risk were estimated by computing the odds ratios (OR) and 95% confidence intervals (CI) using co-dominant, dominant, recessive, multiple, and over-dominant genetic models. All the statistical analyses were performed with the Statistical Package for the Social Sciences software (SPSS 16.0). A p<0.05 indicated a statistically significant difference.
Results
The characteristics of the participants genotyped in this association study are summarized in Table I. Altogether, there were 400 ESCC cases and 400 cancer-free controls in this study. The patients included in our study were recruited from the Department of Cardiothoracic Surgery, at the Southwest Hospital, while healthy controls were recruited from the Physical Examination Center at the same hospital. Cases and controls were part of the Han population living in Chongqing for at least 20 years, did not differ in terms of age (p=0.47) and gender (p=0.22), and were not family-related. The esophageal cancer cases had the following distribution of pathological stages: 7 stage I cases (1.75%), 335 stage IIa (83.75%), 37 stage IIb (9.25%), 13 stage III (3.25%), and 8 stage IV cases (2.0%).
Characteristics of ESCC Patients and Controls

Students' t test;
x2 test; SD: standard deviation.
Table II shows genotype and allele frequency distributions of these SNPs in cases and controls, as well as the results of the HWE test in controls. The HWE has been used to better understand the genetic characteristics of the populations. We used the Hardy-Weinberg test for controlling the genotyping quality. Three SNPs (rs3783468, rs681673, rs532446) showed a deviation from the HWE test, while the other 3 SNPs (rs1009316, rs762624, rs2395655) passed the HWE with p values of 0.340, 0.258, and 0.297, respectively. The SNPs showing departure from the HWE were removed in further analysis.
Genotype and Allele Frequency Distribution of SNPs and HWE Test in Controls

HWE: Hardy-Weiberg equilibrium.
Table III summarizes the association of these polymorphisms with the ESCC risk. Co-dominant, dominant, recessive, multiple, and over-dominant genetic models were used to evaluate the relationship between SNPs and susceptibility to ESCC. We found that the CC genotype and the C allele of rs1009316 and rs762624 could decrease the risk of ESCC in all the models except for the dominant genetic model. By contrast, rs2395655 was related with the risk of ESCC in the co-dominant, dominant, recessive, and multiple genetic models. In the multiple genetic model the statistical significance is the lowest (p=0.004) and, when compared with the A allele, the G allele increases the susceptibility to ESCC (OR: 1.364; 95% CI: 1.104-1.685).
Main Effects of SNPs on ESCC

M: major allele; m: minor allele.
p<0.05 are in bold.
To examine whether the risk associated with the genetic variant was modified by epidemiological factors, we performed logistic regression analyses stratified by gender and age and we found no significant interactions between the genotype and gender, age, or degree of differentiation. To evaluate the interactions between genotype and clinical stage, we carried out an additional analysis evaluating the association between specific alleles and risk of ESCC stratified for the clinical stage. We found no significant interactions between SNPs and ESCC clinical stages (Tab. IV).
Stratification Analyses for SNPs According to Clinical Stage

ref: reference allele.
Discussion
Esophageal cancer is a complex disease that results from both gene-gene and gene-environment interactions. Genetic factors, especially, play important roles in esophageal cancer genesis and may be very important for the early diagnosis of this disease. SNP is the most common variation across the human genome, and is the ideal genetic marker in association studies of complex diseases. Recently, several association studies have been conducted on ESCC, including the genome-wide association study (GWAS) (15–17). In our previous work, we found that a SNP in the pre-miR-196a was associated with susceptibility of ESCC risk in a Chinese Han population and a SNP in the RAP1A 3′UTR could affect miR-196a regulation contributing to the increased ESCC risk (13, 14).
P53 is the most extensively studied gene involved in human cancers including breast cancer, ovarian carcinoma, and head and neck squamous cell carcinoma (SCC) (18–20). P53 can bind to specific DNA sequences, activate its downstream target genes' expression, and thus control cell-cycle arrest, DNA repair, and apoptosis (4). When cells are put in stress conditions, p53 can promote cell apoptosis through the upregulation of Bax and downregulating Bcl-2 (21). Furthermore, the p53-mediated induction of CDKN1A (which encodes WAF1, also known as p21) might also inhibit apoptosis and induce cell-cycle arrest and DNA repair through GADD45A. These effects of p53 might actually protect cells from death during the early stages of tumor progression (22). Thus, the SNPs located in the p53 binding site may affect the regulatory activity of p53 and contribute to cancer susceptibility. A relatively large case-control study showed that SNPs in the promoter regions of BAX and Bcl-2 may affect their regulation by p53, and demonstrated their association with risk of squamous cell carcinoma of the head and neck (23).
The HWE test has been applied for understanding better the genetic characteristics of the populations included. The HWE testing is commonly used for controlling the quality of large-scale genotyping and is one of the few ways to identify systematic genotyping errors in unrelated individuals (24, 25). In our HWE testing, we found that while the p values for rs1009316, rs762624, and rs2395655 were respectively 0.240, 0.258, and 0.297, the 3 SNPs rs3783468, rs681673, and rs532446 did not fit the HWE. Some reasons for this may be: first, the small sample size; second, the 3 SNPs which departed from the HWE are located within the GADD45A gene, which may be under natural selection in this population.
The optimal method for using different genetic models in association studies is not clear when the inheritance pattern of the causal allele is unknown. One apparent solution to this problem is to test several genetic models. Until now, there are only few reports on the association between Bax polymorphisms (rs1009316) and the risk of cancer. The rs1009316 CC genotype decreases the risk of ESCC in co-dominant, recessive, and multiple genetic models. rs1009316 is located in the first intron of Bax and linked with the SNP rs4546878. Some studies found that rs4645878 is associated with squamous cell carcinoma of the head and neck in the Chinese population (23) and is associated with chronic lymphocytic leukemia in a Spanish population (26). Additionally, this SNP was associated with a lower mean Bax expression in the same patients with chronic lymphocytic leukemia (27). Liu Z. and colleagues showed that the SNP rs4546878 of the Bax gene may not be a susceptible genotype for esophageal cancer (28), and this conclusion is different from what shown by our results. This may be explained by the different population and different pathological types considered.
The SNPs rs762624 and rs2395655, located in the promoter region of the CDKN1A gene, are associated with the risk of ESCC. We speculated that these 2 SNPs might affect p53 binding to the promoter of CDKN1A and contribute to the susceptibility of ESCC. Ma H. and colleagues suggested a possible association of the rs2395655 polymorphisms of CDKN1A with the prognosis of NSCLC in a Chinese population (29). Kim K. and colleagues concluded that the minor allele A at rs762624 of CDKN1A is associated with the increased susceptibility to systemic lupus erythematosus and lupus nephritis (30); additionally the decreased cellular levels of p21 and a luciferase reporter gene assay found that the A allele displayed ~15% lower activity than that of the non-risk C allele (30). In our study, the A allele at rs762624 of the CDKN1A gene was associated with an increased susceptibility to ESCC. The underlying mechanism is that the A allele enhanced the regulation of p53 and increased the expression of CDKN1A. Thus, individuals carrying the C allele may have low levels of CDKN1A and be at high risk of ESCC.
In conclusion, we found that 3 SNPs (rs1009316, rs762624, and rs2395655), located in the p53 binding regions, were associated with the risk of ESCC, and provided an experimental evidence for the early diagnosis of ESCC. However, this study has some limitations: first, the sample size and sample range are limited, indicating the need to expand the sample size to further validate this result; second, the biological mechanism by which the SNPs affect the susceptibility to ESCC is unclear. More experiments are needed to clarify the biological functions of the positive SNPs sites, and to provide the theoretical basis of the mechanism for the early diagnosis of ESCC.
Footnotes
Acknowledgements
The authors would like to acknowledge Jun Li and Wei Wu from the department of Thoracic and Cardiac Surgery, of the Southwest Hospital, Third Military Medical University.
Supplementary Material
Primer Sequences for the Detection of Genes and SNPs
| Gene/SNPs | Primer | Primer sequence 5′-3′ | Size (bp) | Tm (°C) |
|---|---|---|---|---|
| Bax/rs1009316 | Forward | tgcgatctccaagcactg | 317 | 59 |
| Reverse | gcctgtatcctacattctccc | |||
| GADD45A/rs3783468 | Forward | ctgggttgcctgattgtg | 218 | 60 |
| Reverse | gcagatgtaggtagggagtagc | |||
| GADD45A/rs681673 | Forward | taaaggaattagtcacgggagg | 442 | 60 |
| Reverse | ctgcgagaacgacatcaaca | |||
| GADD45A/rs532446 | Forward | tggactttcagccgagat | 296 | 56 |
| Reverse | ctagggaattaacaaggtttg | |||
| CDKN1A/rs762624 | Forward | aggtagatgggagcggatag | 368 | 58 |
| Reverse | ggttgcagcagctttgtt | |||
| CDKN1A/rs2395655 | Forward | gagggttatttggcattt | 458 | 54 |
| Reverse | agtcccgtttatttcaca | |||
| SNapShot primers: | ||||
| GADD45A/rs3783468 | TTGCCTGATTGTGGATCTGTGGTAGGTG | |||
| Bax/rs1009316 | TTTTTTCTGCCCCCTCAGGCCAGGGGTCTGGATGCA | |||
| GADD45A/rs681673 | TTTTTTTTTTTTCGGCTGAAAGTCCAGCCACACTCTAGTCGG | |||
| GADD45A/rs532446 | TTTTTTTTTTTTTTTTTTACTTTCAGCCGAGATGTGCTAGTTTCATCA | |||
| CDKN1A/rs2395655 | TTTTTTTTTTTTTTTTTTTTTTTTTTTTGCCAACAAAGCTGCTGCAACCACAGGG | |||
| CDKN1A/rs762624 | TTTTTTTTTTTTTTTTTTTTTTTTTTTTTTGAGTTAGGTCACCAGACTTCTCTGAGCCCC | |||