
Abstract
Introduction
Esophageal cancer was the eighth and sixth leading cause of morbidity of all cancers in the world, and the 15th and 12th in Ethiopia, respectively. There is a lack of comprehensive data regarding Ethiopia’s esophageal cancer hotspot, treatment outcome clustering, and other factors.
Objective
This scoping review was designed to understand the extent and type of existing evidence regarding spatiotemporal distribution, time to treatment outcome clustering, and determinants of esophageal cancer in Ethiopia up to March 28, 2023.
Methods
Three-step search strategies were employed for the scoping review from March 15 to 28, 2023. Targeted databases included PubMed/Medline, PubMed Central (PMC), Google Scholar, Hinari, and Cochrane for published studies and different websites for unpublished studies for evidence synthesis. Data were extracted using the Joanna Briggs Institute (JBI) manual format.
Results
Our final analysis comprised 17 (16 quantitative and 1 qualitative) studies. Three studies attempted to depict the country’s temporal distribution, whereas 12 studies showed the spatial distribution of esophageal cancer by proportion. The regional state of Oromia recorded a high percentage of cases. Numerous risk factors linked to the tumor have been identified in 8 investigations. Similarly, 5 studies went into detail regarding the likelihood of survival and the factors that contribute to malignancy, while 2 studies covered the results of disease-related treatments.
Conclusions
The substantial body of data that underpins this finding supports the fact that esophageal cancer has several risk factors and that its prevalence varies greatly across the country and among regions. Surgery, radiotherapy, or chemotherapy helped the patient live longer. However, no research has investigated which treatment is best for boosting patient survival and survival clustering. Therefore, research with robust models for regional distribution, clustering of time to treatment outcomes, and drivers of esophageal cancer will be needed.
Plain language summary
The review was based on 17 studies searched from five electronic databases, and six additional sources. Esophageal cancer incidence varies across the nation (from region to region). The median survival time of esophageal cancer cases were four months, and six months. No study investigated the better treatment that improved the survival of patients with esophageal cancer. A contradicting report were found about the link b/n khat chewing and esophageal cancer. The temporal distribution of the tumor was controversial.
Keywords
Introduction
Cancer is a group of disorders defined by the uncontrolled growth and spread of abnormal cells, 1 whereas esophageal cancer is a tumor [squamous cell carcinoma (SCC) and adenocarcinoma (AC)) that develops in the tissue lining the esophagus.2,3 Nonspecific signs of esophageal cancer include heartburn, unusual chest discomfort, dyspepsia, occult blood in the stool, and iron deficiency anemia; as the illness progresses, dysphagia, weight loss, and anorexia develop. 4 Incessant cough and pneumonia can result from tracheoesophageal or bronchoesophageal fistula.4,5
Cancer can be fatal if it spreads uncontrollably. 1 The global cancer burden increased to 19.3 million new cases and 10 million new deaths in 2020 6 from 18.1 million new cases and 9.6 million new deaths7-9 in 2018. In 2013, the number of new cases was 14.9 million and 8.2 million new deaths,10,11 and it was estimated to double by 2040. 8 Esophageal cancer is the eighth 12 and sixth leading cause of morbidity8,12,13 and mortality4,5,8,14 of cancer in the world, and the 15th and 12th in Ethiopia,12,15 respectively. The standardized incidence rate of esophageal cancer ranges from 4.5 per 100,000 in Sub-Saharan countries to 11 per 100,000 in East Asia. 16 Esophageal cancer is highly prevalent in central Asia, known as the esophageal cancer belt, and Eastern Africa’s esophageal cancer corridor. 17
Although the underlying causes of cancer are not fully understood, various factors have been identified as contributing to the disease’s occurrence, either concurrently or sequentially, 1 including many that were modifiable (eg, tobacco use and excess body weight) and those that were not (eg, inherited genetic mutations and immune conditions). 4 Many studies pinpointed environmental; living (polymorphisms and Polycyclic aromatic hydrocarbons (PAH) (from wood, 18 and tobacco)8,16,19,20), and working (chemical fumes)8,21; Nutritional; low vegetable and fruit consumption which results in low vitamins and minerals,2,4,16,19,21 consumption of red meat (N-nitroso compound),19,21 bulimia, 22 supplements (selenium supplementation), 23 zinc deficiency, 16 and hot drinks,19,20,23 behavioral; alcohol,2,18-21,24 tobacco,2,4,18-23 khat 25 and obesity,2,18,19,21,26 previous medical history; gastroesophageal reflux disease,2,18,19,21-23 barrett’s esophagus,2,4,18,19,21,22 achalasia,2,21 caustic stricture,19,23 gastrectomy and atrophic gastritis, tylosis,2,21 viral agents,20,23 and H. pylori,18,27 oral and teeth infection, 19 drugs; proton pump inhibitors (PPI’s), statins, histamine receptor antagonists (H2RAs), regular aspirin use, and nonsteroidal anti-inflammatory drugs (NSAIDs),16,18 genetics,19,23,28 and sociodemographic factors; age,21,23 gender,18,21,23,28 and race, 18 and other factors like sex hormones, 28 and health seeking behavior 29 were associated to esophageal cancer.
A few reviews on the management of esophageal cancer revealed that using chemotherapy preoperatively and/or postoperatively or neoadjuvantly has no significant effect on the survival of the patient compared with surgery alone.4,5,30 The same result was reported for preoperative chemotherapy and radiotherapy. 4 The survival of Esophageal cancer patients was significantly linked to clinical classification (ie, stages, histologic types, and cancer site). 31
Different studies have revealed that esophageal cancer distributions vary based on geographical locations.16,18,29,32-37 Adenocarcinoma (AC) is common in developed countries, whereas squamous cell carcinoma (SCC) is more common in developing countries.16,32 A study conducted in Canada showed spatial clustering of esophageal cancer. 38
Studies have shown that Ethiopia (Arsi/Bale regions), Western Kenya (Eldoret, Tenwek), Malawi, Mozambique, Zibabwe and Northern Tanzania (Kilimanjaro) form part of East Africa’s high-risk corridor for esophageal squamous cell carcinoma (ESCC).17,39,40
Despite an increase in esophageal cancer cases in Ethiopia, the country has few resources for management, research, and early detection, diagnosis, and screening. The causes of sudden rises in occurrences should be the focus of research, rather than studies emphasizing early diagnosis to improve the prognosis of the disease,8,41 particularly in developing nations like Ethiopia. The researchers recommended a thorough examination to identify regional risk factors for esophageal cancer prevention and control.29,33
A preliminary search of PubMed (Medline), PubMed Central (PMC), Google scholar, Hinari, and Cochrane databases as well as Google and MedNar (https://mednar.com/mednar) were conducted from September 15 to 20, 2022, and we could not find systematic reviews or scoping reviews on the topic. Thus, these scoping reviews, also called mapping reviews or scoping studies, 42 were designed to identify and understand the extent and type of evidence existing about spatiotemporal distribution, time to treatment outcome clustering, and determinants of esophageal cancer in Ethiopia up to March 28, 2023.
Review Question
Primary question
What is known from the existing literature regarding spatiotemporal distribution, time to treatment outcome clustering, and their determinants among Ethiopian patients with esophageal cancer?
Sub-questions
➢ What is the esophageal cancer hotspots and times in Ethiopia? ➢ What are the Determinants of the Spatiotemporal Clustering of Esophageal Cancer in Ethiopia? ➢ What are the Determinants of Esophageal Cancer outcomes in Ethiopia? ➢ What are the determinants of Time to Treatment Outcome clustering among Esophageal Cancer patients in Ethiopia?
Methods
Protocol and Registration
The scoping review was conducted in accordance with the Joanna Briggs Institute (JBI) guideline and methodology for scoping reviews. 43 In addition, the JBI scoping review framework was used for the development of this review protocol. 42 The Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) reporting standard was used for the scoping review final report writing (Appendix I_Tricco_2018. docx). 44 The scoping review protocol was registered with Open Science Framework (https://osf.io/) (ie, registration number osf. io/qf8w6) and Figshare (https://figshare.com/) (ie, Doi of the item 10.6084/m9. figshare.21228065).
Eligibility Criteria
Participants
All full text and English language studies conducted on esophageal cancer, both squamous cell carcinoma and adenocarcinoma, in patients in Ethiopia were targeted for the scoping study.
Concept
All research conducted on esophageal cancer’s distribution/clusters in prevalence, survival rate, time to treatment outcome clustering, and their determinants in Ethiopia were considered for the scoping review. Esophageal cancer includes both squamous cell carcinoma (SCC) and adenocarcinoma (AC).1,2
Context
The scoping review included all research conducted in Ethiopia. The capital city of Ethiopia is Addis Ababa. Ethiopia is found at the horn of Africa; and bounded by Sudan and South Sudan to the west, Kenya to the south, Somalia to the East, Djibouti to the northeast, and Eritrea to the north. The country is located at 9.1450 N (ie, between 3 and 15° north latitude, between the Equator and the Tropic of Cancer) and 40.4897 E (ie, between 33 and 48° east longitude) latitude and longitude, respectively. 45 Approximately 44% of Ethiopians are under the age of 15 years, while 4% are 65 years and older with 1 to 1 sex ratio. 46
Search Strategy
Sample Search Strategies Aligned With the PCC Mnemonic Elements of the Review Question, Inclusion Criteria, and Exclusion Criteria for 2023.

Source of Evidence Selection
Following the search, all identified citations through the 3 steps were collated and uploaded into the EndNote X7.2.1(Bid 8311) software, and duplicates were removed. Following a pilot test, titles and abstracts were then screened by 2 independent reviewers for assessment against the inclusion criteria for the scoping review. Potentially relevant sources were retrieved in full and their citation details imported into the EndNote X7.2.1(Bid 8311) software.
47
The full texts of the selected citations were assessed in detail against the inclusion criteria by 2 independent reviewers (TK and AM). Reasons for exclusion of sources of evidence in full text that did not meet the inclusion criteria were recorded and reported in the scoping review. Any disagreements that might arise between the reviewers at each stage of the selection process were resolved through discussion. The results of the search and the study inclusion process were reported in full in the final scoping review and presented in a Preferred Reporting Items for Systematic Reviews and Meta-analyses extension for scoping review (PRISMA-ScR) flow diagram (Figure 1).44,48
Data Extraction
Data were extracted from papers included in the scoping review by 2 independent reviewers (ie, TK and AM) using a data extraction tool adapted from the Joanna Briggs Institute (JBI) manual format and guideline for the scoping review. The extracted data included specific details about the participants, concept, context, study methods (ie, study design, sampling process, and sample size), and key findings relevant to the scoping review questions. The 2 reviewers piloted, after adaption, the draft of the data extraction form on 3 articles selected independently before the actual review. Based on the pilot results, the draft data extraction tool was modified and revised. The disagreements that might have been raised between the reviewers were resolved through discussion.
Data Analysis and Presentation
The scoping review extracted the results from the included sources and mapped the evidence. The data extractions were conducted by the 2 reviewers using the format prepared by the reviewers independently, and then it was imported into STATA 14 statistical software for further analysis. For quantitative paper, summary measures were computed using STATA 14 version after double data entry was independently performed by the 2 reviewers. The summary measures were pooled prevalence (rate) (for categorical data), proportion range, and mean range (for continuous data). The summarized values and ranges were further interpreted and discussed in detail to identify the gaps in the study area. Where statistical pooling was not possible, in the case of qualitative analysis, the findings were presented in narrative form, including tables and figures, to aid in data presentation. The qualitative content analysis approach was applied to analyze the participants, concepts, and contexts of the studies included in the scoping review. Charting of data was used to identify, characterize, and summarize research evidence on a topic, including the identification of research gaps (Table 3). The results of a scoping review were presented as a map of the data extracted from the included papers in a diagrammatic (Figure 1) or tabular form and/or in a descriptive format that aligns with the objective/s and scope of the review. The elements of the PCC mnemonic inclusion criteria were followed to guide how the data should be mapped most appropriately.
Results
Selection of Sources of Evidence
From a total of 1088 documents obtained by searches in the five electronic databases, 889 titles and abstracts were reviewed after deleting duplicates (ie, PubMed/PMC = 674, PubMed/Medline = 25, Cochrane = 11, Hinari = 427, and Google scholar = 54) and from 6 others additional sources (OpenGrey = 1, google = 158, HUIR = 1, AAUIR = 8, UoGIR = 9, Mednar = 15). Eight hundred sixty-three (863) publications were excluded from eligibility after being examined by title and abstract and found to not have been done in Ethiopia, have not dealt with Esophageal cancer, survival, or their determinants, or could not be obtained in full for the 3 remaining articles. Consequently, only 23 full-text and English-language studies that were further reviewed for eligibility were undertaken on esophageal cancer in Ethiopia. Out of 23 full-text studies, 2 were published twice; 3 did not mention spatial/temporal or survival clustering or their factors; and 1 study examined all cancer patients without mentioning esophageal cancer separately. Eventually, throughout our data extraction and narrative account stages, our scoping review contained 17 applicable papers (Figure 1).
Characteristics of the Included Studies
Two studies were published in 1990 (49) and 1994 (50), before 33 years and 29 years, respectively. The majority of the studies (64.70%) were published within the last 7 years (ie, 2016-2022).51-61 Four works, 2 of which were preprints62,63 and 2 of which were Addis Ababa University theses,64,65 have not yet been published. Only 5 of the studies (29.41%) obtained primary data,53,58,59,62,65 whereas most studies (58.82%) relied on secondary data.49-52,54-57,61,64 Of the investigations, 2 (11.76%) gathered both secondary and primary data.60,63 Six of the studies were case-control studies, of which half were matched case control studies,49,53,58 and the other half were unmatched case control studies51,54,60; 3 studies were cross-sectional57,64,65; 2 studies were cohort studies, 1 of which was prospective, 59 the other retrospective 55 ; 1 study was qualitative phenomenology 62 ; and for 4 studies, a clear study design was not reported.50,52,56,61 The studies were carried out in Addis Ababa City (ie, on patients from Tikur Anbessa Specialized Hospital (TASH),52-55,59,63-65 Mexico Higher Clinic (MHC),53,54 the Adera Higher Clinic (AHC),51,53,54 6 health facilities from Addis Ababa, 60 and Addis Ababa Cancer Registry (AACR) (three governmental hospitals and 12 private facilities submitted cancer cases) 61 ) (64.71%),51-55,59-61,63-65 Yirga Alem (on patients from Sidama Regional Hospital) (5.88%), 50 Arsi zone (patients from Asella Teaching and Referral Hospital and others) (23.53%),49,57,58,62 and 10 referral hospitals from 7 regions and one administrative town (Amhara (Gondar University RH), Oromia (on patients from Aira general Hospital, Goba referral, and Arsi University referral and teaching hospitals), SNNPR (Hawassa University RH), Tigray (Ayder RH), Afar (Dubti RH), Harari (Hiwot Fana Specialized hospital), Somali (Karamara RH), and Dire Dawa (Dilchora RH) (5.88%). 56 No studies were undertaken in the community because all investigations49-65 were conducted at health institutions.
Characteristics of Patients Included in the Studies
Regions’ Esophageal Cancer Proportion Ranges Reported by Studies in 2023.

Spatiotemporal Distribution
Although there was no study that tested the spatiotemporal distribution of esophageal cancer via a strong model, some studies attempted to depict the spatial distribution by proportion across the regions,50-56,64,65 and zones,50,52,57,58,62,65 and only 3 studies attempted to depict the temporal distribution using time at first diagnosis.56,61,64 Accordingly, a high proportion of cases were reported from the Oromia regional state (37.82%) followed by the Somali regional state (9.09%). The smallest proportion of EC was observed from the Gambella reginal state (.04%), whereas for 2.35% of cases, the origin of region or zone was not reported (Figure 2). proportion of esophageal cancer cases reported by studies for regions of Ethiopia in 2023.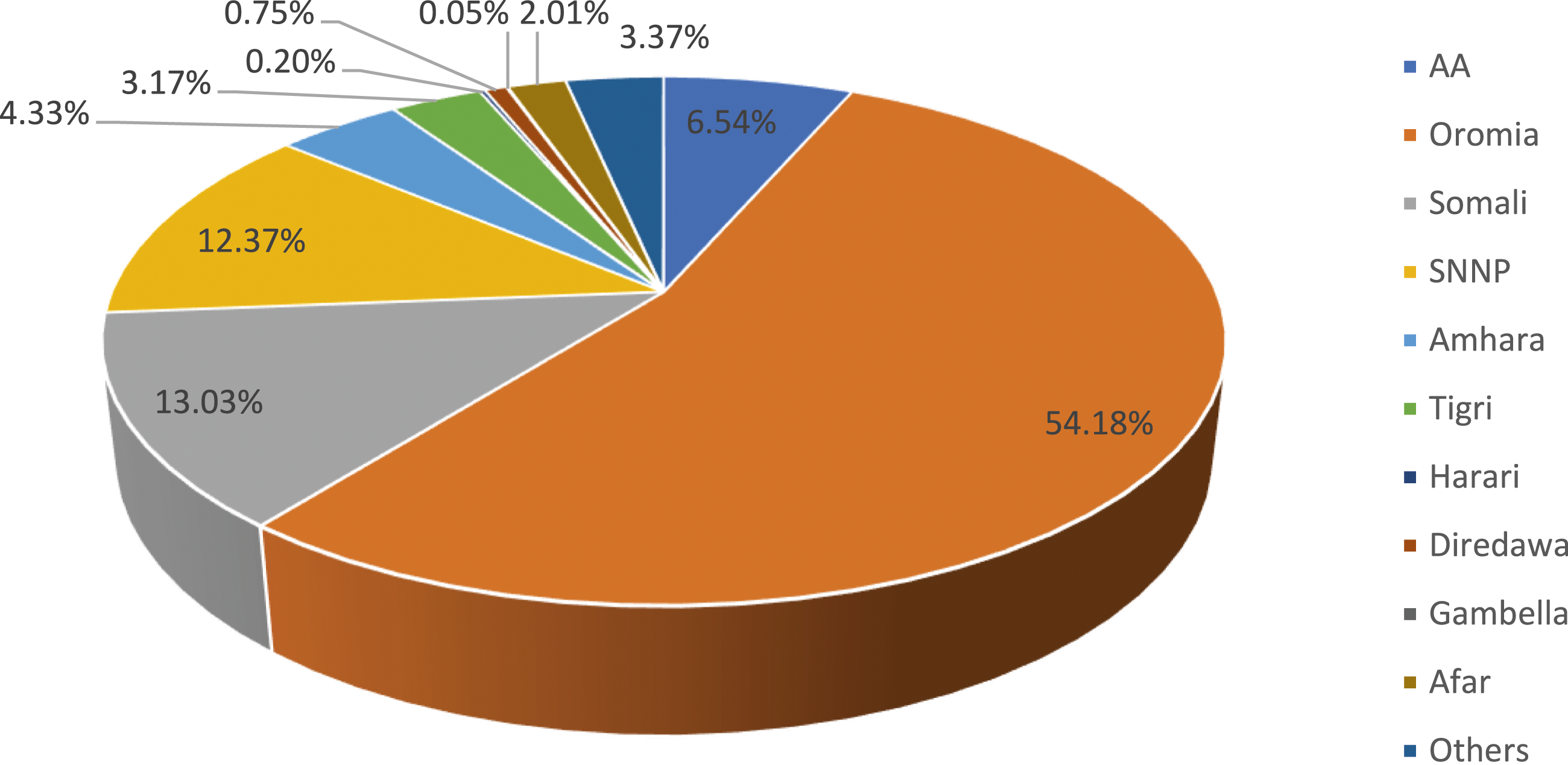
Source of Evidence Details, Characteristics, and Results Extraction Instrument Adapted From JBI Guideline 2023.
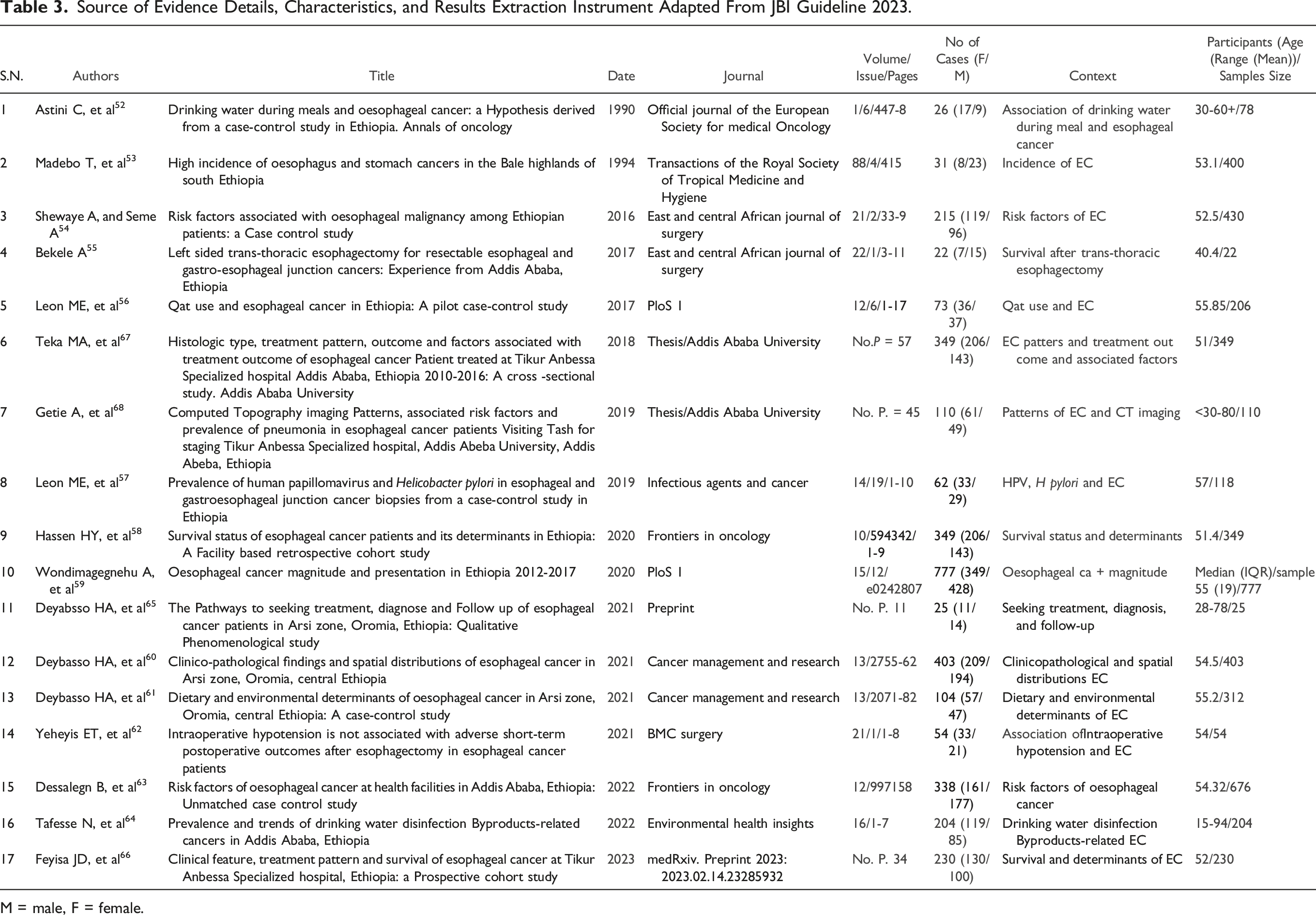
M = male, F = female.
Five studies reported distribution of esophageal cancer cases at town or zones level, of which 19.98% of the cases were from Ars zone,50,52,57,58,62,65 1.26% of the cases were from Bale zone,50,52,65 .25% of the cases were reported from Gurage Zone,52,65 and 1.3% of the cases were from other zones (ie, Siltie, 4 North Shewa, 3 Gojam, 3 Gondar, 1 Adama, 4 Shashemene, 4 Welkite, 2 Hararge, 2 Segen, 1 Welega, 6 Kembata, 2 Jijiga, 1 Hawassa 4 ). A study from the Arsi zone attempted to identify clusters of Esophageal cancer at the district level using the number of cases as measurements. Thus, Jeju, Diesis, and Robe world were reported as hotspots area of the EC with 31 and more cases; Ziway Dugda, Shirk, Sude, Lude Hitosa, and Dodota were reported with 21-20 EC cases; Merti, Cole, Amigna, Bele Gesgar, Limu Bilbilo, Munesa, and Tiyo were areas with 11-20 EC cases. Asko, Guna, Gololcha Arsi, Serum, Inkolo Wabe, Degelia Tico, Tena, Hitosa, and Bele Gesgar were where the list EC cases were reported (1-10 cases). Additionally, the study pinpointed that cases were clustered to highland, 178 (44.2%), midland, 137 (34.0%), and lowland, 88 (21.8%) agroclimatic divisions. 57
Only 3 studies have reported the temporal distribution of esophageal cancer, where the study conducted by Teka MA et al (2018) reported irregularity of the number/proportion of patients diagnosed with esophageal cancer from 2012 to 2016, with the highest proportion seen in 2011 (23.1%) followed by 2016 (12.89%). 64 However, a study conducted at 10 hospitals from 7 regions by Wondimagegneh et al in 2020 revealed an increase in esophageal cancer cases from 2012 to 2017 (56). On the other hand, another study by Tafess N et al, 2022 reported that esophageal cancer cases significantly decreased from 2012 (baseline year) to 2016 in Addis Ababa. 61
Survival Clustering/Survival
Survival of the patients was considered from the time of diagnosis to the occurrence of death. Five studies reported the outcome of patients from a total sample size of 1728. Approximately 18% of the patients were alive; 47.28% of the patients passed away; and for 34.72% of the patients, the outcome status was unknown at the time of analysis.52,55,56,63,64 Three of the articles measured the survival of esophageal cancer patients even though the survival was not consistent over time.55,56,63 Two studies reported that the median survival time of esophageal cancer cases were 4 months 55 and 6 months. 63 For the 2 studies, the median follow-up time was 32 (IQR = 27) months, 55 and 35 (IQR = 27) months 63 with 1932, and 1244 person-month follow-up periods, respectively. This yielded an overall 3176 person-month follow-up period. Within this follow-up period, 56 esophageal cancer cases were alive, resulting in an overall survival rate of 17.63 per 1000 person-months.55,63 The 3 studies elaborated the survival of esophageal cancer patients over the follow-up period. Accordingly, the study conducted by Hassen HY et al, 2020, reported that the survival rates of patients at 1, 2, and 3 years were 14.4% [95%CI: 11.0-18.9], 6.3% [3.9%–10.2], and 2.4% [.9%–6.0%] respectively. 55 Nearly the same result was reported by Feyisa JD et al, 2023, who reported that the survival rates of esophageal cancer cases at 6 months, 1 year, and 2 years were 54.6% (95%CI:47.5%-61.2%), 19.5% (13.8% −25.9%), and 2.0% (.45%–5.9%), respectively, whereas the status of 43 (18.7%) patients was unknown. The study revealed that only 17 (7.4%) patients were alive at the time of analysis. 63 The other study conducted by Wondimagegnehu A et al, 2020 revealed that the 6-year survival rate was 194 (25%) while 26 (3.3%) patients passed away. However, for 557 (71.7%) cases, the survival status was unknown. 56
Treatment Modalities and Treatment Outcomes
Six of the articles reviewed documented diverse treatments administered to esophageal cancer patients. For 60.29% of the total patients (n = 1458) the treatment administered were recorded. Accordingly, the treatments being administered in the country were chemotherapy, surgery, and radiotherapy, either concurrently or separately49,52,55,56,59,63 (Figure 3). The types of surgery performed were resection without macroscopic residual tumor,
52
esophagectomy,
49
trans-hiatal esophagectomy (THE),55,56,59,63 Ivor-lewis/Trans thoracic esophagectomy (TTE),55,56,59,63 Feeding gastrostomy,
55
thoracotomy/laparotomy,55,56 and feeding tube.56,63 Chemotherapy was prescribed for the patients for Neoadjuvant,55,63 adjuvant,55,63 and palliative purpose.55,63 The 2 studies added that radiotherapy was also used as Neoadjuvant,55,63 radical,55,63 and palliative
23
. Two studies mentioned the various types of chemotherapy used for the treatment of esophageal tumor like Cisplatin + 5 fluorouracil (5-FU),56,63 Cisplatin + paclitaxel,56,63 carboplatin + paclitaxel,
56
and Cisplatin + irinotecan
56
whereas Cisplatin + 5 fluorouracil (5-FU) was prescribed frequently followed by Cisplatin + paclitaxel. The study conducted by Yeheyis ET et al, 2021 recommended trans-Hiatal esophagectomy for mid- and distal thoracic esophageal cancers; McKeown’s esophagectomy for mid- and upper thoracic esophageal cancers.
59
Two studies reported that radiotherapy and chemotherapy were used concurrently for the treatment of the tumor.55,63 Even though a study conducted by Bekele
52
(2017) commented that surgery was the mainstay of treatment for esophageal cancer, there was no study recommendation for the “gold standard” treatment. Regarding the country’s esophageal cancer treatment outcomes, only 1 study was published.
64

Histological Sub-type
Twelve (70.59%) studies investigated the histologic sub-type of esophageal cancer.50-57,62-65 The total number of esophageal cancer cases reported by these studies was 2646. Of these, more than half of the patients (55.86%) were diagnosed with squamous cell carcinoma, and for 27.55% of the patients, the histological subtype was not known (Figure 4). The studies reported that the range of squamous cell carcinoma was between 8.62% and 98.26%,50-57,62,64,65 adenocarcinoma was between 1.74% and 22.73%,50-57,62,64,65 Adenosquamous (mixed) carcinoma was between .29% and 19.18%,53,54,56,63-65 and the proportion of patients whose information did not register was between .91% and 84.81%.50-57,62,64,65 Proportion of esophageal cancer by histological subtype in the country, 2023.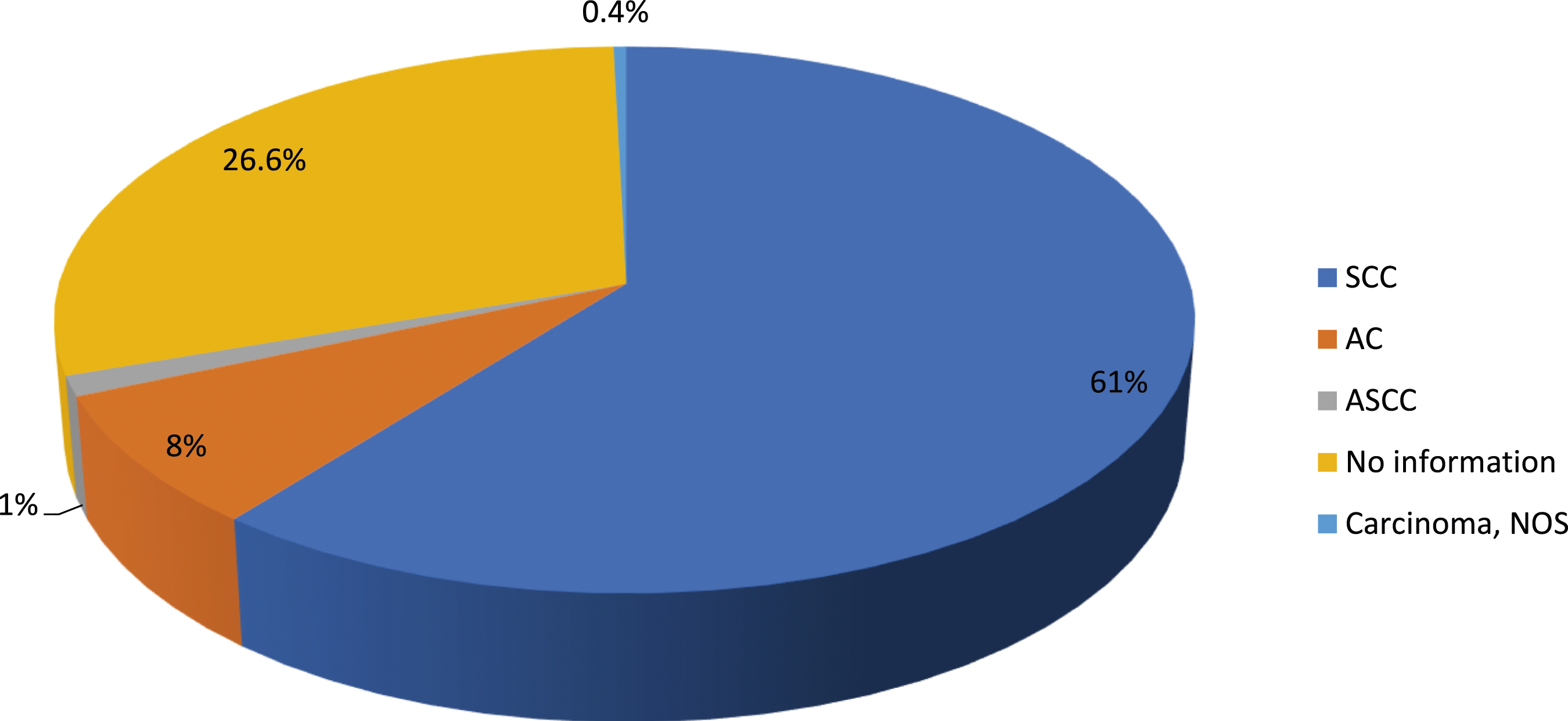
Determinants of Survival
Five studies identified different types of factors associated with survival in patients with esophageal cancer.55,59,62-64 One of the factors reported by the 4 articles was the treatment status of the patient, where the survival improved significantly for those who treated by chemotherapy,55,59,63,64 surgery,55,64 and radiotherapy 55 compared with those who were not treated. However, no study has investigated better treatments that improve the survival of patients with esophageal cancer. Anastomotic leak, MI, Stroke, and chylothorax (sepsis, hypotension) were also reported in 1 study. 59 Esophageal cancer patients found with poor performance status at presentation, local recurrence, and brain metastases were less likely to survive, as reported by Feyisa JD et al, 2023 (63). Two studies identified that the survival time varied among pathological and clinical stages, where patients with advanced stage (ie, stage III and IV) survived less than those with stage I and II. A qualitative study conducted by Deyabsso et al 62 in 2021 explored that experiences of survival with EC were linked to patients’ food intake, treatment side effects, quality of life, and psychological and physical impairments.
Determinants of Esophageal Cancer
Eight articles identified 1 or more risk factors for esophageal cancer.49-51,53,54,58,60,61 One study reported that drinking water during meals had a protective effect on the disease. 49 The other 2 studies identified eating hot food (like hot porridge) as a risk factor for developing esophageal tumors.49,58 On the other hand, 2 studies reported that porridge consumers without considering temperature were at the highest risk of developing EC compared to those who had a habit of consuming other food like Injera.51,58 The study conducted by Shewaye and Seme 51 (2016) reported that residing in the Oromia, Amhara, and SNNP regions was significantly associated with the disease in the country compared with residing in the Addis Ababa city. In addition, the study identified that farmer workers were at a high risk of developing esophageal cancer compared with the unemployed. Two studies revealed that being in the age category of 35 years and more was significantly associated with esophageal cancer compared with those aged less than 35 years.51,60 Those who attended any schooling (ie, educational status) were at a lower risk of developing the tumor.53,54 These 2 studies added that Christian religion followers were at less risk to have the tumor compared with other religion followers.53,54 Consuming fruit and vegetables daily was stated as protective for tumor of the esophagus by Leon ME et al, 2017 and Dessalegn B et al, 2022. 60 Nevertheless, the study conducted by Leon ME et al, 2017 discovered that eating a salty diet was reported as a risk for the development of tumor of the esophagus. 53 Tobacco users (ie, any use) were at a high risk of developing esophageal malignancy, as identified by Leon ME et al, 2019, and Dessalegn B et al, 2022. 60 This result contradicted a study by Leon ME, et al 2017, which reported that tobacco use had no association with esophageal cancer. 53 A study conducted by Deybasso et al 58 , 2021, stated that drinking scalding coffee, drinking large volumes of coffee, eating porridge fast, low intake of dairy products, cooking food in sleeping room, exposure to X-ray, nonalcohol homemade drinks (kenneth), and use of chemical containers were risk factors associated with the development of malignancy . Residing in a rural area, khat chewing, raw meat consumption (red meat), monthly income less than 35USD, consuming tobacco and alcohol together, consuming tobacco and khat together, consuming alcohol and khat, consuming tobacco, alcohol, and Khat together, consuming 2 and more cups of spice tea per day, consuming 2 and more cups of tea per day; experiencing mouth or tongue burn; and consuming sorghum as a staple diet 60 were reported as risk factors for EC by Dessalegn B, et al, 2022. 60 However, the 2 studies conducted by Made et al (1994) and Leon et al (2017) discovered that khat chewing and alcohol drinking had no significant association with EC.53,54 A study conducted in Addis Ababa by Tafesse N, et al, 2022 disproved that disinfection byproduct (chlorine byproduct) had no association with tumors of the esophagus. 61 Although the association was not well-investigated HPV and H. Pylori were the 2 infections detected in the tumor of the esophagus. 54
Discussion
In this scoping review, findings from 17 papers that discussed spatiotemporal distribution/clustering, time to treatment outcome clustering, and/or the determinants of esophageal tumors were identified, selected, and synthesized using conventional systematic review procedures. We were able to document the current state of peer-reviewed, preprint, and theses literature on esophageal cancer by examining regional distributions, time to treatment outcome clusters, and their determinants in Ethiopia. For the benefit of Ethiopian and international esophageal cancer practitioners, researchers, and policy makers, we have included vital information below on the consequences of the findings and the gaps that this review’s findings revealed.
Drinking water during meals, 49 eating hot food (like hot porridge),49,58 residence,51,60 occupational status, 51 age,51,60 educational status (schooling),53,54 religion,53,54 fruit and vegetables consumption,53,60 eating a salty diet, 53 tobacco use (ie, any use,54,60 drinking hot beverages, drinking large volumes of coffee, speed of eating porridge, low intake of dairy products, cooking food in sleeping room, exposure to X-ray, nonalcohol homemade drinks (kenneth), use of chemical containers, 58 khat chewing, raw meat consumption (red meat), monthly income, consuming tobacco and alcohol, consuming tobacco and khat, consuming alcohol and khat, consuming tobacco, alcohol, and Khat together, consuming spice tea, consuming tea frequently, experiencing mouth or tongue burn; and consuming sorghum as staple diet, 60 HPV and H. Pylori infections 54 were the factors associated with esophageal cancer. Detected in the tumor of the esophagus. 54 Treatment status,55,59,63,64 anastomotic leak, MI, stroke, chylothorax (sepsis, hypotension), 59 and pathological and clinical stage59,63 were factors associated with survival of patients with esophageal cancer.
The outcomes of the studies that were included provided some significant data regarding the spatiotemporal, time to occurrence of outcome, time to treatment outcome clustering, and their determinants among esophageal cancer patients. Even if the research did not support the proper approach to determine the spatial clustering of the disease, the distribution of esophageal cancer varied from region to region in the country. Few studies have also attempted to demonstrate the temporal clustering of the disease using the period since the initial diagnosis. The proper test for temporal clustering, however, was not applied because it used the count or percentage of patients with a diagnosis. No study investigated time to treatment outcome or time to treatment outcome clustering except 3 studies that showed time from first diagnosis to occurrence of outcomes.55,56,63 Only 1 study reported the treatment outcomes of various treatments for esophageal cancer patients. 64
The majority of the studies49,51,53,54,57,58,60,64,65 used case-control and cross-sectional designs that relied on secondary data, and a sizeable number of studies50,52,56,61 did not clearly state their study designs. Except for a few, all investigations were conducted in health institutions located in the nation’s capital (Addis Ababa).
Twelve studies were found in the scoping review to have attempted to illustrate the geographic distribution of esophageal cancer cases by proportion across regions50-56,64,65 and/or zones,50,52,57,58,62,65 whereas only 2 studies attempted to do so by examining the timing of initial diagnoses.61,64 Although the actual exposure may have occurred at the kebele level, which is the lowest structural unit in the country, most studies have documented the distribution of cases at the regional level. As a result, the number of cases varied by area within the nation; the highest number of cases was recorded from the regional state of Oromia (37.82%), followed by the regional state of Somalia (9.09%). The region with the lowest percentage of EC cases was Gambella (.04%), whereas in 2.35% of cases, the origin of the region or zone was not noted. Additionally, the Shewaye and Seme 51 study (2016) found that living in the Oromia, Amhara, and SNNP regions of Ethiopia was substantially related to the condition compared with living in Addis Ababa city. This may indicate that important risk factors in 1 community have a more limited impact on other populations. Furthermore, this geographic variation suggests plausible roles for distinctive environmental, infectious, and/or genetic risk factors in the regions, as supported by Asombang et al's systematic review and meta-analysis on disease epidemiology, risk factors, management, and outcomes, 23 which was conducted in 2019. To guide prevention and early detection initiatives in this area, it will be necessary to identify environmental, molecular, and genetic elements, as well as any potential interconnections, that contribute to the high incidence of this disease along the country’s high-risk regions.
Eight articles49-51,53,54,58,60,61 revealed several types of variables, ie, environmental (living or working), nutritional, behavioral, infectious, and sociodemographic factors, that are linked to esophageal cancer. According to a study, drinking water while eating had a preventive effect on the disease. 49 The other 2 investigations49,58 found that eating hot food, such as hot porridge, increased the risk of developing an esophageal tumor. According to a study by Deybasso et al 2021, eating oatmeal quickly, drinking coffee that is extremely hot, and drinking a lot of coffee were also among the risk factors of EC (58). Similar to this, the study by Dessalegn B et al from 2022, 64 revealed that drinking 2 or more cups of tea or spice tea per day and having mouth or tongue burn were risk factors. 60 People who regularly ate porridge had the highest chance of acquiring EC compared with those who typically ate other foods like infera.51,58 All of these exposed the esophagus to heat because hot food and drinks may damage the esophageal mucosa, and skipping drinks while eating can intensify the effect by letting carcinogens stay in contact with the esophageal mucosa for a longer period of time. In contrast, consuming water while eating may help lower the food’s temperature. Furthermore, a systematic review by Islami F et al extrapolated from studies that tea and coffee may pick up some possibly cancer-causing pollutants during processing, such as polycyclic aromatic hydrocarbons (PAH) and mycotoxins, 66 which could also be applicable for porridge.
Daily fruit and vegetable consumption has been cited as a preventive measure against esophageal cancer by Leon ME et al (2017) and Dessalegn B et al (2022).53,60 This may be due to the fact that fruits and vegetables are high in vitamins and minerals,16,21 which are protective against EC. However, Leon et al. 53 ’s 2017 study found that eating a salty diet was associated with an increased chance of developing an esophageal tumor . According to the research analyzed in the systematic review by Banda KJ et al (2020), a high-salt diet may cause damaged esophageal cells to multiply and produce DNA, which would raise the likelihood of developing EC (67). A study by Deybasso HA et al (2021) stated that low intake of dairy products had a risk of EC. However, Castro et al 68 's (2018) systematic review and meta-analysis found no evidence of a link between EC and milk or dairy products . Homemade barley beverages created without alcohol, known as “kenneth,” have been linked to an increased risk of esophageal cancer. 58 The potential risk associated with the consumption of homemade beverages prepared from barley may be related to the addition of sweets and/or the creation of hazardous compounds during the brewing process. This may be because roasting starchy meals at high temperatures produces acrylamide, which is damaging to DNA and neurons and has been linked to a higher risk of developing cancer. The other option might be connected to how “kenneth” picks up some cancer-causing compounds during its production by wood fire, such as polycyclic aromatic hydrocarbons (PAH) and mycotoxins. 66 Consumption of raw meat, especially red meat, has been linked to an increased risk of esophageal cancer. This might be because red meat contains N-nitroso compounds, which are thought to be carcinogens,21,69 and Ethiopians are accustomed to eating raw meat, which exposes them to these compounds. Dessalegn et al 60 (2022) identified sorghum consumption as a risk factor for EC. A plausible explanation could be that tannin is abundant in sorghum (Kao Liang), particularly the variety with brown or red seeds. Tannins break down proteins in enzymes and the mucosa. Polyphenolic biomolecules are responsible for the binding and precipitation of proteins and a variety of other chemical substances, such as alkaloids and amino acids. The 4 locations of the world with the highest rates of esophageal cancer were also the regions where sorghum consumption was the highest. 70
According to 2 studies, esophageal cancer was much more common among people aged 35 years than among those under that age.51,60 This is because as people age, their risk of developing esophageal cancer rises. 23 People who went to school (ie, had any education) and Christian followers (compared to who practice other religion) had a lower likelihood of developing the tumor.53,54 It is possible that the temporal relationship between religion and health is inverted, which would explain the association between religion and esophageal cancer by the confounding effects of earlier health status. In other words, cancer patients are more inclined to adopt a religious or spiritual outlook. However, in terms of coping, support, hope, and purpose, religion is significant for cancer patients. Monthly income less than 35-USD, were reported as a risk factor for EC by Dessalegn B, et al, 2022. The conclusion is backed by a systematic review and meta-analysis of studies conducted in Africa, which found that people with no monthly wage had a higher chance of acquiring EC than people with large salaries. 23
According to Leon ME et al (2019) and Dessalegn B et al, (2022),54,60 tobacco users (ie, any use) were at a significant risk of developing esophageal cancer. This finding was at odds with a study by Leon et al 53 (2017) that claimed there was no connection between smoking and esophageal cancer . The umbrella review by Castro et al 68 (2018) concluded that current smokers had a significantly higher risk of ESCC than never smokers. Two investigations by Leon ME et al (2017) and Madebo T et al (1994) found no association between EC and drinking alcohol.50,53 However, Dessalegn et al.’s recent study (2022) revealed that drinking alcohol may be a risk factor for EC. Even at high levels of intake, no significant relationships were discovered in most meta-analyses, according to the umbrella review of Castro et al (2018). While alcohol may enhance insulin sensitivity or serum lipid and lipoprotein levels, all of which are crucial for EAC risk, other research in the review revealed a protective impact of low to moderate alcohol use on EAC risk. In contrast, a systematic review and meta-analysis of a Japanese study found that those who drank the equivalent of 100 g of pure alcohol per day had a higher chance of developing esophageal cancer than those who never drank alcohol. 24 Dessalegn et al 60 identified khat chewing as a risk factor for EC in 2022. In contrast, earlier research by Madebo T. et al (1994) and Leon ME et al (2017) found no connection between Khat chewing and EC.50,53 A systematic review and meta-analysis by Chong ZX et al (2020) revealed the same contentious results, with 4 studies showing that khat causes cancer with low evidence level, 3 showing that khat has an anticancer effect with moderate to high evidence level, and 1 suggesting that khat is unrelated to cancer. 71
Deybasso HA et al (2021) reported that cooking food in a sleeping room and the use of chemical containers 58 were risk factors, whereas Dessalegn B, et al, 2022 reported that residing in a rural area was a risk factor for esophageal malignancy. 60 The majority of cases were from rural areas where food preparation uses wood that might produce carcinogenic substances such polycyclic aromatic hydrocarbons (PAH), 66 making cases more likely to be exposed. The rural community, on the other hand, has a frequent practice of reusing leftover chemical containers for various purposes, such as storing food and water that could expose them to carcinogenic substances. Exposure to X-ray was reported as a risk factor for esophageal cancer, which could be explained as ionizing radiation is a high-energy wavelength or particle that penetrates tissue to reveal the body’s internal organs and structures. This radiation is produced by X-ray imaging. This could damage DNA, and while cells usually repair most damage, they can occasionally make mistakes, leaving small patches of damage that can lead to DNA mutations years later. In addition, the study found that compared with people who were not employed, farmers had a higher risk of acquiring esophageal cancer. 51
Although the association was not well investigated, HPV and H. Pylori were the 2 infections detected in the tumor of the esophagus. 54 To substantiate this, Castro et al (2018)’s umbrella review of 7 studies found a strong correlation between EC and HPV infection. The review concluded that there was no correlation between HP and ESCC, but HP infection had a protective impact on EAC. 68
A total combined sample size of 1728 patients was used in 5 investigations to describe the results. A Approximately 18% of the patients were still alive, 47.28% had already passed away, and for 34.72%, the outcome status was unknown at the time of study.52,55,56,63,64 Although the survival rate for patients with esophageal cancer varied over time, 3 of the articles measured it.55,56,63 According to 2 investigations, patients with esophageal cancer had median survival times of 4 months 55 and 6 months. 63 Fifty-six (17.63 per 1000 person-month) esophageal cancer cases were still alive at the end of the entire follow-up period (3176 person-months).55,63 According to the research done by Hassen HY et al (2020), the patient survival rates at 1, 2, and 3 years were, respectively, 14.4% [95%CI: 11.0-18.9], 6.3% [3.9%-10.2], and 2.4% [.9%-6.0%]. 55 Based on the study by Feyisa JD et al (2023), the survival rate for esophageal cancer cases at 6 months, 1 year, and 2 years was 54.6% (95%CI:47.5%-61.2%), 19.5% (13.8% −25.9%), and 2.0% (.45%-5.9%), respectively. Forty-three (18.7%) patients’ conditions were unclear. Only 17 patients (7.4%) were still living at the time of the analysis, according to the study. 63 In a separate study, Wondimagegnehu et al (2020) found that 194 cases survived for 6 years, whereas 26 cases (3.3%) died. However, survival status was uncertain in 557 (71.7%) of the cases. 56 The 4 studies discussed the relationship between patient survival and various forms of treatment. Patients who received chemotherapy,55,59,63,64 surgery,55,64 or radiotherapy 59 had considerably better survival rates than those who received no treatment. The studies in this scoping review did not investigate the superior treatment that boosted esophageal cancer patient survival, nor did they provide evidence of the effect of immunotherapy on esophageal cancer patient survival. However, paclitaxel and platinum-based concurrent chemoradiotherapy (TP-CRT)-neoadjuvant offers an overall survival advantage over platinum and 5-fluorouracil-based concurrent chemoradiotherapy (PF-CRT)-neoadjuvant, especially for the SCC population, according to the results of an earlier systematic review and network meta-analysis by Huang TC et al (2015). 72
Strengths and Limitations of the Scoping Review
This review applied a systematic and rigorous search strategy that retrieved several articles to answer our research questions and objectives. Each element from the PCC mnemonic framework was searched by MeSH term and multiple keywords using truncations, proximity search, phrase search, and appropriate field tags to target all relevant studies. However, we may have omitted some relevant studies published in other languages that are not accessible freely. Additionally, the review excluded abstracts for which we could not access the full document.
Conclusions
This study presents a national overview of the most recent academic research on regional and temporal distribution of esophageal cancer, time to treatment outcome, and factors. However, the extensive existing data from this study support the idea that esophageal cancer incidence varies across the nation and from region to region.
The review identified significant risk factors for the disease, such as not drinking water while eating, drinking hot food and beverages, avoiding fruits and vegetables, eating a salty diet, consuming little dairy products, and making sorghum the main food source. Other risk factors included age, being a farmer, not attending school, practicing another religion than Christianity, cooking food in a sleeping area, being exposed to x-rays, drinking nonalcoholic homemade drinks like “Kenneth”, and using chemical containers. Studies on the relationship between esophageal cancer and cigaret usage and/or alcohol consumption are contradictory.
Similar to this, the review found many types of factors linked to esophageal cancer patients’ survival. Although better treatment that increased the survival of patients with esophageal cancer was not explored, chemotherapy, surgery, and radiotherapy enhanced survival despite the presence of additional risk factors.
Implication
Our study highlights the necessity for more thorough research to show improved treatment options for increasing the survival rates of esophageal patients in the nation. More patients’ treatment results are unknown, necessitating thorough research. Because most studies simply employed frequency or proportion to place patients in regions or zones of origin, there is a need for in-depth research on the spatiotemporal clustering of esophageal tumors. If the lowest structure was employed to show disease clustering, the precise exposure status of the patients could be determined.
Since most research relies on secondary data and patients who visit medical facilities, particularly in the nation’s capital, more sociable primary and community-based investigations may be able to pinpoint more important risk factors for the disease. Based on the disease’s histological subtype, risk variables were not found. To examine the interplay of many factors on spatiotemporal distribution, time to treatment outcome, and outcome clustering for esophageal cancer, practitioners and researchers will be encouraged by the insights gained from this study.
Funding
Most research49-53,57,60-62,64,65 failed to mention whether or not they had received financing. Funding for 2 studies58,62 was not provided. The junior Scholars fellowship Program of Medical Education Partnership Initiative program of Addis Ababa University School of Medicine, 59 the International Agency for Research on Cancer Section of Environment and Radiation and the Infections and Cancer Biology Group and from the American Cancer Society, 54 Addis Ababa University (partial), 55 and Addis Ababa University School of Public Health through the esophageal cancer thematic research project award with support from Martin-Luther University Halle-Wittenberg, Halle (Saale), German, 63 and Dr Adamu Addissie 56 provided funding for the other studies. The sponsors were not involved in the data collection, analysis, manuscript preparation, or publication processes, according to the authors. No funding was provided by any source for this scoping review.
Footnotes
Authors’ Contributions
The scoping review was conceptualized by TKB and
Acknowledgments
We are grateful to the Addis Ababa University library for providing us with access to databases like Hinari and its internet service. We wish to express our gratitude to every author whose work was included in the scoping review. We also appreciate the two reviewers’ helpful criticisms and recommendations. Last but not least, we sincerely thank all of the open databases we used to access the studies.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
Because no primary data were obtained and the study was only a scoping study, ethical approval was not sought.
Data Availability Statement
The appendices of this published article provide the formats used for manuscript preparation and data extraction for this scoping study. The body of the manuscript elsewhere contains the complete electronic search methodology for a database. Requests for additional information can be made to the corresponding author.