
Abstract
Background
ZEB1-AS1 acts as an oncogene in hepatocellular carcinoma, accelerating tumor growth and promoting metastasis. However, its roles in colorectal cancer (CRC) remain unclear.
Methods
In this study, we determined the expression of ZEB1-AS1 in CRC tissues by quantitative real-time polymerase chain reaction (qRT-PCR). Additionally, we investigated the relationship between various clinicopathological features of CRC patients and ZEB1-AS1 expression, and evaluated the diagnostic and prognostic value of ZEB1-AS1 in CRC.
Results
We found that ZEB1-AS1 expression was significantly higher in CRC tissues than in adjacent normal colorectal tissues. Moreover, its expression was significantly correlated with tumor size, differentiation degree, TNM grade, metastasis, depth of invasion and Dukes' classification, but not with sex, age, location and organization. In addition, at the optimal cutoff value of 2.340, the values of diagnostic sensitivity and specificity amounted to 63.0% and 90.7%, respectively, with an area under the curve (AUC) of 0.846 (95% CI, 0.797-0.895). Finally, CRC patients of the high ZEB1-AS1 expression group had a poorer prognosis and a significantly lower survival rate than those of the low expression group, and Cox regression analysis indicated that ZEB1-AS1 expression and metastasis were independent predictors of poor prognosis.
Conclusions
Our data suggest that ZEB1-AS1 has no obvious early diagnostic value, but it may be utilized as a new prognostic biomarker for CRC.
Introduction
Colorectal cancer (CRC) is the third most commonly diagnosed cancer in males and the second in females. It had high incidence and mortality rates in 2012, and importantly, its incidence is on the rise (1). In China, CRC in 2011 was the cancer with the fifth highest incidence (310,244 newly diagnosed cases) and mortality (149,722 deaths) (2). Early-stage CRC has a very high cure rate when treated with surgery followed by radiotherapy and chemotherapy. In contrast, relapsed and metastatic CRC are still difficult to cure (3). Therefore, new early diagnostic, progressive and prognostic markers are urgently required.
Long noncoding RNAs (IncRNAs) are noncoding RNAs with a length greater than 200 nt and are known to be involved in tumorigenesis and tumor progression (4). Accumulating evidence demonstrates that dysregulated IncRNAs could serve as novel biomarkers for early diagnosis, and for metastasis, recurrence and poor prognosis in many cancers (5-9). Current studies have focused on ZEB1-AS1 (ZEB1 antisense RNA 1), a IncRNA involved in the expression of zinc finger E-box-binding proteinl (ZEB1). By directly repressing E-cadherin, which is an epithelial to mesenchymal transition (EMT) inhibitor, the ZEB1 protein enhances EMT, a process that may promote metastasis (10). A previous study showed that ZEB1-AS1 acts as an oncogene in hepatocellular carcinoma, accelerating tumor growth and promoting metastasis; it exerts this function by up-regulating the expression of ZEB1 through directly targeting the gene's promoter, and the increased level of ZEB1 leads to the induction of EMT (11). In this study, we set out to investigate the expression of ZEB1-AS1 in CRC tissues, to examine the relationship between various clinicopathological features of CRC patients and ZEB1-AS1 expression and to clarify the diagnostic and prognostic value of ZEB1-AS1 in CRC.
Methods
Patients and tissue samples
A total of 108 tissue samples were obtained from patients with CRC who were recruited from January 2013 to December 2016 at the Siping City Centre People's Hospital before receiving chemotherapy or radiation therapy. All of the patients were followed up, with the last follow-up performed 3-48 months after surgery. All participants signed informed consent forms. All experiments were approved by the ethics committee of the Siping City Centre People's Hospital. The diagnosis and clinicopathological characteristics were confirmed by 2 pathologists. CRC tissues and adjacent normal colorectal tissues (at least 5 cm away from the primary site) were obtained during radical resection and immediately stored at −80°C until used for total RNA extraction.
RNA extraction and quantitative real-time polymerase chain reaction
Total RNA was extracted from CRC tissues and adjacent normal colorectal tissues using the TRIzol reagent (Invitrogen, Carlsbad, CA, USA) according to the manufacturer's protocols. Complementary DNA (cDNA) was synthesized by reverse transcription of 1 μg of total RNA using the PrimeScript RT Reagent Kit (TaKaRa, Kusatsou, Japan) according to the manufacturer's protocols. Subsequently, quantitative real-time polymerase chain reaction (qRT-PCR) was conducted using SYBR Premix Ex Taq (TaKaRa) in an Applied Biosystems 7500 system (Applied Biosystems, Foster City, CA, USA) to determine the expression level of ZEB1-AS1, with GAPDH as a normalizer. Primers for ZEB1-AS1 and GAPDH were purchased from GENEWIZ(Suzhou, Jiangsu, China) and were as follows: ZEB1-AS1, forward 5′-CCGTGGGCACTGCTGAAT-3′ and reverse 5′-CTGCTGGCAAGCGGAACT-3′; GAPDH, forward 5′-CCCATCACCATCTTCCAGGAG-3′ and reverse 5′-GTTGTCATGGATGACCTTGGC-3′. Gene expression was measured in triplicates. Quantitation was based on the 2−ΔΔCt method. Results were expressed as fold induction. Each experiment was repeated 3 times.
Statistical analysis
All statistical analyses were performed using SPSS 19.0 software (IBM Inc., USA). The differences in the expression of ZEB1-AS1 between CRC tissues and adjacent normal colorectal tissues were evaluated using an independent t-test. Correlation analyses of ZEB1-AS1 expression with the various clinicopathological features was performed using the chi-square test. The diagnostic value of ZEB1-AS1 and the optimal ZEB1-AS1 level cutoff value for diagnosis were determined using a receiver operating characteristic (ROC) curve. Survival rates were estimated using the Kaplan-Meier method. Multivariate analysis of the prognostic factors was performed using Cox regression analysis. A p value <0.05 was considered statistically significant.
Results
Expression of ZEB1-AS1 was up-regulated in CRC patients
The expression of ZEB1-AS1 in CRC tissues and adjacent normal colorectal tissues was evaluated by qRT-PCR analysis. Results indicated that ZEB1-AS1 expression in CRC tissues was significantly higher than that in adjacent normal colorectal tissues (p<0.01) (Fig. 1A) with a fold change of at least 1. Patients with a relative expression ratio (ZEB1-AS1 in CRC tissues vs. ZEB1-AS1 in adjacent normal colorectal tissues) higher than 1 (log2(1) = 0) accounted for 84.26% (91/108) of all patients (Fig. 1B).
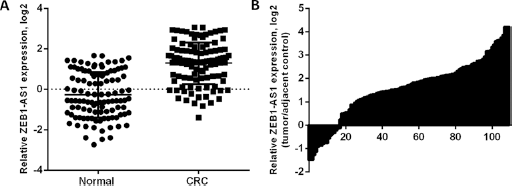
Expression of ZEB1-AS1 in colorectal cancer (CRC) tissues and adjacent normal colorectal tissues. (
ZEB1-AS1 correlates with clinicopathological characteristics of CRC patients
The relationship between various clinicopathological features of the CRC patients and ZEB1-AS1 expression was investigated and the results are shown in Table I. CRC patients were divided into 2 groups according to how their ZEB1-AS1 expression compared with the median ZEB1-AS1 expression value (2.58): the low expression group (ZEB1-AS1 expression <2.58) and the high expression group (ZEB1-AS1 expression ≥2.58). There was no significant correlation between ZEB1-AS1 expression and sex, age, location or organization (p>0.05). In contrast, the expression of ZEB1-AS1 was significantly correlated with tumor size, differentiation degree, TNM grade, metastasis, depth of invasion and Dukes' classification (p<0.05).
Association between clinicopathological characteristics and IncRNA ZEB1-AS1 expression
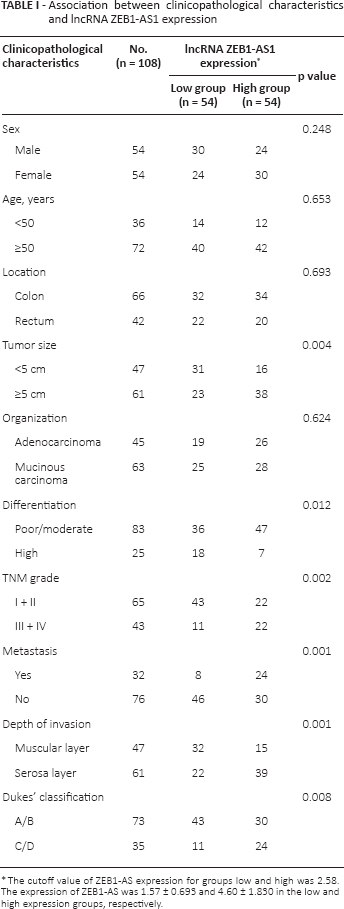
The cutoff value of ZEB1-AS expression for groups low and high was 2.58. The expression of ZEB1-AS was 1.57 ± 0.693 and 4.60 ± 1.830 in the low and high expression groups, respectively.
Similar results are shown in Figure 2. Figure 2A shows a significantly higher ZEB1-AS1 expression in CRC tissues with tumor size >5 cm than with tumor size <5 cm and than adjacent normal colorectal tissues. Figure 2B shows a significantly higher ZEB1-AS1 expression in poor + moderate differentiation degree CRC tissues than high differentiation degree CRC tissues and adjacent normal colorectal tissues. Figure 2C shows a significantly higher ZEB1-AS1 expression in III + IV TNM grade CRC tissues than II TNM grade CRC tissues and adjacent normal colorectal tissues. Figure 2D shows a significantly higher ZEB1-AS1 expression in metastasized CRC tissues than primary CRC tissues and adjacent normal colorectal tissues. Figure 2E shows a significantly higher ZEB1-AS1 expression in serosa layer invasion CRC tissues than in muscular layer invasion CRC tissues and adjacent normal colorectal tissues. Figure 2F shows a significantly higher ZEB1-AS1 expression in C + D Dukes' classification CRC tissues than in A + B Dukes' classification CRC tissues and adjacent normal colorectal tissues.
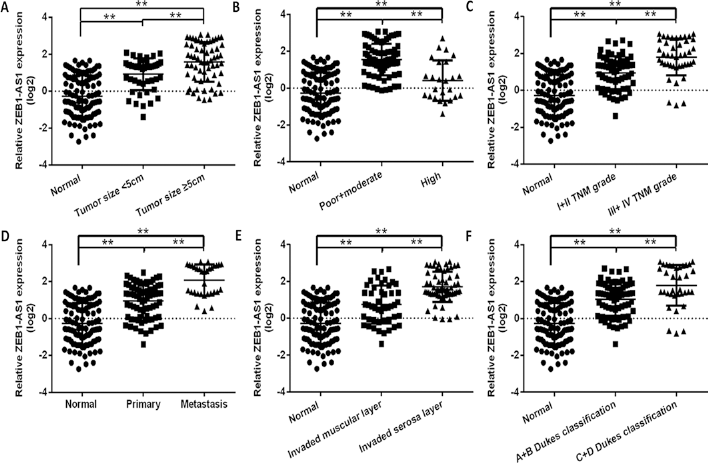
ZEB1-AS1 expression in the control group and other groups. (
Diagnostic and prognostic value of ZEB1-AS1 for CRC
The sensitivity and specificity of CRC diagnosis based on ZEB1-AS1 expression were determined using a ROC curve analysis. At the optimal expression cutoff value (2.340), sensitivity and specificity were 63.0% and 90.7%, respectively, with an area under the curve (AUC) of 0.846 (95% confidence interval [95% CI], 0.797-0.895) (Fig. 3A).
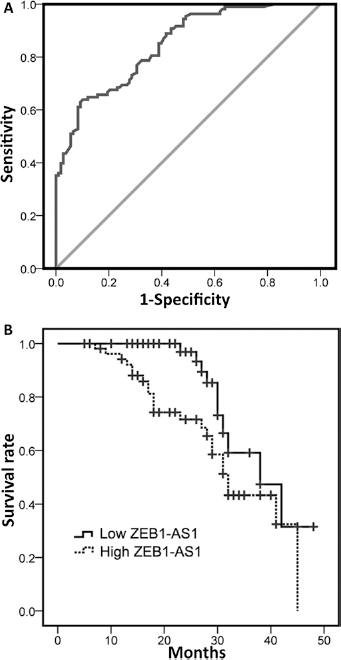
Diagnostic and prognostic value of ZEB1-AS1 for CRC. (
To evaluate the prognostic value of ZEB1-AS1 in patients with CRC, we collected survival period data from all 108 patients included in this study. For the purposes of this analysis, patients were again divided into low and high expression groups according to how their ZEB1-AS1 expression compared with the median ZEB1-AS1 expression (2.54). At the time of the last follow-up (3-48 months after surgery), the numbers of living patients in the low and the high expression groups were 47 (47/54) and 29 (29/54), respectively. The survival rates for each group were estimated using the Kaplan-Meier method, and the results are shown in Figure 3B. CRC patients of the high expression group had a poorer prognosis and a significantly lower survival rate than the patients of the low group (log rank χ 2 = 9.556, p = 0.002).
In addition, we performed univariate and multivariate analysis to determine whether ZEB1-AS1 expression and the clinicopathological parameters of Table I were independent prognostic indicators of CRC patient outcomes. The results are shown in Table II. The results indicated that ZEB1-AS1 expression and metastasis were independent predictors of poor prognosis for CRC patients.
Univariate and multivariate cox proportional hazard models for overall survival in CRC patients
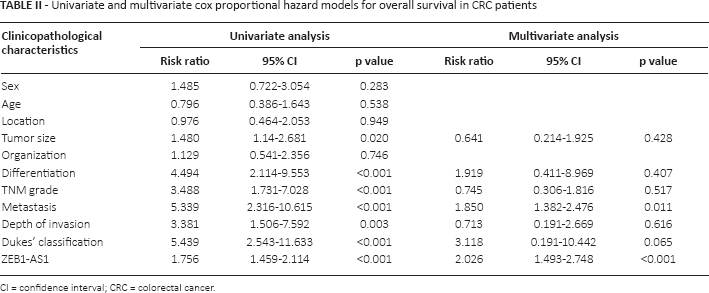
CI = confidence interval; CRC = colorectal cancer.
Discussion
Dysregulated IncRNAs have been linked to many cancer types. The expression of ZEB1-AS1 was found to be significantly higher in cancer tissues compared with adjacent normal colorectal tissues in patients with various carcinomas, such as hepatocellular carcinoma (11), esophageal squamous cell carcinoma (12), glioma (13), osteosarcoma (14, 15) and bladder cancer (16). Our study of CRC gave consistent results, as it showed an increased expression of ZEB1-AS1 in CRC tissues compared with adjacent normal colorectal tissues. In more detail, the patients in whom the relative expression ratio (ZEB1-AS1 in CRC tissues vs. ZEB1-AS1 in adjacent normal colorectal tissues) was higher than 1 accounted for 84.26% (91/108) of all patients, a percentage similar to the ones reported for ZEB1-AS1 expression in other cancers.
ZEB1-AS1 acts as an oncogene, accelerating tumor growth and metastasis. ZEB1-AS1 silencing in glioma cells significantly inhibited cell proliferation, migration and invasion; induced G0/G1 phase arrest; promoted apoptosis; inhibited cyclin D1, cyclin-dependent kinase 2 (CDK2), ZEB1, matrix metalloproteinase 2 (MMP2), MMP9, N-cadherin and Bax expression; and enhanced E-cadherin and Bcl-2 expression (13). ZEB1-AS1 knockdown in osteosarcoma cells inhibits their proliferation and migration by epigenetically silencing ZEB1 (7). These studies showed that ZEB1-AS1 affects tumorigenesis and tumor progression and might serve as a novel biomarker for the early diagnosis and for a poor prognosis of CRC. In the current study, we found that ZEB1-AS1 expression was significantly correlated with tumor size, differentiation degree, TNM grade, metastasis, depth of invasion, and Dukes' classification, but not with sex, age, location and organization. The results also suggested a positive correlation between ZEB1-AS1 expression and tumor size, TNM grade, metastases or not, depth of invasion, Dukes' classification and a negative correlation between ZEB1-AS1 expression and differentiation degree. In addition, we found that, at the optimal cutoff value of 2.340, the diagnostic sensitivity and specificity were 63.0% and 90.7%, respectively, with an AUC of 0.846 (95% CI, 0.797-0.895). The results suggested that ZEB1-AS1 expression had no obvious value as an early diagnostic marker. Furthermore, CRC patients of the high ZEB1-AS1 expression group had a poorer prognosis and significantly lower survival rate than those of the low ZEB1-AS1 expression group, and Cox regression analysis indicated that ZEB1-AS1 expression and metastasis were independent poor prognosis markers for CRC patients. The results showed that ZEB1-AS1 expression was significantly associated with CRC tumorigenesis and metastasis, and it may possibly be an independent poor prognosis marker. The results of the current study are similar to those of a previous study that reported an association of ZEB1-AS1 with tumor progression and patient survival in esophageal squamous cell carcinoma and glioma (12, 13).
In conclusion, our data suggest that ZEB1-AS1 may act as a new prognostic biomarker but has no obvious early diagnostic value for CRC. Further studies are required to determine whether ZEB1-AS1 could serve as a potential therapeutic target.
Footnotes
Financial support: No grants or funding have been received for this study.
Conflicts of interest: None.