
Abstract
Background
The use of des-gamma-carboxy prothrombin (DCP) as a predictor of the risk of recurrence of hepatocellular cancer (HCC) after liver transplant (LT) has recently gained interest, especially in view of the recent extension of the eligibility criteria of these patients for LT. The aim of the present study is to look into this important matter based on a systematic review and meta-analysis.
Methods
A systematic literature review about the role of DCP in the specific setting of LT for HCC has been conducted.
Results
Three selected studies, which showed a high rate of homogeneity (I2 = 0.0%), confirmed that the tumor marker DCP is a useful predictive factor, indicating a 5-fold increased risk for HCC recurrence after LT (p<0.001).
Conclusions
The meta-analysis enabled us to underline the importance of DCP in the refinement of the eligibility criteria of HCC patients for LT. This information, based on Japanese studies performed in the setting of living-donor LT only, needs further validation in the Western world both in the setting of post-mortem and living-donor LT.
Keywords
Introduction
Several tumor markers have been developed for the diagnosis and prognosis of hepatocellular cancer (HCC). Unfortunately, alpha fetoprotein (AFP), the most commonly used HCC marker, is significantly elevated in less than half of patients only (1, 2). Consequently, other markers have been looked at in order to improve the sensitivity and specificity of tumor diagnostics. Des-gamma-carboxy prothrombin (DCP), also known as protein induced by vitamin K absence-II (PIVKA-II), has been investigated almost exclusively in Asian countries as a useful liver tumor marker in the last 2 decades. DCP differs from prothrombin by the composition of amino-acid residues, lacking the ability to interact with other coagulation factors. This “abnormal prothrombin” was initially discovered in the blood of patients presenting vitamin K deficiency or receiving vitamin K antagonists (3). In 1984, Liebman et al (4) reported for the first time that serum DCP was also increased in HCC patients. The exact mechanism by which DCP is produced by the tumor is not yet fully understood (5), but the normalization of DCP levels after curative cancer treatment clearly indicates that the tumor is the source of its production (6). Numerous, almost exclusively Eastern, reports underlined the value of DCP in the diagnosis of HCC and carefully compared the evolution of both AFP and DCP as tumor markers (7), but few of these studies looked at its role for the risk of recurrence after liver transplant (LT). This study aims to analyze the value of this marker in the selection process of HCC patients waiting for LT and to thereby define DCP as a risk factor for recurrence after LT. For this purpose a meta-analysis investigating the association between pre-LT DCP levels and the HCC recurrence rate after LT was performed.
Materials and methods
Search strategy
A systematic search was done to identify relevant studies focusing on the role of DCP in the setting of LT. The search strategy was in accordance with the Preferred Reporting Items for Systemic Reviews and Meta-Analysis (PRISMA) guidelines, as well as PRISMA for abstracts (8). We searched the electronic databases MEDUNE-PubMed and Cochrane Library using the following MeSH terms: (des gamma carboxy prothrombin OR protein induced by vitamin K antagonist-II OR PIVKA OR DCP) AND (liver transplant OR liver transplantation OR living donor LT). Studies published before December 1, 2016 were taken into consideration.
Screening process
The inclusion criteria were as follows: papers written in English and containing sufficient data on survival analysis (disease-free survival [DFS]) and being approved by institutional ethical review boards.
Papers were excluded according to the following criteria: studies lacking sufficient statistical details, review articles, nonclinical studies, letters, expert opinions, conference summaries and case reports. In case of studies coming from the same center, only the most recent presenting all the statistical details was considered in order to avoid the risk of analyzing the same patients in the final analysis.
Data extraction
Two authors (QL and JL) independently reviewed the identified studies and their extracted data. In case of disagreement, the paper was discussed by all the authors. For each study the following characteristics were collected: first author's name, year of publication and reference, country/city, number of patients, DCP cutoff value, time of enrollment, patient age, follow-up in months, type of LT (living or deceased donor), type of statistical analysis and characteristics of the study (Tab. I). The quality of the papers was assessed using the Newcastle-Ottawa Quality Assessment Scale: studies with scores >6 were defined as high-quality studies (9).
Characteristics of studies included in the meta-analysis about the association between DCP and DFS in HCC patients undergoing LT
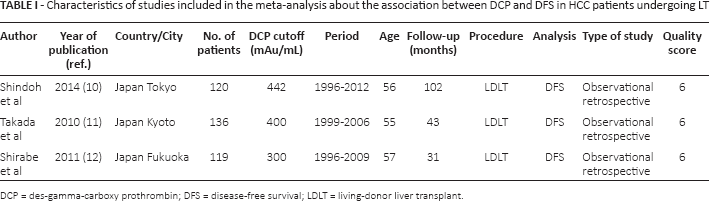
DCP = des-gamma-carboxy prothrombin; DFS = disease-free survival; LDLT = living-donor liver transplant.
Patient eligibility criteria
The patient eligibility criteria were investigated according to the different analyzed articles. The selection criteria were similar but not identical among studies. In all cases, the liver recipients presented early-stage HCC developed in a liver with preexistent liver disease in the absence of extra hepatic metastases and macrovascular invasion. No conventional upper tumor limits (such as the Milan Criteria) were commonly adopted.
Statistical analysis
Different DCP cutoffs were observed among studies. The DFS end-point in the different studies corresponded to 5 years after LT. Summary measures were extracted from each study and used to generate a pooled hazard ratio (HR). Cochran's Q test and the Higgins I2 statistic were used to assess heterogeneity. The result was defined as heterogeneous when the Higgins I2 statistic was ≥20% or the p value ≤0.10 for the Q test. Only the random-effects model was used, starting from the assumption that a common HR was unreliable in the analyzed studies due to the broad eligibility criteria and the different DCP cutoff values used. HR was considered statistically significant when p was <0.05. HR and 95% confidence intervals (CI) >1 revealed that patients with high DCP values had poor prognosis (higher risk of recurrence), whereas a result <1 had the opposite meaning. Analysis was performed using Stata/SE 14.0 (StataCorp LLC).
Results
The selection process of the articles is displayed in Figure 1. After examination of the various databases, 99 articles were identified and screened. After reading the titles and abstracts, we removed 40 articles. Fifty-six of the remaining 59 papers were considered ineligible after full-text evaluation: 22 were review articles, 7 were written in a language other than English, 4 were case reports, and 1 was a letter to the Editor. Several studies were excluded from the evaluation because they were encompassed in a more recent “final” study originating from the same center (n = 6) or because there was insufficient information about DFS or recurrence (n = 16).
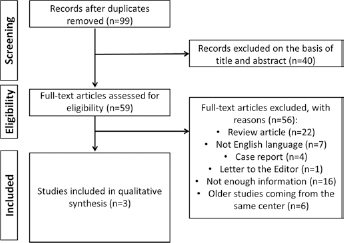
PRISMA flowchart of the literature search and study selection.
Finally 3 papers only, all originating from Japan (Tokyo, Kyoto and Kyushu-Fukuoka) and all dealing with living-donor LT, allowed to appropriately investigate the role of DCP for the risk of recurrence after LT (10-12). The studies had different but relatively close cutoff values of DCP, ranging from 300 to 442 mAu/mL (corresponding to 5.7-8.4 ng/mL [1 ng = 52.6 mAu]).
The 3 studies included 375 patients having median age of 55-57 years (ranges 21-70) and a 70.7%/29.3% M:F ratio. HCV positivity was observed in 58.9% of patients, with 62.4% of the cases undergoing pre-LT neoadjuvant treatment(s). One hundred fifty-seven (41.9%) cases were outside the conventional Milan Criteria. Fifty-four (14.4%) recurrences were observed. Forty-one (10.9%) patients died of their tumor recurrence and 38 (10.1%) of non-HCC-related causes (Tab. II).
Patient characteristics and post-LT course of the investigated population
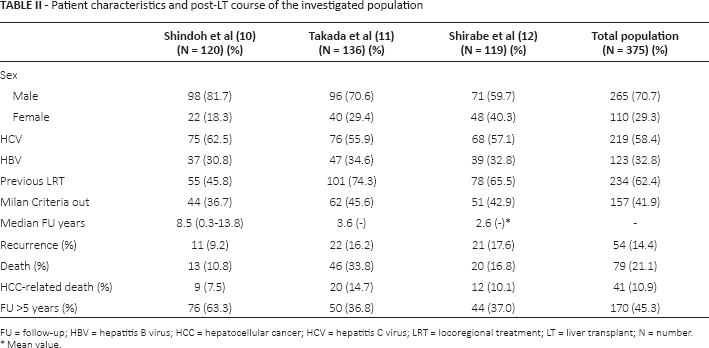
FU = follow-up; HBV = hepatitis B virus; HCC = hepatocellular cancer; HCV = hepatitis C virus; LRT = locoregional treatment; LT = liver transplant; N = number
Mean value.
All the investigated papers were retrospective and observational cohort studies presenting a rate of 6/9 on the Newcastle-Ottawa Quality Assessment Scale. Looking specifically at the different categories, all articles scored 4/4 points in Selection, 1/2 points in Comparability, and 1/3 points in Outcome.
When the overall impact of DCP on post-LT recurrence was considered, there was a strong relationship between shorter DFS and elevated DCP values (HR = 5.04, 95% CI 3.32-7.67; p<0.001). Cochran's Q test was 0.31 (p = 0.86), with an excellent Higgins I2 statistic (0.0%), showing good homogeneity between the examined studies (Fig. 2).
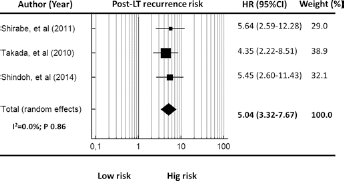
Forest plot of hazard ratios and 95% confidence intervals for the association between DCP and DFS in HCC patients undergoing LT. Weights are from fixed- and random-effects analyses. CI = confidence interval; DCP = des-gamma-carboxy prothrombin; DFS = disease-free survival; HCC = hepatocellular cancer; HR = hazard ratio; I 2 = Higgins I-squared; LT = liver transplant.
Discussion
The present meta-analysis confirms the predictive role of DCP for the risk of tumor recurrence after LT. Unfortunately, only a very small number of studies clearly investigated this very intriguing topic. Several difficulties were observed in constructing a rigorous meta-analysis. First of all, most studies originated from Japan and explored the role of DCP only in the setting of living-donor LT. Only 1 study from the US investigated the role of this marker in 79 deceased-donor LTs; unfortunately, insufficient data were available in relation to post-LT recurrence (13). More than 90% of the published papers related to DCP are produced by 3 Japanese centers, namely the Universities of Tokyo, Kyoto and Kyushu-Fukuoka. All 3 expanded the inclusion criteria of HCC patients for LT based on the combination of morphological tumor aspects and biological tumor behavior expressed by DCP and/or AFP secretion. The “Tokyo HCC-LT Criteria” include patients presenting with ≤5 tumors, each tumor having a diameter of ≤5 cm, in combination with AFP and DCP levels of ≤250 ng/mL and ≤450 mAU/mL, respectively (10, 14). The “Kyoto HCC-LT Criteria” include patients presenting ≤10 tumors, all having a diameter of ≤5 cm, in combination with a DCP level of ≤400 mAU/mL (11, 15-17). Finally, the Fukuoka group focused on the creation and internal validation of the “Kyushu Criteria”, including patients presenting a tumor sized ≤5 cm and a DCP level of ≤300 mAU/mL (12, 18-20).
The combination of morphological and biological tumor characteristics allowed not only to expand the inclusion criteria for LT but, most interestingly, to improve DFS, even for Milan Criteria-out patients. The Fukuoka group investigated the role of the Kyushu Criteria in 54 Milan Criteria-out patients, convincingly showing that the addition of DCP to the conventional morphological criteria allows to raise the ability of identifying “low-risk for recurrence” patients, even if they are outside the conventional criteria (21).
Of note in this context is the large Japanese HCC-LT multicenter study comprising 653 living-donor-transplant recipients performed in 49 different centers (22). This study showed that the combination of the Milan Criteria and AFPDCP levels (AFP ≤200 ng/mL and PIVKA II ≤100 mAU/mL) allows to further improve the selection process of HCC patients for LT. Despite the fact that this study could not be retained in our final meta-analysis due to the lack of sufficient information about DFS and the use of very different DCP cutoff values (≤100 and >1,000 mAU/mL), its results are in line with those of the 3 aforementioned included studies (22).
All 3 investigated Japanese studies showed intermediate quality according to the Newcastle-Ottawa scale (6/9 points), their weight being hampered by the short follow-up, the limited number of patients ending the follow-up period, and the absence of control patients. Despite these limitations, the obtained results were interestingly convergent, showing the role of DCP as a risk factor for HCC recurrence after LT, this risk being increased 5-fold if the DCP level encompasses values of 300-450 mAU/mL. Such convergence was probably reinforced by the fact that the investigated patients belonged to a same geographical area and presented tumors with similar biological behaviors.
No Western LT studies related to DCP have been available for analysis so far. Given the long-standing DCP-HCC experience in the Eastern world, it is quite surprising that the Western liver community has not integrated this marker in the therapeutic algorithm for HCC patients, the more so because HCC is becoming one of the most common indications for LT in both Europe and North America. The main reason could be the lack of reimbursement for the test and, more importantly, the lack of technical know-how and support in Western laboratories to perform this test reliably.
In relation to the predictive value of DCP for tumor recurrence after LT also in a European setting, some important issues should be taken into account: a) Western and Eastern practice differences in terms of living-donor LT, waiting times and locoregional treatments; b) differences in the indications for LT; c) the possible (albeit debated) difference in the biological behavior of HCC in the West and in the East. It is also important to underline that the DCP level can be strongly influenced by medications such as antitubercular drugs and their derivatives (e.g., rifampicin), vitamin K shortage (e.g., due to malnutrition in cirrhotic patients) and anti-vitamin K medications (e.g., anticoagulants such as warfarin). Vitamin K supplementation the day before blood sampling therefore enables to further increase the discriminatory power of this marker in tumors effectively secreting it (23).
Despite the fact that the potential association between DCP and prediction of the post-LT clinical course of HCC patients could be carefully calculated using the most recent and statistically solid studies and attempting thereby to derive reliable conclusions for clinical applications, our study has some limitations: a) the exclusively Japanese origin of the studies (only 3 could be included in the final analysis) resulted in a limited number of investigate cases (10-12); b) DCP thresholds were different and the patient eligibility criteria were broad; c) no meta-regression analysis could be performed on the available cases. Consequently, the conclusions drawn here are preliminary and a greater number of studies, also including Western ones, are required to validate the predictive value of this marker in relation to tumor recurrence after LT. The authors are confident that including this marker in the therapeutic algorithm for HCC patients will allow to further expand the inclusion criteria of HCC patients for LT in a justified way, allowing more patients to undergo LT without increasing the post-LT recurrence rates.
Conclusion
This meta-analysis suggests that high pre-LT DCP values are associated with higher recurrence rates in HCC patients undergoing LT. The fact that all included studies were Japanese guaranteed good homogeneity. However, more studies, also from the Western world, are needed to corroborate the role of DCP in this oncological transplant context. Inclusion of DCP values in the evaluation process of HCC patients might allow to justifiably expand the inclusion criteria of HCC patients for LT.
Footnotes
Financial support: None.
Conflict of interest: The authors have no conflicts of interest to declare in relation to the content of the paper.