
Abstract
Introduction:
Liver transplantation offers the most reasonable expectation for curative treatment for hepatocellular carcinoma. Living-donor liver transplantation represents a treatment option, even in patients with extended Milan criteria. This study aimed to evaluate the outcomes of hepatocellular carcinoma patients, particularly those extended Milan criteria.
Materials and Patients:
All HCC patients who received liver transplant for HCC were included in this retrospective study. Clinical characteristics including perioperative data and survival data (graft and patient) were extracted from records. Univariate and multivariate analyses was performed to identify significant prognostic factors for survival, postoperative complications and recurrence.
Results:
Two-hundred and two patients were included. The median age was 54.8 years (IQR 53-61). Fifty-one patients (25.3%) underwent deceased donors liver transplantation and 151 patients (74.7%) underwent living donor liver transplantation. Perioperative mortality rate was 5.9% (12 patients). Recurrent disease occurred in 43 patients (21.2%). The overall 1-year and 5-year survival rates were 90.7% and 75.6%, respectively. Significant differences between patients beyond Milan criteria compared to those within Milan criteria were not found. Alpha-fetoprotein level >300 ng/mL, vascular invasion, and bilobar tumor lesions were independent negative prognostic factors for survival.
Conclusion:
Liver transplantation is the preferred treatment for hepatocellular carcinoma and it has demonstrated an excellent potential to cure even in patients with beyond Milan criteria. This study shows that the Milan criteria alone are not sufficient to predict survival after transplantation. The independent parameters for survival prediction are Alpha-Fetoprotein-value and status of vascular invasion.
Keywords
Introduction
Hepatocellular carcinoma (HCC) is among the most common malignancies and leading causes of cancer deaths. Cirrhosis developed as a result of chronic hepatitis virus infection represents the most common cause of HCC. 1,2 There are different treatment approaches available, such as resection, radiofrequency ablation, chemoembolization, radioembolization or liver transplantation (LT), yet there has been no effective medical treatment for HCC till now. In liver cirrhosis patients, poor liver function and high recurrence rate after surgical procedures are main challenges for major liver resections. Interventional treatment options are useful only as bridging therapy since they do not lead to a definitive cure for the disease. Deceased donor liver transplantation (DDLT) or living donor liver transplantation (LDLT) is in these patients with cirrhosis the treatment of choice with curative intension. 3 -6 However, when global organ shortage is considered, survival after LT in the long term is extremely important in terms of justifying the use of the organ or justifying the donor risk in case of LDLT. The widely used definition for prediction of survival is the Milan criteria. However, there are many data in the literature describing good long-term survival of patients with HCC outside Milan criteria. This study aimed to evaluate the outcomes of patients with liver cirrhosis and HCC, who underwent LT at our center.
Materials and Methods
The data of 1,182 patients who underwent liver transplantation at our center between years 2004 and 2019 were retrospectively reviewed. LDLT was performed in 951 patients (80.5%) and 231 (19.5%) underwent DDLT. Patients with a diagnosis of HCC were identified and following data were extracted and analyzed: clinical and demographical characteristics, transplantation indication, model for end-stage liver disease (MELD) score, preoperative alpha-Fetoprotein (AFP) level, tumor-related data (size, histological type, location, pathological examination findings), intraoperative data, postoperative course, primary immunosuppressive therapy used, rejection and its treatment, donor criteria, duration of ischemia, follow-up of the donor, recurrence, and patient/graft survival.
All potential recipients were evaluated using a standard evaluation program for liver transplantation, which includes routine blood tests and virologic assessments, Doppler ultrasonography of the liver, computed tomographic (CT) angiography with portal reconstruction of the liver, pulmonary function tests, cardiovascular examination, and psychiatric evaluation. For LDLTs, donor criteria were age between 18 and 65 years, up to 4th degree relative or a non-relative (for non-relatives the approval of the Regional Ethical Committee was required), remnant liver volume
In patients with proven HCC and with a suitable living donor, the LDLT was the preferred type of transplantation independent of the MELD score. According to the legal guidelines after 2010, all patients listed for DDLT had to be within the boundaries of the Milan criteria. 7 The requirements of our center for LDLT were exclusion of radiological macrovascular invasion and exclusion of extrahepatic manifestations.
Interventional treatments such as radiofrequency, chemoembolization, or radioembolization were performed as a bridging treatment to liver transplantation. Calcinurine inhibitors and prednisone supplemented with mycophenolat mofetil were used for immunosuppression after transplantation. Drug or dose modifications were made individually where necessary depending on the clinical course. Postoperatively, patients were followed every 3 months for the first 2 years, then every 6 months for the next 5 years. History and physical examination, blood tests, AFP assessment, CT or magnetic resonance imaging (MRI) and, if needed, bone scintigraphy and PET-CT were done on each follow-up examination.
Descriptive data are reported as median and interquartile range (IQR) or mean and standard deviation, where appropriate. Mann-Whitney U test was used for the comparison of continuous variables. Fisher’s exact test was used for the comparison of categorical variables. Kaplan-Meier curves were plotted for overall survival and disease-free survival. Because the percentage of events was less than 50%, mean survival estimates with standard errors were reported as descriptive statistics. Multivariate Cox regression analysis was used to estimate hazard ratios (HR), and multivariate logistic regression analysis was used to estimate the odds ratios (OR). A P value <0.05 was considered to indicate statistical significance. SPSS 23.0 for Windows statistical package was used for statistical analyses.
Results
A total of 202 patients with HCC in liver cirrhosis underwent liver transplantation at our center between January 2004 and December 2017 (median age 54.8, IQR 53-61). Liver cirrhosis was caused by hepatitis B in 110 patients (54.4%), hepatitis C in 32 patients (15.9%), cryptogenic in 25 patients (12.3%), alcoholic in 12 patients (6%), and had other etiology in 23 patients (11.4%). The median lab-MELD-score was 13.8 (IQR 13-17), and the median AFP value was 27 ng/mL (IQR 7-109). The Milan criteria were met in 121 patients (60%) and 81 patients (40%) fell outside the Milan criteria. Of all patients, 51 patients (25.3%) underwent DDLT, and 151 patients (74.7%) underwent LDLT. Right lobe LDLT was performed in 146 (96.6%) patients and left lobe LDLT was performed in 5 (3.4%) patients (Table 1). The transplantations were performed in all cases by the same transplant team. The median graft to recipient weight ratio was 1.1 (IQR of 0.9-1.3). The median number of tumor lesions was 2 (IQR 1-4). The median tumor size was 3 cm (IQR 2-5), and the median total tumor volume was 53.61 cm3 (IQR 0.5-496.91). The histopathologic grading was grade I in 42 patients (20.7%), grade II in 122 patients (60.4%) and grade III in 38 patients (18.9%). Microvascular invasion was seen in 22 patients (10.9%), and macrovascular invasion was seen in 11 patients (5.4%). Perioperative death was seen 12 patients (5.9%) due to sepsis, graft failure, cava thrombosis, pulmonary emboli and primary none function. Recurrent disease occurred in 43 patients (21.2%). Median time to recurrence was 13 months (IQR 7-20). The 1-year, 3-year, and 5-year overall survival rates were 90.7%, 88.9% and 75.6%, respectively. On the other hand, the 1-year, 3-year, and 5-year disease-free survival rates were 88.2%, 84.8% and 68%, respectively. Patients who underwent DDLT and LDLT did not differ in terms of overall or disease-free survival (Figures 1 and 2). Also, overall survival and disease-free survival were similar for patients within and beyond Milan criteria (Figures 3 and 4). The univariate logistic regression analyses showed that the survival and recurrence rates were influenced by the preoperative AFP value, grade of the disease, vascular invasion, tumor type and unilobar or bilobar localization of the tumor lesion. However, type of surgery, size of the tumor and Milan criteria did not have any significant influence (Tables 2 and 3). The survival was obviously negatively influenced by recurrence. As shown in Tables 4 and 5, the multivariate regression analyses showed that histopathologic tumor type and pretransplant AFP values were independent predictive factors for survival and recurrence. Recurrence rate was significantly higher in patients with AFP >200 (OR 3.52, 95%CI 1.1-10.9, P = 0.03). The mortality risk was significantly higher in patients with AFP >300 ng/mL (HR 3.27, 95%CI 1.2-8.9, P = 0.02). Independent predictive factors for recurrence and time to recurrence were grade of tumor and histophatologic tumor type. Interestingly, Milan criteria did not have any significant influence on survival nor on recurrence rate or time in the univariate or multivariate analyses.
Clinical Characteristics.
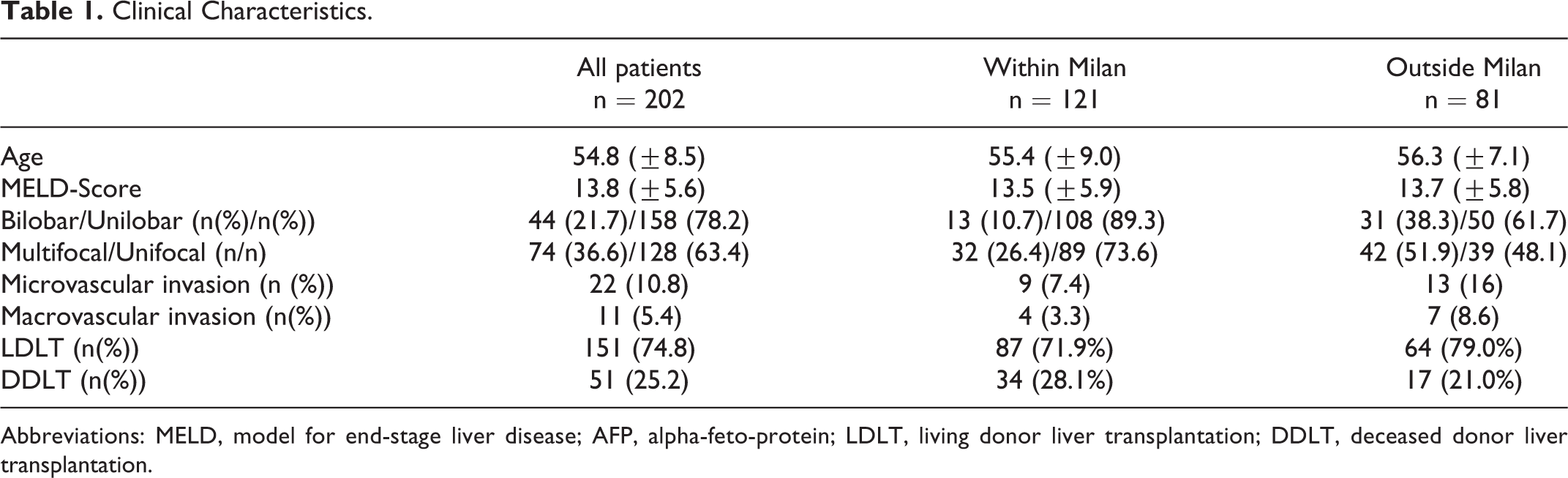
Abbreviations: MELD, model for end-stage liver disease; AFP, alpha-feto-protein; LDLT, living donor liver transplantation; DDLT, deceased donor liver transplantation.

LDLT n = 162, 5-years survival rate 75%. DDLT n = 50, 5-years survival rate 80.0%, P value = 0.92 HR 1.04 (95% CI for HR 0.53-2.02).

LDLT n = 162, 5-years disease free survival rate 71%. DDLT n = 50, 5-years disease free survival rate 76%, P-value = 0.78 HR 0.91 (95% CI for HR 0.48-1.72).

1-, 3- and 5-year survival rates of 91.9%, 81.6% and 76.3% for patients within the Milan criteria (n = 131) and 88.8%, 81.8% and 72.3% for patients outside the Milan criteria (n = 81) [P-value = 0.41 HR 1.22 (95% CI for HR 0.71-2.30)].

1-, 3- and 5-year survival rates of 89.3%, 79.3% and 73.2% for patients within the Milan criteria (n = 131) and 81.4%, 76.2% and 66.3% for patients outside the Milan criteria (n = 81) [P-value = 0.21 HR 1.17 (95% CI for HR 0.84-1.93)].
Univariate Logistic Regression Analyses for Overall Survival.

*P < 0.05 is defined as significant.
Univariate Logistic Regression Analyses for Recurrence Rate.

*P < 0.05 is defined as significant.
Multivariate Regression Analyses for Overall Survival.

*P < 0.05 is defined as significant.
Multivariate Regression Analyses for Recurrence.

*P < 0.05 is defined as significant.
Discussion
Liver transplantation represents the only curative treatment option for HCC patients with approximately 70% 5-year survival rates. 1,7 The difficulty is that in times of organ shortage, the risk for tumor progression while on the waiting list is too high. Another limitation for DDLT is the Milan criteria, which must be fulfilled. Our results showed that HCC patients within Milan criteria and beyond Milan criteria do not differ in terms of long-term survival following liver transplantation and significant proportion of them were beyond Milan criteria. Furthermore, the 1-year liver transplant wait-list dropout rates for patients with HCC are estimated between 10% and 40%. 5 -8 In countries with no mechanism for organ donation, LDLT is the preferred type of transplantation for HCC patients with end-stage liver disease. Milan criteria are often not a limitation for LDLT; therefore, if the patient has a suitable donor, the LDLT is an optimal alternative since the liver transplantation can be performed in all stages of the disease, and patients do not need to wait for an organ. Another benefit is that patients are mostly in significantly better condition with low lab-MELD scores, and excellent outcomes can be expected.
Some publications have described disadvantages of LDLT regarding HCC recurrence as compared with DDLT. 9 -12 Possible explanations are noted as higher rate of more aggressive tumors among the patients who undergo LDLT since these patients would drop off the list while waiting for DDLT, 13,14 increased risk for residual tumor cells due to preserved native vena cava, bile duct and hepatic artery 15 - 17 and increased release of growth factors and cytokines due to stimulation of graft proliferation in partial grafts are further possible explanations described in the literature. 18 - 20 We have not seen this phenomenon in our study; patients who underwent LDLT and DDLT did not significantly differ in terms of survival and recurrence rates. These results can be based on the fact that we use defined criteria (i.e., exclusion of macrovascular invasion, exclusion of extrahepatic manifestation and exclusion of AFP value over 700 µg/l) for patients with HCC to be suitable candidates for LDLT at our center. Other studies have also shown that there is no difference between the long-term results after LDLT for HCC compared to DDLT when parameters of tumor morphology and biology were taken into account for patient selection. 19
However, to justify the donor risk, the LDLT should have excellent survival rates comparable to those of HCC patients within Milan criteria after DDLT. Consequently, survival prediction is significantly favorable not only for DDLT but also for LDLT. Several studies have shown that many patients with potential for good post-transplant survival are often not viable candidates for DDLT due to Milan criteria requirements. 20 -24 Based on the results of our study and some other published data, more accurate predictions of 5-year survival rates can be achieved by new guidelines such as vascular involvement, preoperative AFP value, histological grading of the tumor and PET positivity. 23 -25 Our study clearly shows that patients with HCC outside of Milan criteria can exhibit excellent survival rates. Parameters such as preoperative AFP-value ≤300 ng/mL, pathologic grading of the tumor, exclusion of vascular invasion and unilobar tumor localization are more important and predict survival and also recurrence much more accurately than Milan criteria alone.
It is notable that AFP level was significantly reduced in patients with cryptogenic liver cirrhosis. Only one patient (3.8%) had an abnormal AFP. Although survival and recurrence rates were similar across different groups for the etiology of liver cirrhosis, the primary disease underlying the liver cirrhosis could still influence tumor biology and consequently prognosis. Total of 25 of our patients had cryptogenic liver cirrhosis (12.3%), which is too small to achieve a statistically significant difference. It is known that the active viral replication in chronic viral hepatitis increases the risk of HCC, 26,27 and there is a positive correlation between specific viral genotypes and cancer development described in the literature. 28 This pattern of cancer development makes the assumption of an association between etiology and tumor biology more likely. However, a correlation between low AFP value and cryptogenic liver cirrhosis has not yet been described.
Retrospective design and related shortcomings are the main limitations of this study. Although our sample size is relatively high, in order to define new and widely accepted criteria for survival prediction and patient selection, which could replace the Milan criteria, the number of patients should be even higher. This would be possible with multicenter studies. Another shortcoming of this study is that we did not have PET scan data for the majority of the patients. Consequently, we could not make statistically sufficient analyses on this data, which could add significant impact on survival prediction.
Conclusions
Our findings suggest that excellent long-term survival can be achieved after LDLT in patients with HCC outside of Milan criteria. New criteria based on tumor biology (e.g., preoperative AFP value, histological grading, status of vascular invasion, uni- or bilobular localization of the lesions) are needed for better survival prediction and patient selection. LDLT should also be widely adopted as the treatment of choice in Western countries in patients with HCC and end-stage disease, in order to avoid tumor progress and reduce the dropout rate while on the waiting list.
Footnotes
Authors’ Note
A. Alim collected and analyzed data and wrote the paper. Y. Erdogan collected and analyzed data. A. Oezcelik designed and mentored the study and contributed important reagents. Y. Yuzer and Y. Tokat contributed important reagents and revised the manuscript.
Ethical Statement
The study was conducted to following the Declaration of Helsinki criteria as well as Declaration of İstanbul criteria. The study was performed as retrospective study with anonymized data analyses. For this setting the local ethical policy does not require IRB approval.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.