The role of serum biomarkers in the surveillance of hepatocellular carcinoma (HCC) is controversial.
OBJECTIVE:
We assessed the diagnostic performances of alpha-fetoprotein (AFP) and protein-induced by vitamin-K-absence/antagonist-II (PIVKA-II) in 388 cirrhotic patients with chronic liver disease (CLD).
METHODS:
Biomarkers were quantified by automated chemiluminescent-enzyme-immunoassays (Fujirebio, Tokyo, Japan) at HCC diagnosis in 258 patients (204 males; median age 66.9 years) and in 130 cirrhotics without HCC (104 males; median-age 60.6 years). CLD etiology in HCC/non-HCC was CHB in 48/35, CHC in 126/56 and Non-Viral in 84/39.
RESULTS:
Overall AUROC values for AFP and PIVKA-II were 0.698 (95%CI 0.642–0.753, 0.001) and 0.780 (95%CI 0.730–0.831, 0.001). AFP/PIVKA-II AUROC (95%CI) were: 0.822 (0.728–0.915)/0.833 (0.739–0.926) in CHB, 0.648 (0.560–0.736)/0.732 (0.650–0.814) in CHC; 0.640 (0.540–0.740)/0.806 (0.722–0.889) in Non-Viral-CLD. AFP/PIVKA-II diagnostic accuracy was 40.5–59.8%/62.7–73.5% and combining both markers 78.2% for CHB, 77% for Non-Viral-CLD and 75% for CHC. AFP correlated with ALT in HCC patients with CHC ( 0.463/ 0.001) and Non-Viral CLD ( 0.359/ 0.047), but not in CHB (treated with antivirals). PIVKA-II correlated with tumour size independently of CLD-etiology ( 0.001) and AFP in CHB patients only ( 0.007).
CONCLUSION:
The diagnostic performance of AFP and PIVKA-II is significantly influenced by the etiology and activity of CLD; their combination provides a better diagnostic accuracy.
Hepatocellular carcinoma (HCC) is the fifth most common cancer in men and the seventh in women worldwide [1]. Chronic liver disease (CLD) induced by chronic infection with major hepatitis viruses (hepatitis B, C and D viruses) and/or steatohepatitis are the main causes of HCC that associate with cirrhosis in about 90% of cases [2]. Age- and sex-specific HCC rates vary in different geographic regions in relation to differences in the prevalence of hepatitis virus infections and other co-factors of CLD. The highest incidence of HCC occurs in sub-Saharan Africa and Eastern Asia with about 20 per 100,000 individuals and the lowest in North America, South America, Northern Europe, and Oceania (5.0 per 100,000 individuals). Italy and other Southern European countries such as Spain and Greece show mid-incidence levels (12.0 per 100,000 individuals) [1, 2, 3]. Given an incidence rate higher than 1.5% year in at-risk population, such as cirrhotic patients, surveillance programs have a positive cost-benefit ratio because diagnosis in early stage may significantly improve the management of HCC [4]. Ultrasonography (US) is the imaging technique used for surveillance because of its effectiveness in HCC detection despite the limitations due to the operators’ expertise [5]. In the past alpha-fetoprotein (AFP) was combined to US, but at present it is not any more recommended by European and American guidelines [4, 6] because of a suboptimal diagnostic performance of serum biomarkers of HCC in clinical practice [7, 8, 9]. AFP shows highly variable rates of both sensitivity (ranging from 50–70%) and specificity (45–85%) because its serum levels are influenced by liver regeneration following necrosis and inflammation [10, 11]. On the other hand the diagnostic performance of protein induced by vitamin-K absence/antagonist-II [PIVKA-II, also known as des-gamma-carboxyprothrombin (DCP)], a marker of oncogenic mechanisms associated with neovascularization [12, 13, 14], was evaluated almost exclusively in patients with hepatitis C virus (HCV) infection [15]. At present the combination of AFP and PIVKA-II biomarkers for HCC diagnosis is proposed only in Japan [16] where most of HCC cases occur in HCV infected patients [17]. Therefore, several factors depending on liver disease etiology, disease activity and liver regeneration could be responsible for the variability of the results because of the heterogeneity of the studied populations. The importance of such confounding factors could become even more relevant nowadays after the introduction of highly effective antiviral treatment for chronic hepatitis B and C patients [18, 19, 20, 21]. We studied the impact of etiology and activity of chronic liver disease in the diagnostic performance of AFP and PIVKA-II in cirrhotic patients with and without HCC.
Patients and methods
Patients
We studied retrospectively 388 consecutive patients with liver cirrhosis, enrolled in three Italian Hepatology centres [163 (42.0%) in Padua, 180 (46.4%) in Pisa, 45 (11.6%) in Turin]: 1) 258 cirrhotic patients with HCC (diagnosis performed from 2010 to 2015), for whom a serum sample at the time of diagnosis was available; 2) 130 cirrhotic patients on ultrasound (US) surveillance for at least 12 months, without evidence of HCC and with a serum sample available at the beginning of their follow-up. Liver cirrhosis was diagnosed by clinical, biochemical and imaging data (presence of US signs and transient elastography 13 kPa) or liver biopsy: all the patients underwent every 6 month US surveillance during a median follow-up of 25.2 months (range 12.0–67.2). HCC diagnosis and staging were performed according to EASL guidelines and BCLC classification [6, 22]. The underlying CLD was classified in three different groups by etiology: i) Chronic Hepatitis B (CHB), HBsAg positive; ii) Chronic Hepatitis C (CHC), anti-HCV/HCV-RNA positive; iii) Non-Viral CLD, HBsAg and anti-HCV negative. The study was approved by the local Ethical Committee and fulfilled the guidelines of the Declaration of Helsinki (7th revision, 2013). All patients gave their written informed consent.
Serological assays
Quantitative measurements of AFP and PIVKA-II were performed on sera stored at 20C since they were obtained at the time of diagnosis in 258 HCC patients or at a single point evaluation in 130 cirrhotic patients without HCC during their surveillance follow-up. AFP and PIVKA-II serum levels were measured using fully automated chemiluminescent enzyme immunoassays (CLEIA) on Lumipulse G1200 (Fujirebio Inc, Tokyo, Japan). The analytical sensitivity was 0.8 ng/mL for AFP and 1.37 mAU/mL for PIVKA-II. The dynamic range of quantification was 0.8–22,451 ng/mL for AFP and 1.37–75,000 mAU/mL for PIVKA-II and their upper limit of normality were 7.4 ng/mL and 48 mAU/mL respectively. Samples with results exceeding the dynamic range were retested following appropriate dilutions. Tests were performed in a single run at a single reference laboratory according to the manufacturer’s instruction.
Statistical analysis
Quantitative variables were expressed as median and ranges. Differences between the groups of etiology were analysed using Mann-Whitney or Kruskal-Wallis tests and corrected Chi-square test for continuous and categorical variables respectively. Multivariate analysis was performed by logistic regression. The correlations between biomarkers and with ALT levels and tumour size (in HCC patients) were performed with nonparametric Spearman rank test. Receiver operating characteristic (ROC) curves were plotted for each assay in the overall population and according to the etiology of CLD. Areas under ROC curves (AUROC) were evaluated and compared by using MedCalc for Windows, version 15.0 (MedCalc Software, Ostend, Belgium). Diagnostic performances of AFP, PIVKA-II and their combination were determined by calculating sensitivity (Se), specificity (Sp), positive predictive value (PPV), negative predictive value (NPV) and diagnostic accuracy (DA), using several fixed cut-off values, both overall and according to the etiology of CLD. The thresholds used as cut-offs were arbitrarily chosen in accordance to previous studies [23, 24, 25, 26]: 10–20–100 and 400 ng/mL for AFP and 40–48–70 and 150 mAU/mL for PIVKA-II. values 0.05 were considered as significant. All statistical analyses were performed by SPSS (version 20.0, SPSS Inc., Chicago, IL, USA).
Characteristics of the cirrhotic patients without or with hepatocellular carcinoma
Variables
Univariate
Multivariate Analysis
Overall 388
Non-HCC 130
HCC 258
OR
95% CI
Sex
Male Female
(%)
308 (79.4) 80 (20.6)
104 (80.0) 26 (20.0)
204 (79.1) 54 (20.9)
0.471
Age (years)
Median (range)
65.0 (33.8–87.9)
60.6 (33.8–85.3)
66.9 (37.2–87.9)
0.001
1.047
1.019
1.075
0.001
Etiology CHBCHC Non-Viral
(%)
83 (21.4) 182 (46.9) 123 (31.7)
35 (26.9) 56 (43.1) 39 (30.0)
48 (18.6) 126 (48.8) 84 (32.6)
0.166
ALT (U/L)
Median (range)
39 (9–480)
36 (9–312)
41 (9–480)
0.299
Total Bilirubin (mg/dL)
Median (range)
0.82 (0.32–4.87)
0.82 (0.32–4.87)
0.83 (0.32–4.42)
0.355
Platelets ( 10/L)
Median (range)
115 (37–626)
124.5 (37–295)
112 (38–626)
0.182
AFP (ng/mL)
Median (range)
8.6 (1.1–1,366,736)
5.2 (1.4–255.2)
11.4 (1.1–1,366,736)
0.001
2.656
1.612
4.376
0.001
PIVKA-II (mAU/mL)
Median (range)
68 (5–181,690)
34 (5–68,989)
150.5 (7–181,690)
0.001
3.308
1.994
5.487
0.001
BCLC staging
(%)
56 (21.7) 141 (54.7) 37 (14.3) 24 (9.3) 0
ALT, alanine aminotransferase; AFP, alpha-fetoprotein; BCLC, Barcelona clinic liver cancer; CHB, chronic hepatitis B; CHC, chronic hepatitis C; HCC, hepatocellular carcinoma; PIVKA-II, protein induced by vitamin-K absence/antagonist-II. and were included in multivariate analysis after logarithmic transformation.
Changes in biomarkers’ serum levels according absence or presence of HCC and etiology
Biomarker
ULN
Etiology
Non-HCC
HCC
P
AFP
7.4 ng/mL
CHB
2.8
(1.4–14.0)
6.4
(1.2–1,366,736.0)
0.001
CHC
11.2
(3.0–255.2)
20.3
(2.1–81,123.4)
0.005
Non-viral
4.2
(1.6–12.9)
7.5
(1.1–10,525.0)
0.028
PIVKA-II
48 mAU/mL
CHB
32.0
(2.0–60,989.0)
85.0
(21.0–73,068.0)
0.001
CHC
35.0
(10.0–22,515.0)
137.5
(7.0–96,463.0)
0.001
Non-viral
35.0
(8.0–1,224.0)
266.0
(8.0–181,690.0)
0.001
AFP, alpha-fetoprotein; CHB, chronic hepatitis B; CHC, chronic hepatitis C; PIVKA-II, protein induced by vitamin-K absence/antagonist-II; ULN, upper limit of normal.
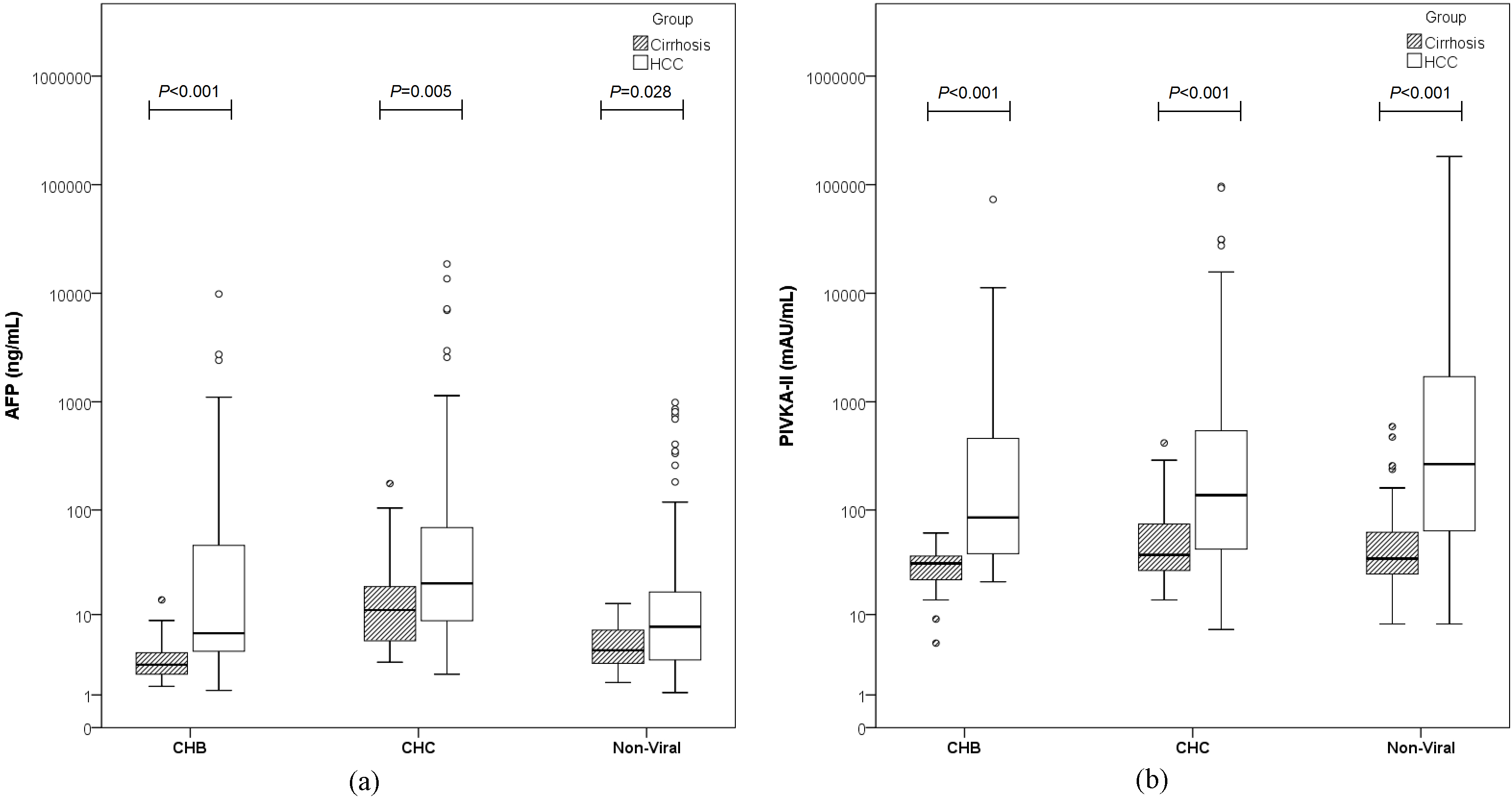
AFP (a) and PIVKA-II (b) in cirrhotic patients with and without HCC with different (CHB, CHC or Non-Viral) etiology of CLD. AFP in patients with cirrhosis: the analysis of the three groups together (Kruskal-Wallis test) shows 0.001. The analysis of two groups at a time (Mann-Whitney Test) shows 0.001 for CHB vs CHC; 0.004 for CHB vs Non-Viral; 0.001 for CHC vs Non-Viral. PIVKA-II in patients with cirrhosis: the analysis of the three groups together (Kruskal-Wallis test) shows 0.319. The analysis of two groups at a time (Mann-Whitney Test) shows 0.289 for CHB vs CHC; 0.142 for CHB vs Non-Viral; 0.550 for CHC vs Non-Viral. AFP in patients with HCC: the analysis of the three groups together (Kruskal-Wallis test) shows 0.001. The analysis of two groups at a time (Mann-Whitney Test) shows 0.007 for CHB vs CHC; 0.334 for CHB vs Non-Viral; 0.001 for CHC vs Non-Viral. PIVKA-II in patients with HCC: the analysis of the three groups together (Kruskal-Wallis test) shows 0.065. The analysis of two groups at a time (Mann-Whitney Test) shows 0.636 for CHB vs CHC; 0.042 for CHB vs Non-Viral; 0.047 for CHC vs Non-Viral.
Results
Demographic, laboratory and clinical data of the 388 cirrhotic patients (258 with HCC and 130 without HCC) are reported in Table 1. The etiology of CLD was CHB, CHC and Non-Viral CLD in 83 (21.4%), 182 (46.9%) and 123 (31.7%) patients, respectively, Liver disease was alcohol-induced in 63 of the 123 (51.2%) patients with Non-Viral CLD, 56 (45.5%) of them had non-alcoholic steatohepatitis (NASH) and 4 (3.3%) autoimmune hepatitis. HCC was present in 48 of 83 CHB (57.8%), 126 of 182 CHC (69.2%) and 84 of 123 Non-Viral CLD (68.3%) patients. Fifty-seven of 83 (68.7%) CHB patients (27 with and 30 without HCC) were on nucleos(t)ide analogues (NUCs) treatment. Median age was higher in HCC patients than in cirrhotics (66.9 vs 60.6 years, 0.001). ALT levels were not significantly different in patients with or without HCC [41 (9–480) vs 36 (9–312) U/L, 0.299]. Overall, CHC patients showed higher ALT values than CHB and Non-Viral CLD [75 (10–480) vs 26.5 (9–168) and 29 (9–229) U/L, 0.001)]. Median ALT levels of patients with or without HCC were comparable in CHC [78 (10–310) vs 72 (15–480) U/L, 0.343] and Non-Viral CLD [30 (12–229) vs 28 (9–132) U/L, 0.627] groups. On the contrary, in CHB patients, median ALT levels were significantly higher in patients with HCC (27 out of 48 on NUCs) than in those without HCC (30 out of 35 on NUCs) [29.0 (12–168) vs 22.5 (9–153) U/L, 0.032]. In 258 HCC patients the BCLC staging at diagnosis was: 0 in 56 (21.7%), A in 141 (54.7%), B in 37 (14.3%) and C in 24 (9.3%); none of the patients was diagnosed on stage D. According to etiology of CLD the HCC staging in CHB, CHC and Non-Viral patients was: 0 in 13 (27.1%), 37 (29.3%) and 6 (7.1%), A in 23 (47.9%), 77 (61.1%) and 41 (48.8%), B in 5 (10.4%), 5 (4.0%) and 27 (32.1%), C in 7 (14.6%), 7 (5.6%) and 10 (12.0%) ( 0.001) respectively.
AFP and PIVKA-II serum levels according to etiology of CLD
Median serum levels of AFP [8.6 ng/mL (1.1–1,366,736)] and PIVKA-II [68 mAU/mL (5–181,690)] were significantly higher in patients with HCC than in those without HCC ( 0.001 for both groups): 11.4 ng/mL (1.1–1,366,736) and 150.5 mAU/mL (7–181,690) versus 5.2 ng/mL (1.4–255.2) and 34 mAU/mL (5–68,989) respectively. At multivariate logistic regression analysis older age (OR 1.047, 95% CI 1.019–1.075, 0.001), and higher AFP and PIVKA-II levels (OR 2.656, 95% CI 1.612–4.376, 0.001, and OR 3.308 95% CI 1.994–5.487, 0.001, respectively) were independently associated with HCC (Table 1). The difference of median AFP and PIVKA-II levels between patients with and without HCC remained statistically significant after stratification by CLD etiology (Table 2 and Fig. 1). AFP median levels were similar in CHB and Non-Viral HCC patients [6.5 ng/mL (1.2–1,366,736) and 7.5 ng/mL (1.1–10,525), respectively, 0.334], but higher in CHC [20.3 ng/mL (2.1–81,123.4), 0.007 vs CHB and 0.001 vs Non-Viral]. In cirrhotics without HCC, AFP levels significantly differed among CHB [2.8 ng/mL (1.4–14.0)], CHC [11.2 ng/mL (3.0–255.2)] and Non-Viral [4.2 ng/mL (1.6–12.9)] groups (CHC vs CHB, 0.001; CHC vs Non-Viral, 0.001; CHB vs Non-Viral, 0.004). PIVKA-II median levels in HCC patients were similar in CHB [85 mAU/mL (21–73,068)] and CHC groups [137.5 mAU/mL (7–96,463)] ( 0.636), but significantly higher in the Non-Viral CLD group [266 mAU/mL (8–181,690)] ( 0.042 vs CHB and 0.047 vs CHC). In patients without HCC PIVKA-II levels were comparable in all CLD groups: 32 mAU/mL (5–68,989), 35 mAU/mL (10–22,515) and 35 mAU/mL (8–1,224) in CHB, CHC, and Non-Viral CLD, respectively (CHC vs CHB, 0.289; CHC vs Non-Viral, 0.550; CHB vs Non-Viral CLD, 0.142).
AFP and PIVKA-II correlations and diagnostic performance
AFP and PIVKA-II levels correlated with each other significantly, but the was low both overall ( 0.355, 0.001) and in the subgroups, namely in patients with and without HCC: 0.281, 0.001 and 0.255, 0.006, respectively. The statistical correlation was maintained when considering each etiologic group, with higher in Non-Viral CLD ( 0.491, 0.001) and CHB ( 0.432, 0.001) as compared to CHC ( 0.254, 0.001). In the sub-analysis where the correlation between the two biomarkers was analysed in each etiology group according to presence or absence of HCC, AFP and PIVKA-II were significantly correlated in HCC patients with viral infection ( 0.416, 0.005 in CHB and 0.218, 0.019 in CHC), but not in cirrhotics without HCC (0.216, 0.220 in CHB and 0.228, 0.133 in CHC). In Non-Viral CLD group a significant correlation between AFP and PIVKA-II was found both in HCC ( 0.423, 0.001) and non-HCC patients ( 0.562, 0.001). AFP and ALT correlated significantly in HCC patients with CHC and Non-Viral CLD ( 0.463, 0.001 and 0.359, 0.047, respectively), but not in CHB patients ( 0.175, 0.354). On the contrary, in cirrhotics without HCC, the correlation was found in CHB patients only ( 0.601, 0.002). PIVKA-II and ALT correlated significantly in HCC patients with Non-Viral CLD only ( 0.595, 0.001); whereas no correlation was observed in HCC patients with viral infection ( 0.179, 0.344 in CHB and 0.194, 0.191 in CHC) or in cirrhotic patients without HCC ( 0.156, 0.477 in CHB; 0.298, 0.124 in CHC and 0.193, 0.647 in Non-Viral). AFP levels correlated with tumour size in CHB patients only ( 0.419; 0.007). PIVKA-II showed a significant correlation with tumour size independently of etiology, with higher in CHB and Non-Viral ( 0.552; 0.001 and 0.542, 0.001, respectively) as compared to CHC patients ( 0.436; 0.001).
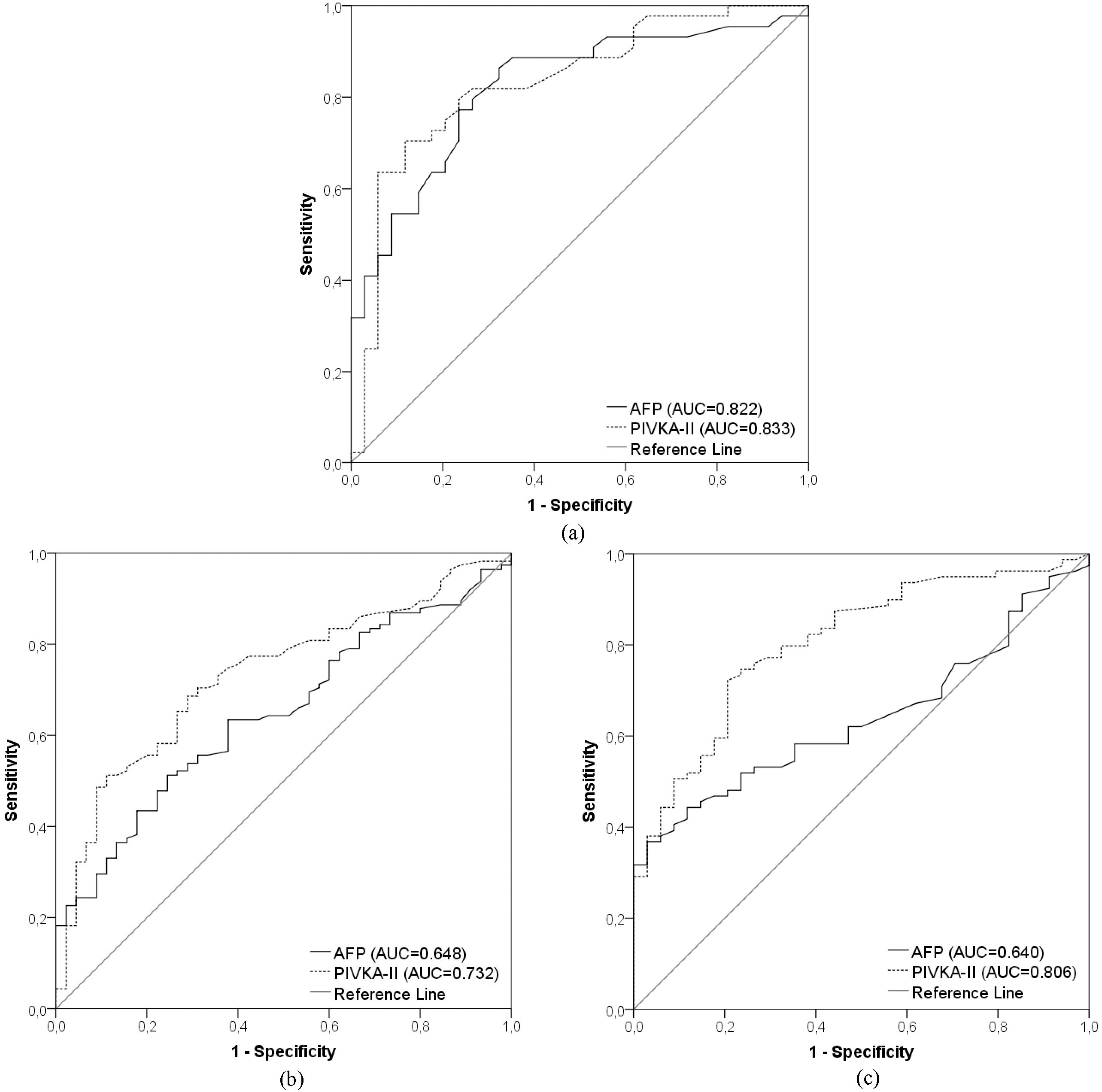
Receiver operating characteristic curves of AFP and PIVKA-II according to CLD etiology. The best performances of the two biomarkers in differentiating HCC from Cirrhosis are obtained in the CHB group (a). In CHC (b) and Non-Viral (c) groups it is evident a progressive loss of performance of AFP. PIVKA-II maintains higher values of AUCs (Area under curve) than AFP in all the three groups of etiology.
Diagnostic performances of AFP and PIVKA-II overall and according etiology
AFP
PIVKA-II
AFP PIVKA-II
10
20
100
400
40
48
70
150
10
20
100
400
40
48
70
150
Overall
Sensitivity
52.5
38.2
21.0
12.2
78.7
74.0
64.7
50.0
87.4
80.7
68.5
51.7
Specificity
75.2
90.3
98.2
100
62.5
70.8
80.0
90.0
52.2
67.3
78.8
89.4
PPV
81.7
89.2
96.2
100
81.9
84.5
87.4
91.5
79.4
83.8
87.2
91.1
NPV
42.9
41.0
37.1
35.1
57.7
55.9
51.3
45.6
66.3
62.3
54.3
46.8
DA
59.8
55.0
45.9
40.5
73.5
73.0
69.6
62.7
76.1
76.4
71.8
63.8
CHB
Sensitivity
36.4
29.5
20.5
18.2
75.0
68.8
58.3
39.6
79.5
72.7
63.6
43.2
Specificity
97.1
100
100
100
76.5
85.3
94.1
94.1
73.5
85.3
94.1
94.1
PPV
94.1
100
100
100
81.8
86.8
93.3
90.5
79.5
86.5
93.3
90.5
NPV
54.1
52.3
49.3
48.6
68.4
65.9
61.5
52.5
73.5
70.7
66.7
56.1
DA
62.8
60.3
55.1
53.8
75.6
75.6
73.2
62.2
76.9
78.2
76.9
65.4
CHC
Sensitivity
69.6
51.3
23.5
11.3
76.2
71.4
60.3
49.2
91.3
81.7
64.3
49.6
Specificity
44.4
75.6
95.6
100
57.1
69.4
73.5
91.8
33.3
57.8
71.1
91.1
PPV
76.2
84.3
93.1
100
82.1
85.7
85.4
93.9
77.8
83.2
85.1
93.4
NPV
36.4
37.8
32.8
30.6
48.3
48.6
41.9
41.3
60.0
55.3
43.8
41.4
DA
62.5
58.1
43.8
36.3
70.9
70.9
64.0
61.1
75.0
75.0
66.3
61.3
Non-Viral
Sensitivity
36.7
24.1
17.7
10.1
84.5
81.0
73.8
57.1
86.1
83.5
77.2
59.5
Specificity
94.1
100
100
100
56.8
59.5
75.7
83.8
55.9
61.8
73.5
82.4
PPV
93.5
100
100
100
81.6
81.9
87.3
88.9
81.9
83.5
87.1
88.7
NPV
39.0
36.2
34.3
32.4
61.8
57.9
56.0
46.3
63.3
61.8
58.1
46.7
DA
54.0
46.9
42.5
37.2
76.0
74.4
74.4
65.3
77.0
77.0
76.1
66.4
AFP, alpha-fetoprotein; CHB, chronic hepatitis B; CHC, chronic hepatitis C; DA, diagnostic accuracy; NPV, negative predictive value; PIVKA-II, protein induced by vitamin-K absence/antagonist-II; PPV, positive predictive value.
The ROC curves of AFP and PIVKA-II for the whole cohort were 0.698 (95% CI 0.642–0.753, 0.001) and 0.780 (95% CI 0.730–0.831, 0.001), respectively. The diagnostic performances of the two biomarkers were evaluated using fixed cut-off values: the thresholds with the best performance were 10 ng/mL for AFP (Se 52.5%, Sp 75.2%, PPV 81.7%, NPV 42.9%, and DA 59.8%) and 40 mAU/mL for PIVKA-II (Se 78.7%, Sp 62.5%, PPV 81.9%, NPV 57.7%, DA 73.5%). When the ROC curves were plotted according to CLD etiology, the highest AUROCs were obtained for both PIVKA-II and AFP in CHB group. AFP showed a progressive loss of diagnostic performance compared to PIVKA-II in CHC and Non-Viral CLD patients: AUROC (95% CI) AFP/PIVKA-II 0.822 (0.728–0.915)/0.833 (0.739–0.926) in CHB; 0.648 (0.560–0.736)/0.732 (0.650–0.814) in CHC; 0.640 (0.540–0.740)/0.806 (0.722–0.889) in Non-Viral CLD (Fig. 2). Then, we evaluated the diagnostic performances of the two biomarkers, alone or in combination, in each group of etiology using different cut-off values (Table 3). In CHB and Non-Viral CLD patients AFP resulted highly specific for HCC even at low cut-off values (100% Specificity at the threshold of 20 ng/mL), but with poor Sensitivity (29.5% and 24.1%). In CHC patients 100% Specificity was achieved at 400 ng/mL cut-off with 11.3% Sensitivity. Overall the diagnostic performance of PIVKA-II was higher than that of AFP: PIVKA-II diagnostic accuracies ranged between 62.7 to 73.5% as compared to 40.5 to 59.8% for AFP. The same hold true when each etiologic group was considered. The best DA was obtained combining the two biomarkers and considering as positive AFP 20 ng/mL or PIVKA-II 48 mAU/mL: 78.2% for CHB (Se 72.7%, Sp 85.3%), 77% for Non-Viral CLD (Se 83.5%, Sp 61.8%) and 75% for CHC (Se 81.7%, Sp 57.8%) (Table 3).
Discussion
In a cohort of 388 consecutive patients with liver cirrhosis with and without HCC we studied the impact of the etiology of the underlying CLD as confounding factor influencing the diagnostic performance of AFP and PIVKA-II as HCC biomarkers. AFP and PIVKA-II serum levels were confirmed to be higher in HCC than non-HCC patients independently of CLD etiology. Overall there was a significant correlation between the two biomarkers, but with low value. In cirrhotic patients without HCC, AFP levels differed significantly according to etiology and were higher in patients with CHC and Non-Viral CLD than in CHB (CHC vs CHB, 0.001; CHC vs Non-Viral, 0.001; CHB vs Non-Viral, 0.004). Since all the patients with CHC had an active liver disease whereas the majority (68.7%) of CHB patients were treated with nucleos(t)ide analogue and had normal ALT, these results are consistent with the evidence that AFP serum levels are influenced significantly by hepatocyte regeneration, triggered by necro-inflammation in patients with active chronic liver disease [27]. In the same way AFP serum levels were higher in CHC than in CHB and Non-Viral CLD ( 0.007 vs CHB and 0.001 vs Non-Viral CLD) in patients with HCC. About a half of HCC in CHB cirrhotic patients (27 out of 48, 56.3%) occurred in treated patients with normal ALT. At variance with AFP, PIVKA-II serum levels are not influenced by liver regeneration since PIVKA-II is a prothrombin precursor without coagulation activity which increases following an impaired vitamin-K-dependent post-transcriptional carboxylation of glutamic acid residues at the N-terminus in the HCC cells only [28]. Consistently we did not find any significant difference between PIVKA-II levels in patients with CLD of different etiology and/or correlation with ALT levels. On the other hand we found a highly significant correlation ( 0.001) between PIVKA-II and HCC size in all the etiology groups in accordance with the specific association of this biomarker with tumour angiogenesis. PIVKA-II serum levels were positively correlated with tumour vascularization and PIVKA-II was shown to stimulate the growth and migration of endothelial cells by activating the vascular endothelial cell receptor-2 (VEGFR-2) acting as a paracrine pro-angiogenetic factor [13, 14, 29]. Interestingly PIVKA-II levels were significantly higher in Non-Viral HCC patients ( 0.042 vs CHB and 0.047 vs CHC) (Fig. 1). These findings could stem from a different pathogenic pathway of hepato-carcinogenesis in this subset of CLD. Alternatively, higher PIVKA-II median levels could be explained by the presence of a more advanced neoplastic disease (as suggested by the BCLC stage at diagnosis) in Non-Viral HCC patients as compared to CHB and CHC patients who are usually followed-up by more stringent US surveillance. AFP levels did not correlate with tumour size in patients with elevated ALT, possibly because of a confounding fraction of the biomarker released by regenerating hepatocytes. Consistently, a correlation between AFP levels and HCC size was present only in absence of liver necro-inflammation, namely in treated CHB patients with normal ALT levels. The finding that both HCC biomarkers and age were the only variables independently associated with HCC at multivariate analysis further supports the potential role of these two biomarkers for the HCC surveillance in high risk populations. However, because of the widely variable diagnostic performances of AFP and PIVKA-II in different cohorts, the combined use of these biomarkers did not find yet a homogeneous application in international guidelines. Some investigators reported the superiority of AFP compared to other biomarkers [15, 30] whereas a meta-analysis of forty-nine studies indicated PIVKA-II as the best single marker for HCC even in presence of a significant heterogeneity of sensitivity and specificity rates [31]. Major differences of the study populations in clinical (age distribution, CLD etiology, disease activity, race, tumour stage) and methodological determinants (type of study, assay characteristics, cut-off values, reference standards) are the more reasonable explanations of these discrepancies. Accordingly, two recent Italian studies analysed the diagnostic performance of AFP and PIVKA-II reporting different results: Se/Sp 81.1%/86.4% vs 55.0%/55.0% for AFP and 77.8%/90.9% vs 60.0%/90.0% for PIVKA-II. However, these studies used different assays and cut-offs (AFP 5.3 ng/ml; PIVKA-II 0.4 ng/ml and AFP 20 ng/mL; PIVKA-II 47 mAU/mL, respectively) and the percentage of cirrhotics in the non-HCC group was relatively low [26, 32]. In our study we report the diagnostic performances of the two biomarkers using different cut-offs defined by previous studies [23, 24, 25, 26]. Our results confirm that PIVKA-II is a better marker than AFP in differentiating HCC from non-HCC cirrhotic patients, although there are significant differences according to the etiology of the underlying CLD. Specifically, AUROC values of PIVKA-II and AFP are similar in CHB patients (0.833 and 0.822), but different in CHC (0.732 and 0.648) and Non-Viral CLD (0.806 and 0.640) (Fig. 2). These findings agree with previous observations suggesting a better AFP diagnostic performance in HBV-infected patients undergoing antiviral therapy [33] where the prolonged remission of necro-inflammation reduces the confounding fraction of AFP generated by liver regeneration which is enhanced in active liver disease. The significant impact of CLD etiology on the diagnostic performance of AFP and PIVKA-II and the changing epidemiologic patterns of CLD in different areas of the world explain why the combined use of AFP and PIVKA-II has become a routine diagnostic tool since many years in some countries, such as Japan where HCV infection was the prevalent cause of CLD [17]. In Italy HCV infection prevailed in HCC patients during the last decades, whereas a significant increase of Non-Viral CLD is reported in more recent years [3]. Our results support the utility of combining AFP and PIVKA-II with the highest gain in diagnostic accuracy was observed in CHC patients. Major limitations of our study are the retrospective design and the sample size which do not allow to validate new cut-off values. Nevertheless, we could confirm the relevant impact of the etiology of CLD and disease activity on the diagnostic performance of AFP and PIVKA-II. Accordingly, these co-factors should be taken into account for the definition of the clinically meaningful cut-offs since the use of the same threshold in each group of etiology provides widely different sensitivity, specificity and diagnostic accuracies rates. Another limitation of the study is represented by the etiology ratio that could not be precisely balanced and specifically the number of CHB non-HCC patients was higher (26.9%) than CHB HCC patients (18.6%). Furthermore we could not perform any evaluation in order to assess the cost-effectiveness of these biomarkers for HCC surveillance. Finally we did not completely rule out possible interferences on PIVKA-II serum levels by alcohol intake and vitamin-K deficiency or Warfarin therapies. Future studies should take into account the variability due to the aforementioned confounding factors, together with the individual biological variability which is inherently associated to each biomarker. Therefore, an important step ahead to ameliorate the diagnostic performance of the combined used of AFP and PIVKA-II would be the definition of the biologically meaningful delta variation of the individual baseline level of the two biomarkers in consecutive serum specimens collected prospectively from patients at the same risk of developing HCC.
In conclusion, the overall results of our study show that the diagnostic performance of AFP and PIVKA-II as HCC biomarkers is significantly influenced by the etiology of CLD and provide a consistent rationale for using the combination of AFP and PIVKA-II for HCC diagnosis in clinical practice, particularly in the subgroups of HCV infected and Non-Viral CLD patients. Moreover, these results suggest that the optimization of the two biomarkers cut-offs according to the etiology and activity of CLD (absence of active liver disease, sustained virologic response in both HBV, HCV and HDV infections) represents an important goal of future prospective studies.
Footnotes
Acknowledgments
We thank Fujirebio Inc, Tokyo, Japan for the supply of AFP and PIVKA-II kits without any interference with the design and conduct of the study.
Conflict of interest
None.
References
1.
BoschF.X.RibesJ.DìazM. and ClériesR., Primary liver cancer worldwide incidence and trends, Gastroenterology127 (2004), S5–S16.
2.
El-SeragH.B., Epidemiology of viral hepatitis and hepatocellular carcinoma, Gastroenterology142(6) (2012), 1264–1273.
3.
StroffoliniT.TrevisaniF.PinzelloG.BrunelloF.TommasiniM.A.IavaroneM.Di MarcoV.FarinatiF.Del PoggioP.BorzioF.BorzioM.CaturelliE.Di NolfoM.A.FrigerioM.BrancaccioG. and GaetaG.B., Changing aetiological factors of hepatocellular carcinoma and their potential impact on the effectiveness of surveillance, Dig Liver Dis43(11) (2011), 875–880.
4.
BruixJ. and ShermanM., American Association for the Study of Liver Diseases, Management of Hepatocellular Carcinoma: an update, Hepatology53(3) (2011), 1020–1022.
5.
SingalA.VolkM.L.WaljeeA.SalgiaR.HigginsP.RogersM.A. and MarreroJ.A., Meta-analysis: surveillance with ultrasound for early-stage hepatocellular carcinoma in patients with cirrhosis, Aliment Pharmacol Ther30 (2009), 30–47.
6.
European Association For The Study Of The Liver; European Organisation For Research And Treatment Of Cancer. EASL-EORTC clinical practice guidelines: management of hepatocellular carcinoma, J Hepatol56 (2012), 908–943.
7.
SongP.TobeR.G.InagakiY.KokudoN.HasegawaK.SugawaraY. and TangW., The management of hepatocellular carcinoma around the world: a comparison of guidelines from 2001 to 2011, Liver Int32 (2012), 1053–1063.
8.
LokA.S.SterlingR.K.EverhartJ.E.WrightE.C.HoefsJ.C.Di BisceglieA.M.MorganT.R.KimH.YLeeW.M.BonkovskyH.L.DienstagJ.L., HALT-C Trial Group, Des-gamma-carboxy prothrombin and alpha-fetoprotein as biomarkers for the early detection of hepatocellular carcinoma, Gastroenterology138 (2010), 493–502.
9.
HuoT.I.HsiaC.Y.ChuC.J.HuangY.H.LuiW.Y.WuJ.C.LeeP.C.ChiC.W. and LeeS.D., The predictive ability of serum alpha-fetoprotein for hepatocellular carcinoma is linked with the characteristics of the target population at surveillance, Journal of Surgical Oncology95 (2007), 645–651.
10.
Di BisceglieA.M.SterlingR.K.ChungR.T.EverhartJ.E.DienstagJ.L.BonkovskyH.L.WrightE.C.EversonG.T.LindsayK.L.LokA.S.LeeW.M.MorganT.R.GhanyM.G.GretchD.R., HALT-C Trial Group, Serum alpha-fetoprotein levels in patients with advanced hepatitis C: results from the HALT-C Trial, J Hepatol43(3) (2005), 434–441.
11.
GopalP.YoppA.C.WaljeeA.K.ChiangJ.NehraM.KandunooriP. and SingalA.G., Factors that affect accuracy of a-Fetoprotein Test in Detection of Hepatocellular Carcinoma in Patients with Cirrhosis, Clin Gastroenterol Hepatol12(5) (2014), 870–877.
12.
LiebmanH.A.FurieB.C.TongM.J.BlanchardR.A.LoK.J.LeeS.D.ColemanM.S. and FurieB., Des-gamma-carboxy (abnormal) prothrombin as a serum marker of primary hepatocellular carcinoma, N Engl J Med310 (1984), 1427–1431.
13.
TamanoM.SugayaH.OgumaM.IijimaM.YonedaM.MurohisaT.KojimaK.KuniyoshiT.MajimaY.HashimotoT. and TeranoA., Serum and tissue PIVKA-II expression reflect the biological malignant potential of small hepatocellular carcinoma, Hepatol. Res22 (2002), 261–269.
14.
FujikawaT.ShiraraH.UedaN.TakaokaN.NakanishiY.MatsuoN.TanakaS.NishinaS.SuzukiM.TakakiA.SakaguchiK. and ShiratoriY., Des-gamma-carboxyl prothromobin-promoted Vascular Endothelial Cell Proliferation and Migration, J Biol Chem282 (2007), 8741–8748.
15.
MarreroJ.A.FengZ.WangY.NguyenM.H.BefelerA.S.RobertsL.R.ReddyK.R.HarnoisD.LlovetJ.M.NormolleD.DalhgrenJ.ChiaD.LokA.S.WagnerP.D.SrivastavaS. and SchwartzM., Alpha-fetoprotein, Des-gamma Carboxyprothrombin, and Lectin-Bound Alpha-fetoprotein in Early Hepatocellular Carcinoma, Gastroenterology137(1) (2009), 110–118.
16.
KudoM.MatsuiO.IzumiN.IijimaH.KadoyaM.ImaiY.OkusakaT.MiyayamaS.TsuchiyaK.UeshimaK.HiraokaA.IkedaM.OgasawaraS.YamashitaT.MinamiT.YamakadoK., Liver Cancer Study Group of Japan, JSH Consensus-Based Clinical Practice Guidelines for the Management of Hepatocellular Carcinoma: 2014 Update by the Liver Cancer Study Group of Japan, Liver Cancer3(3–4) (2014), 458–468.
17.
ZhuR.X.SetoW.K.LaiC.L. and YuenM.F., Epidemiology of Hepatocellular Carcinoma in the Asia-Pacific Region, Gut Liver10(3) (2016), 332–339.
18.
ChenL.P.ZhaoJ.DuY.HanY.F.SuT.ZhangH.W. and CaoG.W., Antiviral treatment to prevent chronic hepatitis B or C-related hepatocellular carcinoma, World J Virol1(6) (2012), 174–183.
19.
LaiC.L. and YuenM.F., Prevention of Hepatitis B Virus-Related Hepatocellular Carcinoma With Antiviral Therapy, Hepatology57 (2013), 399–408.
20.
El-SeragH.B.KanwalF.RichardsonP. and KramerJ., Risk of hepatocellular carcinoma after sustained virologic response in Veterans with hepatitis C virus infection, Hepatology64(1) (2016), 130–137.
21.
WirthT.C. and MannsM.P., The impact of the revolution in hepatitis C treatment on hepatocellular carcinoma, Ann Oncol27(8) (2016), 1467–1474.
22.
LlovetJ.M.BrúC. and BruixJ., Prognosis of hepatocellular carcinoma: the BCLC staging classification, Semin Liver Dis19(3) (1999), 329–338.
23.
VolkM.L.HernandezJ.C.SuG.L.LokA.S. and MarreroJ.A., Risk factors for hepatocellular carcinoma may impair the performance of biomarkers: a comparison of AFP, DCP, and AFP-L3, Cancer Biomarkers3 (2007), 79–87.
24.
LimT.S.KimD.Y.HanK.H.KimH.S.ShinS.H.JungK.S.KimB.K.KimS.U.ParkJ.Y. and AhnS.H., Combined use of AFP, PIVKA-II, and AFP-L3 as tumor markers enhances diagnostic accuracy for hepatocellular carcinoma in cirrhotic patients, Scand J Gastroenterol51(3) (2016), 344–353.
25.
SeoS.I.KimH.S.KimW.J.ShinW.G.KimD.J.KimK.H.JangM.K.LeeJ.H.KimJ.S.KimH.Y.KimD.J.LeeM.S. and ParkC.K., Diagnostic value of PIVKA-II and alpha-fetoprotein in hepatitis B virus-associated hepatocellular carcinoma, World J Gastroenterol21(13) (2015), 3928–3935.
26.
ViggianiV.PalombiS.GennariniG.D’EttorreG.De VitoC.AngeloniA.FratiL. and AnastasiE., Protein Induced by vitamin K absence or antagonist-II (PIVKA-II) specifically increased in italian hepatocellular carcinoma patients, Scand J Gastroenterol51(10) (2016), 1257–1262.
27.
KuhlmannW.D. and PeschkeP., Hepatic progenitor cells, stem cells, and AFP expression in models of liver injury, Int J Exp Pathol87(5) (2006), 343–359.
28.
UeharaS.GotohK.HandaH.HonjoK. and HirayamaA., Process of carboxylation of glutamic acid residues in the gla domain of human des-gamma-carboxyprothrombin, Clin Chim Acta289 (1999), 33–44.
29.
MatsubaraM.ShirahaH.KataokaJ.IwamuroM.HoriguchiS.NishinaS.TakaokaN.UemuraM.TakakiA.NakamuraS.KobayashiY.NousoK. and YamamotoK., Des-gamma-carboxyl prothrombin is associated with tumor angiogensis in hepatocellular carcinoma, J Gastroenterol Hepatol27(10) (2012), 1602–1608.
30.
JangE.S.JeongS.H.KimJ.W.ChoiY.S.LeissnerP. and BrechotC., Diagnostic Performance of Alpha-fetoprotein, Protein Induced by Vitamin K Absence, Osteopontin, Dickkopf-1 and Its Combinations for Hepatocellular Carcinoma, PloS ONE11(3) (2016), e0151069.
31.
LiC.ZhangZ.ZhangP. and LiuJ., Diagnostic accuracy of des-gamma-carboxy prothrombin versus alpha-fetoprotein for hepatocellular carcinoma: A systematic review, Hepatol Res44(10) (2014), E11–25.
32.
CavigliaG.P.AbateM.L.PetriniE.GaiaS.RizzettoM. and SmedileA., Highly sensitive alpha-fetoprotein, Lens culinaris agglutinin-reactive fraction fo alpha-fetoprotein and des-gamma-carboxyprothrombin for hepatocellular carcinoma detection, Hepatol Res46(3) (2016), E130–5.
33.
KimG.A.SeockC.H.ParkJ.W.AnJ.LeeK.S.YangJ.E.LimY.S.KimK.M.ShimJ.H.LeeD. and LeeH.C., Reappraisal of serum alpha-fetoprotein as a surveillance test for hepatocellular carcinoma during entecavir treatment, Liver Int35(1) (2015), 232–239.