
Abstract
Background
Waterpipe smoking (WPS) is a social custom common in many Middle Eastern, North African, and Asian countries and has become increasingly popular in the US, especially among youth; however, WPS smoking may be increasing in the US adult population as well. There is a common belief among waterpipe (WP) smokers that WPS is less harmful than smoking cigarettes. Thus, this review aims to systematically explore the literature on the effects of WP tobacco smoking with a particular focus on cardiovascular and respiratory health outcomes as well as on oxidative stress, immunity, and cell cycle interference health outcomes.
Methodology
We conducted a systematic review, guided by the criteria of The Preferred Reporting Items for Systematic Reviews and Meta-Analyses, using the following online databases MEDLINE, CINAHL, ScienceDirect, PMC, and Cochrane Library. Results were summarized qualitatively.
Results
Forty studies met the inclusion criteria established for this review. Based on the existing evidence, several cardiovascular and respiratory physiologic health indicators and conditions have been shown to be negatively affected by WPS. In addition to the effects of nicotine and chemical toxicant exposures, WPS was significantly associated with an increase in heart rate, blood pressure, and lower pulmonary function test results, as well as a number of health conditions such as lung cancer, alterations in oxidative stress, immunity, and cell cycle interference.
Conclusion
The current literature provides evidence that WPS is associated with a number of negative health indicators and outcomes. There is need for more research related to WPS and its effects on health so that appropriate campaigns and prevention interventions can be implemented to control the epidemic increase of WPS in the US.
Introduction
Waterpipe smoking (WPS), commonly known as hookah smoking, is a growing worldwide social phenomenon practiced in group settings such as hookah bars or cafés in which patrons purchase waterpipe (WP) tobacco and then share it during smoking sessions. WPS is a symbol of social sharing and cultural identity.1–4 The unregulated social aspect of smoking WP, combined with the myth that WPS is less harmful than smoking cigarettes, makes it difficult for those newly exposed to WPS to recognize the potential harmful effects, particularly when evidence is still being established. WPS sessions vary in length, ranging from 30 to 90 minutes,5–7 depending on the number of those sharing or the number of tobacco pouches used during a smoking session. A single WPS session may involve 50 to 100 times the smoke volume inhaled from a single cigarette.8–16 In one study, once-a-day WP smokers were found to have levels of plasma nicotine concentration comparable to those of 10 cigarettes/day smokers,8,17 and evidence suggests that WP use is associated with health risks comparable to those caused due to cigarette smoking. 18 WPS is also associated with nicotine addiction 19 and includes negative health consequences from secondhand smoke exposure. 20
Despite the evidence, most WP users are misinformed about the risks of use. Of particular concern is WP use in the Eastern Mediterranean Region (which includes Middle Eastern and North African countries). Prevalence of WPS in this region is the highest in the world, ranging between 20% and 70%. 6 WPS appears to be on the rise, especially among youth and college-age young adults.9–11,21,22 Research focused on WPS and WP secondhand smoke is garnering attention in the US and across the globe; however, there continues to remain a gap in knowledge about WPS and WP secondhand smoke in the US in comparison to other countries such as those in the Middle East. The World Health Organization's (WHO) report on research for universal health coverage notes that smoking is responsible for about six million deaths annually worldwide; more than five million of these deaths occur in primary smokers, and the remainder die as a result of secondhand smoke exposure.23,24 Despite the remarkable success of public health policies in regulating and reducing cigarette smoking, WPS has been flourishing worldwide, thus emphasizing the importance of strict tobacco control policies and regulations that are also WP oriented. Monitoring and regulating tobacco use should target not only cigarette smoking but also all forms of tobacco in order to combat the worldwide spread of WPS and the misconception that it is less harmful than other forms of tobacco. 18
Two systematic reviews conducted by Akl et al 25 and El-Zaatari et al 26 did an excellent job of summarizing the health effects of WPS on multiple organ systems. The systematic review presented here offers additional evidence by extending the search to include CINAHL, ScienceDirect, PMC, and Cochrane Library databases. Additionally, our systematic review adds five additional studies to the previously published systematic review 26 and includes a comprehensive focus and inclusion of studies reporting cardiovascular and respiratory health outcomes as well as on oxidative stress, immunity, and cell cycle interference health outcomes. This review is important in order to compel evidence about the direct association between cardiovascular, respiratory illness, and WPS. In addition, this review is important to develop scientifically based regulatory policies with regard to WPS and WP secondhand smoke exposure, as tobacco control policy makers need reliable up-to-date scientific evidence to inform concerns aimed at: (1) establishing health warning campaigns and label packaging that identifies the known risks of WPS, (2) prevention of the sale of WP tobacco to minors, and (3) targeting prevention control and taxation similar to those used to combat cigarette smoking.
Thus, the aim of this systematic review was to assess the most up-to-date published literature in order to synthesize the evidence about the effects of WPS and exposure to WP secondhand smoke on health outcomes. The research question was: How does WPS affect the cardiovascular, respiratory, and immunity-related health outcomes of people who smoke waterpipe?
Methodology
Protocol Development
We developed the protocol specifying all aspects of the review methods before commencing the review. These included the following: inclusion criteria for studies, search strategy, screening method, abstraction, quality assessment, and data analysis. This aspect of the design was planned to minimize the effect of our possible bias on the review.
Search Strategy
The review of the literature was conducted between May and August 2015 by searching articles published in English using the following electronic databases: MEDLINE, CINAHL, ScienceDirect, PMC, and Cochrane Library. Our literature search was restricted to articles published between January 1, 2005, and August 31, 2015. Search terms included combinations of the following: “waterpipe,” “water-pipe,” “water pipe,” “hookah,” “shisha,” “narghile,” “narguile,” “hubble bubble,” “goza,” “respiratory system illness,” “cardiovascular diseases,” “health concerns,” “health effects,” “cancer,” and “cardiorespiratory.” We included original research studies conducted inside and outside of the US if published in English.
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines 27 outlined this literature search and review. All of the originally retrieved articles were saved in an EndNote library. Using the EndNote library search box, these articles were screened for duplicates, the search terms, and the word “review” in the title. Articles were deleted from the EndNote library if their titles were duplicates, did not contain the key terms, or had the words “review,” “expert's opinion,” or “qualitative.” Abstracts of the remaining articles were also scanned for the search terms and the words “review,” “expert's opinion,” and “qualitative.” Articles were deleted from the library if their abstracts did not contain the search terms or had the words “review,” “expert's opinion,” and “qualitative.” Abstracts and full texts of the remaining articles were read to check for their relevance to the searched topics. Additional articles were excluded because they were literature reviews. The remaining articles were included in this systematic review.
Data Abstraction
The data abstraction form was piloted over five studies and used to abstract general information about the paper, where the study was conducted, study characteristics, populations studied, design features that affected the quality of the study and the validity of the results, outcome measures, and quality assessment data. Abstraction was performed in duplicate independently. Any disagreement was resolved by discussion.
Data Analysis
Four reviewers extracted data from the papers; two reviewers worked independently on each paper and then amalgamated the results. Discrepancies were resolved by referral back to the original papers and discussion. We did not combine the results of the studies because of the heterogeneity of design, outcomes, and populations. In our narrative analysis, we consider the results in relation to the design and quality of the studies.
Results
Our search of the literature identified 59 potentially relevant articles, but only 40 met the inclusion criteria (Fig. 1). The 40 articles regarding the effects of WPS on health outcomes were thoroughly reviewed. A review across the 40 articles resulted in the effects of WPS being categorized into four areas of focus by health outcome: (1) cardiovascular, (2) respiratory, and (3) oxidative stress, immunity, and cell cycle interference. Research studies involving humans (n = 37/40) were mainly conducted in the Middle East (28/37; 75.7%). Other human research studies were conducted in the US (5/37; 13.5%), the United Kingdom (1/37; 2.7%), the Czech Republic (1/37; 2.7%), China (1/37; 2.7%), and Bangladesh (1/37; 2.7%), and one study was conducted in both the Middle East and North Africa (2.7%). In vitro studies (n = 2) and articles that did not provide information regarding participant age (n = 4) were excluded from calculation of participants’ average age.

Process of the literature search.
Twelve studies used a case–control study design.7,15,28–37 A cross-sectional design (n = 12) was also used in many studies.38–49 Other study designs included a quasi-experimental design (n = 3),50–52 a time series (n = 2),14,53 cohort (n = 2),54,55 single group pretest–postest (n = 2),56,57 experimental (n = 2),58,59 a crossover design (n = 2),60,61 secondary analysis (n = 1), 62 repeated measures (n = 1), 63 and case report (n = 1). 64
Cardiovascular Outcomes
Overview
As seen in Table 1, 15 articles examined cardiovascular outcomes and focused on multiple blood pressure factors such as mean arterial pressure, vascular resistance, systolic and diastolic blood pressure, and mean blood pressure.14,15,26,39,40,50,54 In addition, factors such as heart rate, heart rate variability, and blood flow obstruction were examined.14,15,38,51,54,55,60,61 There was some overlap among studies examining cardiovascular outcomes and respiratory outcomes.39,51,55 Also, other cardiovascular studies included variables such as toxic metals and cancer and overall stroke-related mortalities.28,29,54,62
WPS and cardiovascular effects.
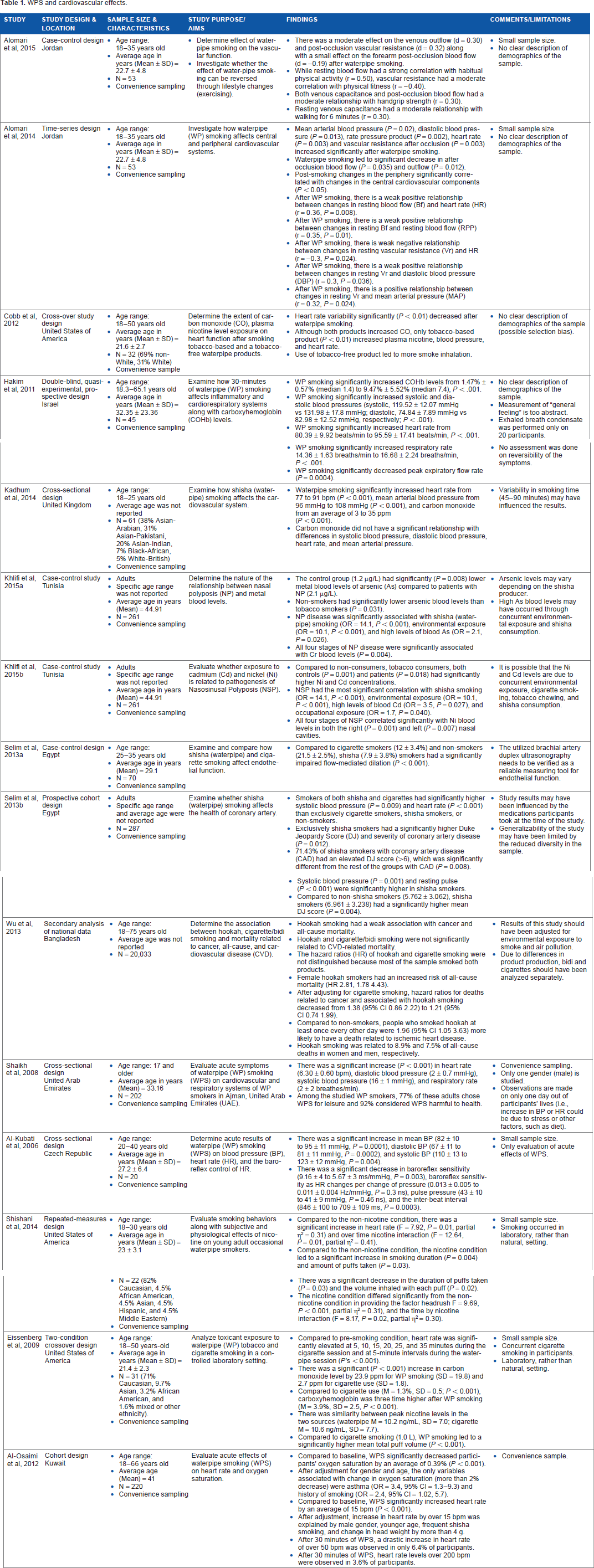
Synthesis of Results
Several cardiovascular outcomes are affected by WPS (Table 1). Vascular resistance demonstrated a significant increase after the use of WPS.14,15 Significant increases were noted among all studies that examined heart rate and systolic, diastolic, and mean blood pressure.38,39,41,47,50,51,54–56,60,61,63 There was a drastic increase in heart rate (50 beats per minute) noted in approximately 10% of participants 30 minutes following WPS in one study. 60 Heart rate variability significantly decreased after WPS. 60
Also noted among WPS users was more severe coronary artery disease compared to nonsmokers and those who only smoked cigarettes. 30 One study found a moderate effect on venous outflow and vascular resistance. 15 Indeed, WPS users were 1.96 times more likely to die from cardiovascular disease than nonsmokers, and WP users had more coronary artery disease than nonsmokers. 62
Respiratory Outcomes
Overview
Twenty-one articles (Table 2) examined respiratory parameters. Nine respiratory studies focused on the effects of WPS on either overall pulmonary function parameters or components of pulmonary function such as forced expiratory volume.32,33,35,42,47,50,52,53,56,65 Nearly half (10 of 21) explored respiratory symptoms (shortness of breath, cough, and wheezing) or diseases (chronic pulmonary obstructive disorder, chronic bronchitis, and asthma).32–34,43–46,49,52,56 Two studies examined lung cancer as an outcome variable of WPS.31,36 One study explored the concept of lung age as a descriptor of WPS use, and one study explored the concept of respiratory quality of life.48,56 Finally, one case study focused on severe carbon monoxide poisoning from smoking WP. 64
WPS and respiratory effects.

Synthesis of Results
There is evidence of the negative effects of WPS on respiratory outcomes (Table 2). Compared to individuals who did not smoke, WPS users had significantly (P < 0.05) lower scores on overall pulmonary function tests (PFTs).16,32,33 The forced expiratory volume significantly (P < 0.001) decreased in individuals in the WPS group compared to non-smokers (P < 0.05) and after WPS use.42,56 Two studies, however, found no difference in forced expiratory volume between WPS and cigarette use, and one study demonstrated a significant (P < 0.05) decrease in forced expiratory volume of cigarette smokers compared to WPS users.47,35,52 WP users demonstrated PFTs comparable (no significant difference between groups) to individuals who smoked cigarettes and deeply inhaled. 33 Of those individuals who smoked cigarettes, normal inhalation was associated with better PFT scores than deep inhalation. 33 Evidence also supports the possible serious health risks of passive smoking, as airway obstruction was significantly associated (P < 0.05) with WP and cigarette smoking. 43
Severity and prevalence of unspecified respiratory symptoms were reported to be significantly greater in WPS users than in nonsmoking individuals.32,33 Shortness of breath (P = 0.018), chronic cough (P = 0.007), and bronchitis (P = 0.026) were found to be significantly associated with WPS. 44 Chronic bronchitis and chronic obstructive pulmonary disease (COPD) were significantly associated (P < 0.05) with WPS.34,43,44,49 Passive WPS was significantly (P < 0.05) associated with COPD in one study 43 and was a significant (P < 0.05) risk for developing COPD in another. 49
There was a significant (P < 0.05) relationship between WPS and lung cancer in the two studies examining this relationship. In addition, a third study demonstrated that WPS users were six times more likely (P < 0.0001) to develop lung cancer than nonsmokers. 36
Oxidative Stress, Immunity, and Cell Cycle Interference Outcomes
Overview
Evidence of oxidative stress and immune factors such as white blood cell count and markers of inflammation is demonstrated in Table 3. The four studies were diverse in their focus and included cellular disruption,7,57–59 inflammation, and impairment of cellular oxygen delivery by measuring carboxyhemoglobin (COHb) and carbon monoxide levels. Studies from the cardiovascular and respiratory categories also examined COHb and carbon monoxide levels.46,50,51,56,60,61
WPS, oxidative stress, and inflammation in the lung and heart.
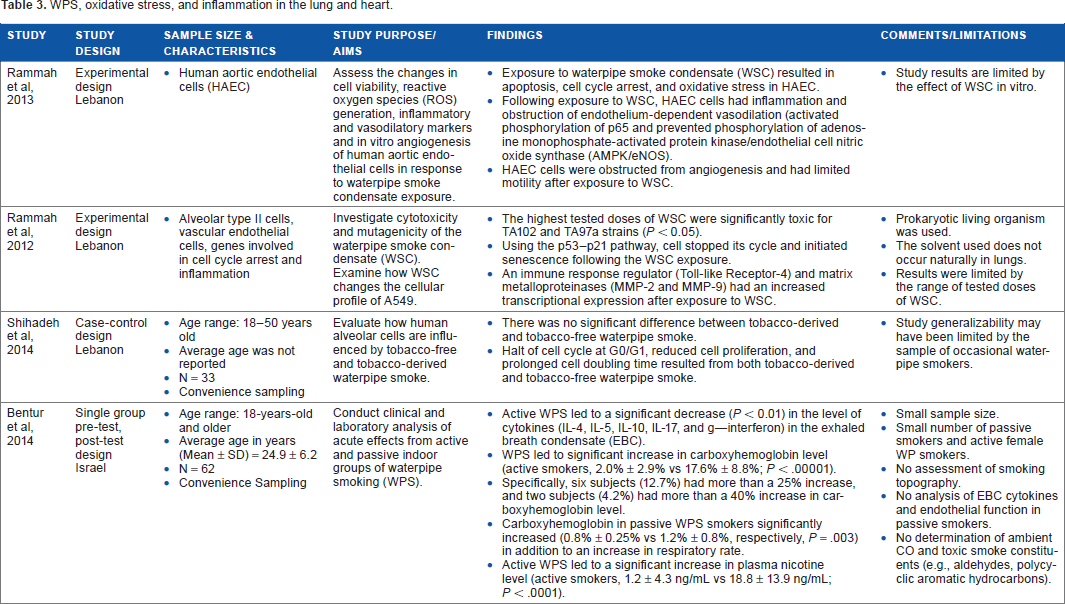
Synthesis of Results
Two in vitro studies examined cellular changes in aortic cells58,59 and alveolar cells. 58 Cellular damage was noted via apoptosis 10 and cell cycle arrest.7,58,59 One study explored the levels of inflammatory markers (cytokines) in the exhaled breath condensate of active WPS. 57 Anti-inflammatory cytokines (interleukin-4, 10, and 17) significantly (P < 0.01) decreased after WPS exposure. 57 COHb levels were significantly higher in both the active (P < 0.00001) and passive (P = 0.003) WPS groups after exposure to WPS. 57 Compared to cigarette use, the COHb level increased threefold after WPS (P = 0.0002).50,61
Other Outcomes
Overview
There were several other chemical toxicants associated with WPS that were included as outcome variables and that were included in this review, including elements such as arsenic, cadmium, chromium, nickel, and nicotine.28,29,51 Associated health conditions also included cancers such as bladder, esophageal, and nasopharyngeal cancers.25,37
Synthesis of Results
There were significant differences noted in the lung tissue of the WP smokers. The literature suggests that WPS increases certain levels of substances that may also have long-term negative health effects associated with nicotine. Nicotine levels were measured in four studies.51,60,61,63 One study found nicotine levels to only be significantly elevated in the cigarette use group; 60 one study found nicotine levels significantly increased after WPS use (P < 0.05); 51 and in contrast, one study found similar nicotine levels between cigarette use and WPS use. 61 One study found there to be a significant (P = 0.01) interaction between nicotine and increased heart rate as well as nicotine and smoking duration (P = 0.004). 63 Arsenic was significantly lower in nonsmokers than smokers (P < 0.05). 28 Nickel and cadmium levels were noted to be more significantly (P < 0.05) elevated in smokers (WP and cigarette users) than in nonconsumers of tobacco. 29 Nasal polyposis (soft, painless, noncancerous growths on the lining of nasal passages or sinuses) was significantly associated with WPS.28,29 This condition was also related to higher concentrations of blood metal (arsenic and chromium) levels.
Discussion
This systematic review has shown that WPS is associated with several health indicators such as increased vascular resistance, increased heart rate, increased blood pressure, lower PFT scores, shortness of breath, chronic cough, and health conditions such as bronchitis and chronic bronchitis, COPD, lung cancer, nasal polyposis, cellular damage, low immunity, and low birth weight. These results are in agreement with Akl et al 25 and El-Zaatari et al, 26 which reinforce the message that WPS is associated with poor health outcomes. This review supports the growing evidence that WP users had more coronary artery and cardiovascular diseases than nonsmokers. Passive WPS was also significantly associated with COPD in two studies. However, this review did not find that WPS was significantly associated with oral dysplasia, esophageal cancer, nasopharyngeal cancer, or bladder cancer.
This review demonstrates that the poor health outcomes associated with WPS are similar to those well-established for cigarette smoking. As most of the studies meeting the inclusion criteria for this systematic review were conducted outside of the US (33/40; 82.5%), it confirms the need for additional study among US populations, particularly with the recognized growing increase in WPS among youth and college-age young adults.2,66 More study is also needed of secondhand exposure. As noted in the “Results” section and Table 1, the evidence supporting the negative health effects of WPS on particularly the cardiovascular and respiratory systems (two of the identified four health outcome categories for this review) is wide and varied. Although research findings on the general health effects of WPS within the US should result in similar findings, this type of information is needed given the rapidly growing exposure, experimentation, and use of WPs in the US, which may be expanding beyond youth and college-age groups as the number of hookah cafés continues to grow and WP tobacco and its products are purchased via the Internet. As a result, WPS and its related secondhand smoke exposure risks ultimately threaten all the public health gains made in reducing cigarette use over the past decade. 67 It is therefore imperative that research studies be conducted in the US in order to provide the necessary empirical evidence to the FDA and US regulatory bodies for use in developing and implementing a WPS policy and regulation to affect the manufacture, distribution, and marketing of WPs to protect public health and prevent the well-known morbidity and mortality associated with tobacco consumption.
Furthermore, although evidence confirming the harmful health effects of WPS across these studies is provided, additional research among US populations is needed in order to assess potential differences among behaviors and patterns of use. Differences may include specific popular products, including the tobacco itself, the coal used, or the different types of WPs and hoses; length of time of the WPS session; how often the product is used; and if multiple tobacco products are used. This type of information is needed given the remarkable increase in uptake and regular use of WPs in the US in order to add further clarity regarding the association between WPS and reported health outcomes, which can be used to assess risks and educate the public.
This systematic review also signifies the need for longitudinal studies in order to assess the health effects over time for users and compare WPS-only users with multiple tobacco product users and nonsmokers. This comparison is necessary given that a significant proportion of WP smokers are also cigarette smokers. Short-term effects on the respiratory system and transmission of diseases as well as long-term health effects including cancer and cardiovascular disease should be assessed. Differences in products potentially popular between different cultures should be reported and studied for any different associations with different health outcomes.
Several limitations should be noted from this review. The research compiled for this review did not include WPS-only users in their studies. As such, there is difficulty in assessing the true harm specific to WPS since many studies included WP smokers who also reported smoking cigarettes. Although the harmful effects of WPS are likely to remain the same, the research on frequency and strength of exposure for WPS-only users and WPS users in the US might reveal different findings or degrees of harm from studies conducted in countries where WPS has a long history of use. Having information for WPS-only users would assist in providing some of the needed evidence to inform consumers, health-care professionals, the Food and Drug Administration, and US tobacco regulatory bodies for use in developing and implementing WPS policy and regulations similar to those for cigarettes. The desired outcome of these controls is the decrease in overall tobacco use and prevention of its associated well-established health-related morbidity and mortality.
Conclusion
Evidence clearly exists that establishes a connection between WPS use and the related harmful health effects. This review illustrates the consistency in the reported literature that WPS may be as harmful as cigarette smoking in terms of multiple health physiologic indicators and tobacco-related condition outcomes. This systematic review shows that the negative health effects, categorized within cardiovascular, respiratory, oxidative stress, immunity, and cell cycle interference, are caused due to the effects of nicotine and chemical toxicant exposures. This review calls attention to the need for additional research as WPS grows in popularity and use in the US. Additional research is needed to examine both the short- and long-term health effects of WPS, which will be added to the body of evidence used to inform policy statements aimed at reducing harm among those smoking and/or exposed to the secondhand smoke of WP tobacco use.
Author Contributions
Conducted the literature search, reviewed the articles, and prepared the original draft of the main sections: LH. Participated in the interpretation and writing the result sections: DLK. Reviewed and edited draft manuscripts, the final manuscript, and contributed to manuscript improvement: LSW. Participated in the study design, as well as reviewed and edited all versions of manuscript: TEB. Validated the literature search and assisted in editing the manuscript: AVF. Reviewed and edited the final manuscript: RG. All the authors read and approved the final manuscript.
Footnotes
Acknowledgments
We would like to acknowledge our editor Debra McDonald from the University of Florida College of Nursing.