
Abstract
Research on the association between waterpipe smoking and depression is limited. This study aimed to explore the prevalence and adjusted associated correlates of depression among Iranian adult. We analyzed data from 974 participants of a population-based cross-sectional study enrolling 18-50-year-old residents of Tehran, Iran in 2015. Data on lifetime self-reported history of depression, smoking behaviors, socioeconomic status, self-rated health, physical activity, stressful life events as well as a number of relevant confounders was obtained. Logistic regression models were employed for estimating adjusted odds ratios (ORs) and their 95% confidence intervals (CI). The mean (SD) age of the study sample was 32.55 (8.58) years. Of 974 recruited adults, 52.36% were female. The lifetime prevalence of depression in the general population was 17.0%. In general, 21.77% and 24.79% of participant reported lifetime history of cigarette and waterpipe smoking, respectively. While only cigarette smoking (OR = 1.94, 95% CI: (1.04-3.61) and only waterpipe smoking (OR = 1.65, 95% CI: (.95-2.86) were significantly associated with depression, joint cigarette and waterpipe smoking (OR= 3.76, 95% CI: (1.99-6.08) was the strongest correlate of depression followed by female gender (OR = 3.28, 95% CI: (2.08-5.15) and poor self-rated health (OR = 2.47, 95% CI: (1.73-3.53). The prevalence of self-reported depression in general population of Tehran is considerably higher than its global mean. We reported joint cigarette and waterpipe smoking as a significant correlate with depression in the general population. Future health promotion interventions should highlight the disadvantages of joint cigarette and waterpipe smoking targeting adults and especially females.
Introduction
Depression as a longlasting or recurrent disorder has been characterized by World health organization (WHO) as “sadness, loss of interest or pleasure, feelings of guilt or low selfworth, disturbed sleep or appetite, feelings of tiredness, and poor concentration. 1 ” In 2015, depression was a major contributor of global disability and was responsible for 7.5% of all years lived with disability. 1 While the global burden of depression is increasing,the low- and middle-income countries are more suffered from depression compared to high-income countries.1,2 In a systematic review by Lim G. et al., that pooled the findings from 30 countries, the lifetime and one-year prevalence of depression between 1994-2014 were 10.8% and 7.2%, respectively. 3 In another systematic review and meta-analysis by Moreno-Agostino et al., an increasing trend in over time prevalence of depression has been reported. 4 A national mental health study among Iranian adults reported an increasing trend in the prevalence of psychiatric disorders from 21% in 1999 to 23.5% in 2015 5 . Similarly, the lifetime prevalence of depression in a recent study on of Iranian adults was 29% 6 .
A number of factors including job dissatisfaction, low income and unemployment,7,8 personality traits, 9 marital status, education status, 8 social contact, 10 ethnic factors 11 as well as dietary patterns 12 have been reported to be associated with depression. Female sex as well as a number of socioeconomic status indicators including poor parental education, low academic performance along with poor within-family relationship have been reported as the most important predictors of depression among Iranian adults in a meta-analysis reported in 2013. 13
While evidence from prospective studies, as the most powerful observational studies, declares a mutual relationship between depression and smoking, 14 there are still inconsistent reports underlying the role and strength of the association between smoking behaviors and depression. 15 Waterpipe is increasingly smoked especially among the young in all WHO regions 16 and considered as a common smoking behavior in the Middle-East 17 with a wide range reported prevalence between 4%-15%. 18 A similar pattern has also been reported in Iran, particularly amongst females. 19 The prevalence of waterpipe smoking in Tehran has been reported as 17.6% in 2017. 19
Based on four proposed major aims of WHO’s Mental Health initiative, timely research on depression and identifying its determinants is critically important for decreasing its global and local burden. 20 Considering the simultaneous observed increasing trend in the prevalence of waterpipe smoking and depression in Iranian adults, we hypothesized that joint cigarette or waterpipe smoking, would be also associated with lifetime history of depression. This study aimed to explore the prevalence and to indentify the adjusted associated factors of depression amongst an Iranian adult population using data from a population-based study in Tehran, Iran.
Methods
This was a secondary analysis of the recent population-based case-control study that was conducted in Tehran, Iran in 2015 and we utilized data of the study general population sample. Details of recruitment, study protocol, measurement tools as well as the study response rate has been reported elsewhere.21,22 In sum, we randomly selected 1057 participants from 15-50 years old residents of 22 municipality areas of Tehran. We employed standard method of random digit dialing (RDD) protocol. 23 The Kish method was used to select one eligible individual from each selected household. 24 Phone interviews were conducted by 10 trained interviewers which were selected for their communication skills. By randomly recording interviews, the data collection process was monitored for any interviewer-related bias. 22 Oral informed consent was obtained from all participants before the interview. A total of 947 participants completed the study questionnaires.
Measurement
History of depression: We obtained information on the lifetime history of depression asking the following question: “Have you ever received a diagnosis of depression from a mental health professional?”
Smoking behaviors: We obtained information on lifetime cigarette smoking (never, current, past). Information on lifetime history of cigarette smoking was obtained asking the following questions; “Have you smoked 100 or more cigarettes during your entire life?” Moreover, data on participants’ current smoking status was also collected asking “Do you now smoke cigarettes every day, some days, or not at all?” Those who have smoked 100 cigarettes in their lifetime and who currently, “everyday” or “somedays”, smokes cigarettes were classified as current smoker. Past smokers were defined as those who have smoked at least 100 cigarettes in their lifetime but who had quit smoking at the time of interview. Finally, those who have never smoked, or who have totally smoked less than 100 cigarettes in their lifetime were categorized as never smokers. 25 Information on duration and average cigarette smoked per day was also collected and converted to pack-years. We classified participants who ever smoked waterpipe at least once a week for a minimum 6 months as those with positive history of waterpipe smoking. 22 Those who currently smoke waterpipe for at least one time per week during recent 6-month period were classified as current waterpipe smoker. We categorized the smoking behavior variable as those with only one active smoking behavior i.e. only waterpipe or only cigarette smokers and those with both smoking behaviors.
Stressful Life Events: We extracted data on the presence of stressful life events (SLE) asking for example; “did you experience death of one of your dear ones? 26 ” Data on the following SLE was obtained; marriage, death of spouse, death of a dear one including close relative (e.g. parent or sibling), divorce, jail term, retirement, severe illness of family members, family disruption (divorce of the parents), suicide, national exam for University entrance, dismissal from work, migration, homeless periods, and being in debt. 26 We calculated the total number of stressful life events summing all 15 life event categories as total stress number.
Physical activity: Physical activity during adolescence (frequency per week, intensity level (severe or light) and average duration (minutes)) was obtained from the study sample. 27 We converted the obtained information to the metabolic equivalent of task (MET). 28
Self-rated health: Data on self-rated health (SRH) was collected based on a single-item question with a 5-point numeric scale as suggested by WHO: “How would you rate your general health status? 29 ” We treated SRH as a continuous variable with the responses ranging from 5 to 1 (very satisfied, satisfied, neither satisfied nor unsatisfied, dissatisfied, and very dissatisfied) and dichotomized the variable as good (those with very satisfied and satisfied SRH) and poor. We employed this question as a proxy for the overall health of participants. The predictive validity as well as its reliability has been demonstrated.30,31
Subjective socioeconomic status (sSES): We asked the study participants to imagine a 10-stairs ladder with the subsequent frame: “Please imagine a 10-step ladder demonstrating where people stand in Tehran. Those people with the highest education, money and job situation are standing on the top rung. On the other hand, on the lowest rung, there are people with the poorest education, the least money, and the worst job situations. Then the higher up on the ladder, the better the social status and vice versa.” We requested the study participants to carefully select the rung that best reflects their socio-economic status in Tehran. We transformed the 10-item score of sSES into 5 categories for analysis. The reliability and validity of this scale has been published. 32
Lifetime alcohol use: The lifetime history of alcohol consumption was defined as intake of any type of alcohol for at least 6 times. We also obtained detailed information on drink duration (years), average number of drinks per month and average drink size of each drink (ml)). 33
Demographic characteristics: We also asked about demographic variables including age, sex, marital status (single or married), and educational level (illiterate or primary school, middle school, high school, associate's or bachelor’s degree, master's degree and higher).
Statistical analysis
Descriptive statistics was used to describe the characteristics of the study sample. The analysis was stratified by depression, in order to explore differences between the study groups. In bivariate analysis, independent t-test as well as chi square test were employed for continuous and categorical variables, respectively. We considered several relevant variables to detect their adjusted association with depression status including age, sex, stressful life event, history of smoking types (tobacco, waterpipe, and passive smoking), SES, marital status, educational level, lifetime alcohol intake, and physical activity. Multiple Logistic regression was used to estimate adjusted odds ratios (ORs) and their 95% confidence interval (95% CI). We also analyzed the smoking behaviors as those with active or those with only passive smoking history. Gender specific multiple logistic regression models with depression as outcome was also employed. We used Hosmer Lemeshow statistics for final model fitting. All statistical procedures were performed using Stata 12 (STATA Corp., Texas, USA) in 2018.
Results
Characteristics of the sample by depression status in the participants (N = 974), Tehran, Iran

MET: Metabolic Equivalent of Task; SRH: Self Rated Health sSES: subjective socio-economic status
aIndependent t-test for continuous and chi square test for categorical variables were employed.
bN (%), except where otherwise indicated. Depression data is missing in 4 participants.
Gender specific multiple logistic regression and unadjusted ORs of associated factors with depression in Iranian adults, 2015 (n=974)
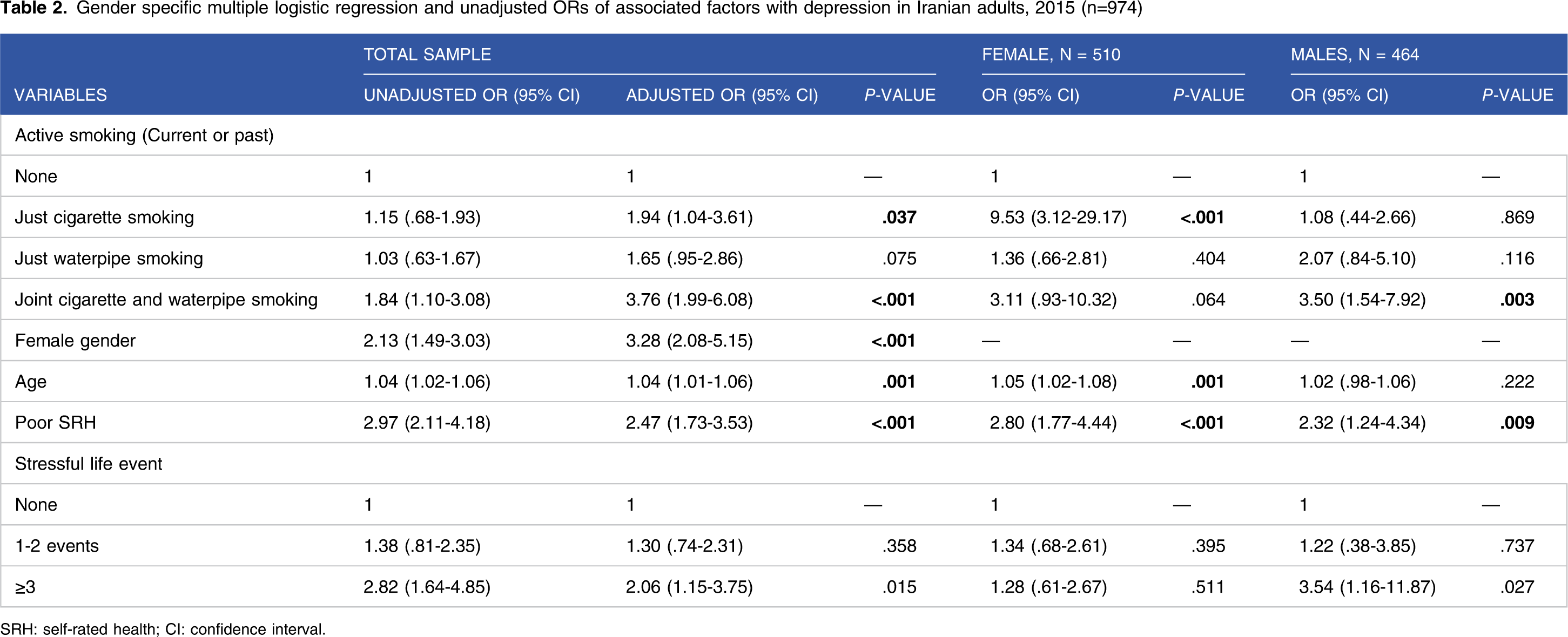
SRH: self-rated health; CI: confidence interval.
While sole cigarette smoking (OR = 9.53, 95% CI: (3.12-29.17) and poor SRH (OR = 2.80, 95% CI: (1.77-4.44)) were significantly associated with depression in females, joint cigarette and waterpipe smoking (OR = 3.50, 95% CI: (1.54-7.92)) as well as more than 2 SLEs (OR = 3.54, 95% CI: (1.16-11.87)) were the most important correlates of depression in males. As expected, those with poor SRH were consistently associated with the lifetime occurrence of depression in the total sample as well as in the gender specific subsamples.
Discussion
In 2015, in this population-based cross-sectional study on adults in Tehran, 17% of participants reported a lifetime history of depression diagnosed by a mental health professional. Joint consumption of waterpipe and cigarette smoking was the most important correlates of depression, followed by female gender and poor self-rated-health.
A number of studies reported the prevalence of depression in variety of Iranian sub-population.34,35 Based on 2015 global health estimates, 300 million people (4.4% of world’s population) aged≥ 15 years suffered from depression 1 which is considerably lower than the estimated prevalence in this study. However, considering the time of date collection in current study, the reported prevalence of depression should be interpreted with caution.Generally, a consistent link between active tobacco and passive smoking with depression is expected.15,36,37 For example, a meta analysis of cohort studies demonstrated a significant association between depression and smoking. 14 However, there are still incompatible findings on the direction and magnitude of the underlying association between smoking and depression. 15 Moreover, some studies showed an inverse association between heavy smoking and depression as a paradoxical finding. 38 In line with the results of Chaiton et al., meta analysis 14 as well as a community-based study that employed a similar methodology with current study and was conducted in low-and middle-income countries (LMICs), 39 our study confirmed the underlying association between smoking and depression.14,15,37
To our best knowledge, we are the first to examine the association between joint consumption of waterpipe and cigarette smoking and depression in the general population level. Our analyses found that sole cigarette or waterpipe smoking is associated with lifetime self-reported depression. Importantly, we demonstrated that those reporting both cigarette and waterpipe smoking were more strongly linked with lifetime history of depression compared with those with history of either cigarette or waterpipes smoking. Since nicotine can damage specific brain pathways that is responsible for regulating mood, it might be associated with mood swings. However, in the majority of people, smoking behavior usually starts before diagnosis of depression. Nevertheless, in our survey the underlying temporal relationship between smoking and depression is unclear. 15
Despite a general public perception of waterpipe smoking being less harmful,40,41 evidence doesn’t support its use as a safe alternative for tobacco smoking. A 10-times higher number of puffs and smoke volume inhaled per smoking sessions42,43 can result in a significant higher exposure to toxic chemicals by waterpipe smoking. Moreover, much higher concentration of heavy metals,42,44 a 36-times larger amount of nicotine, a-two times higher burning temperature of tobacco for waterpipe smoking (900°vs. 450°) 45 and a twice exhaled level of CO compared to cigarettes 46 are other harmful features of waterpipe smoking which impose serious negative health effect on its users. Waterpipe smoking is not considered as a social stigma in Tehran leading a dramatically sharp increase in its use regardless of gender, ethnicity or education level.
In line with the results of a 2‐year prospective cohort study on 6740 community‐dwelling older participants, 47 SRH was significantly linked with depression. In a cross‐sectional study on a random sample of 880 elderly participants by Benoit H Mulsant et al., depression played a role in consequent changes in self‐rated health. 48 SRH was not only reported as a predictor for depression in healthy people, but also, it has been suggested as an independent predictor for future major depressive syndrome in adult patients in a prospective 10-years follow up study. 49 We also found that those with more than two SLEs were more likely to report lifetime diagnoses of depression. This is reinforcing the results of previously conducted studies on different study populations.50,51
Amongst the strengths of our study the recruiting of a random sample of the general population can be highlighted. The response rate was acceptable, decreasing the likelihood of major non-response bias. However, some degree of selection bias might still have happened. If the prevalence of depression or smoking behaviors of non-responders were different to the participants, we could have over-estimated or under-estimated the magnitude of associations. However, in a cross-sectional study on 1200 residents of province of Tehran aged 15 or over, the prevalence of depression was reported 10.2% which is lower than our estimates. 52 The lack of temporality is an inherent limitation of cross-sectional studies and needs to be considered when interpreting our findings. We can demonstrate only associations, and not causal relationships. The current study only investigated the underlying association between the smoking use status with history of depression, not smoking level and intensity of depression. Moreover, the possibility of recall bias might distort the study estimates. The possibility of under-reporting of cigarette smoking is also important. However, currently, waterpipe smoking is not a social stigma in Iran society, decreasing the possibility of underreporting bias for this behavior. As we limited cases of depression to those who stated having received a diagnosis for it, the true population prevalence in Tehran might be higher. Finally, the relatively large estimated OR underlying the association between cigarette smoking and depression in females might be due to sparse data issue. In conclusion, the estimated prevalence of depression in this study is considerably higher than global health estimates reinforcing a need for public health activities aiming at improving the general populations’ mental health status. Even when controlling for age, sex and the number of stress-full life events, we identified joint consumption of waterpipe and cigarette smoking as the most important-previously unreported, correlate of depression. Future smoking cessation interventions are suggested to include targeting the behavior of smoking both cigaretteand waterpipes smoking as a serious neglected health issue in the adult population.
Footnotes
Acknowledgments
The authors would like to thank people who participated in this study.
Author Contributions
IA, SN, YS, MAM and ZG design and conducted the search. IA, IA-P, YS, and MC contributed to the data analysis and drafting the manuscript, and SN, MAM, and ZG revised the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by Tehran University of medical science
Ethical approval
The study was approved by the ethics committee of Tehran University of Medical Sciences (approval number: 127334-26145-188-02-93).