
Abstract
Background
Waterpipe tobacco smoking prevalence, practice, and the associated health perceptions among dental practitioners have not been previously reported. This study aims to determine the prevalence of waterpipe smoking among dental practitioners and to evaluate their awareness of health hazards of waterpipe smoking, particularly the adverse effects on oral health.
Methods
This was a cross-sectional questionnaire-based survey among dental practitioners. Surveyed dental practitioners practiced dentistry in the holy city of Al-Madinah Al-Munawarah, a city in the Central-Western Region of Saudi Arabia, and the study was conducted during March 2015. The questionnaire consisted of questions on demographic data, history and practices of tobacco use, and perceptions toward the health hazards of smoking. Dentists were approached at their work places and invited to participate. Descriptive statistics were used to describe the sample's demographic and smoking characteristics, while cross-tabulation and chi-square test were used to determine the statistical significance of association between the groups (P ≤ 0.05).
Results
One hundred dental practitioners participated in the survey, with 55 males and 45 females. Twenty-six percent indicated that they were water-pipe smokers. Male gender and cigarette smoking were the only factors to be significantly associated with waterpipe smoking (P = 0.008 and P = 0.000, respectively). Most participants stated that waterpipe smoking is harmful to health, and the most commonly reported health hazard was respiratory disease, which was reported by 81% of participants.
Conclusions
Prevalence of waterpipe smoking among dental practitioners is comparable to adult populations but lower than younger populations of university students. Health awareness of dental practitioners regarding waterpipe smoking was judged to be insufficient.
Background
The recent pandemic of waterpipe tobacco smoking does not appear to differentiate between age groups or genders, crossing geographic borders and bypassing cultural differences. 1 The increasing popularity of waterpipe smoking globally is evident in spite of mounting evidence that shows its associated health risks. 2 This pandemic has affected many countries in almost all continents, especially young age groups,3,4 with rates approaching 30%. 5 Interestingly, this type of smoking is gaining popularity among populations that are expected to resist health-risk behaviors, particularly those related to tobacco use. Professionals such as academicians, 6 physicians, 7 and medical university students 8 as well as females in conservative or religious communities 9 are taking on waterpipe smoking assuming that it is a “safer” and “healthier” option than the so far more popular cigarette smoking. In Bahrain for instance, waterpipe smoking was found to be the most common method of tobacco use among a sample of physicians. 7 Furthermore, surveys that were conducted in a Jordanian university found that 20% of a sample of its female employees 10 and 13.5% of a sample of faculty staff smoke waterpipe. 11
Among healthcare professionals, dental practitioners have a unique role in preventing and combating the adverse effects of tobacco smoking, since dental treatment is often based on frequent visits, providing the opportunity to contact the patient for a longer time and subsequently initiating and reinforcing tobacco cessation practices. 12 It is also estimated that more than 50% of smokers make an annual visit to the dentists. 13 Owing to dental practitioners’ experience and knowledge, they are capable of identifying adverse oral health effects of tobacco smoking, 14 particularly potentially malignant lesions. 15 Furthermore, they can adopt an approach to help their smoker patients to quit and maintain tobacco cessation efforts. This professional role may be jeopardized when dental practitioners actually engage in health-risk behaviors such as tobacco use. It was reported that currently smoking dentists showed a less positive attitude toward anti-smoking campaigns compared to ex-smokers. 16 Indeed, there is an evidence to link a dentist's own smoking habits and their desire to help patients quit smoking. 15 Hence, it is important to investigate tobacco use among dental practitioners as this habit may act as a barrier to the strategic role that they can play in providing tobacco prevention and cessation services to their patients. Up to our best knowledge, there is no published research that investigated the prevalence, attitude, and perceptions of dental practitioners to waterpipe tobacco smoking and its associated health risks. Therefore, the main aim of this study was to estimate the prevalence of waterpipe tobacco smoking among dental practitioners in Al-Madinah Al-Monawarah, Saudi Arabia, and to investigate their attitude and perceptions with reference to the potential health hazards of this type of smoking.
Participants and Methods
Ethical approval was obtained from the research ethics committee of Taibah University, College of Dentistry, on February 21, 2015. The research was conducted in complete accordance with the principles of the World Medical Association Declaration of Helsinki. All participants gave their written consent prior to participating in the study.
This study was conducted during March 2015 among dental practitioners working in the public and private sectors in Al-Madinah Al-Munawarah, which is located in the Central-Western Region of Saudi Arabia. Dental practitioners from university hospitals, primary healthcare centers, and private practices were invited to participate during working hours. At the time of the study, there were 370 dentists working in the area of Al-Madinah Al-Munawarah. A sample size of 100 participants was determined to provide between 80% and 90% power of study using an expected frequency of 20% water-pipe smoking, a confidence limit of 5%, and power of study between 80% and 90% (Epi Info software, Center for Disease Control). A convenience sample was formed as the co-author (NS) distributed a hard copy of the questionnaire by visiting the dentists in their practices. First, those dentists located near Taibah University Dental School and Hospital (Central Region of the city) were visited and invited to participate, followed by those situated farther away. This cross-sectional study was based on a modified self-administered questionnaire that was used in other previous studies on comparable samples. 6 This questionnaire was modified to include questions pertaining to sociodemographic and professional profiles of the participating dentists (the previous questionnaire was directed to university staff).
The questionnaire consisted of questions on gender, age, specialty, marital status, year and country of graduation, smoking habits (waterpipe and cigarette), and awareness about the health hazards of waterpipe smoking. Questions on smoking habits explored the method of tobacco use, age of onset of smoking, frequency, quantity, use of hygienic method of waterpipe smoking and disposables, and knowledge on harmful effects of waterpipe smoking. Responses were entered into and analyzed using the IBM SPSS software version 21.0. Descriptives and frequencies were obtained, and data were cross-tabulated to determine the significance of association between the groups. Chi-square test was used, and significance was set at P ≤ 0.05.
Results
A total number of 107 dentists were conveniently selected and invited to participate. Seven dentists opted not to participate, giving a response rate of 93.5%. Table 1 lists the sociodemographic and professional characteristics of the study sample along with the significance of association with cigarette and waterpipe smoking.
Sociodemographic and professional characteristics of participants and significance of association with cigarette and waterpipe smoking.
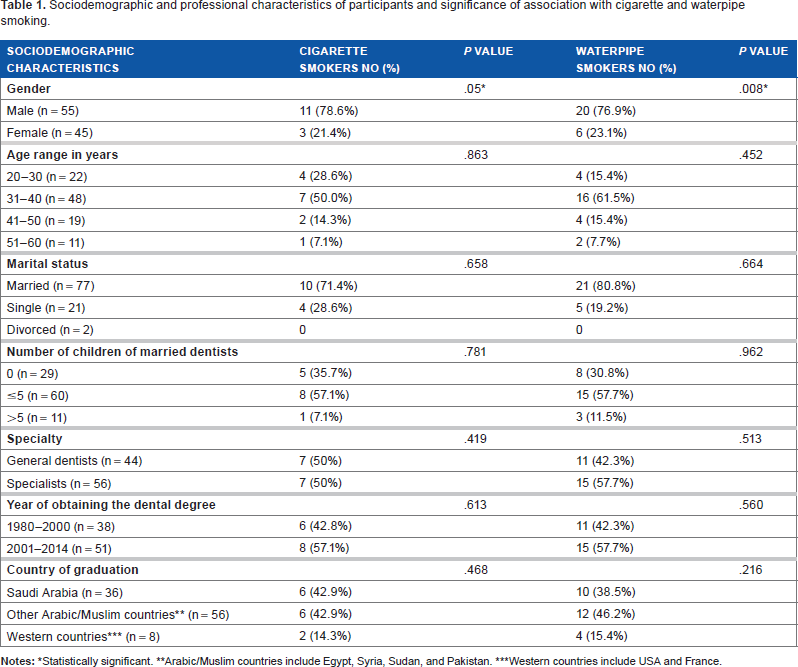
Statistically significant.
Arabic/Muslim countries include Egypt, Syria, Sudan, and Pakistan.
Western countries include USA and France.
Twenty-six dentists stated that they were waterpipe smokers with 20 males and 6 females. Twenty of them indicated they smoked waterpipe on a monthly basis, while five smoked on a weekly basis and only one participant smoked on a daily basis. Fourteen of them were dual waterpipe and cigarette smokers. The age of onset of smoking ranged from 11 to 30 years.
Cross-tabulation revealed a significant association between waterpipe smoking and cigarette smoking (P = 0.000) and between waterpipe smoking and gender (P = 0.008).
There was no significant association between waterpipe tobacco smoking on one hand and the other demographic data on the other hand.
As for the health perceptions of the study sample, the regular use of a disposable mouthpiece was reported by only 14 (53.8%) of waterpipe smokers. Only 16 of waterpipe smokers stated two reasons for practicing this habit, fun and relaxation after work (38.5%) and addiction to nicotine (23.0%). On the other hand, only 11 (42.3%) stated that they would like to quit waterpipe smoking.
Almost 94% of the participants perceived waterpipe smoking as harmful to health. Also, 50% of the sample believed that waterpipe smoking is more harmful than cigarettes, 39% believed that cigarettes are more harmful than waterpipe smoking, and the remaining 11% could not determine which is more harmful.
Figure 1 shows the health hazards of waterpipe smoking as perceived by the study sample.
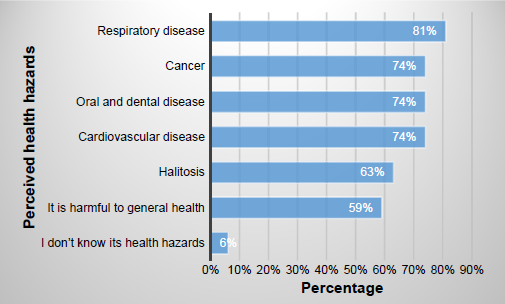
health hazards of waterpipe smoking as perceived by participants.
Discussion
This study provides the first insight into the practice and health awareness of dental practitioners toward waterpipe smoking. Previous studies in this region of the world have shown a lower prevalence of waterpipe tobacco smoking among a sample of highly educated people 6 and healthcare professionals. 7 The prevalence reported in this study is similar to that reported in general adult populations in Arabic countries; 17 however, it is lower than that reported among younger populations of adolescents and university students who may have a prevalence of 30%. 18 This can be explained based on the behavioral attitudes of younger people, while older people might have less interest in waterpipe as they are engaged in their careers and family lives.
Dental practitioners are supposed to have a sufficient medical knowledge on the adverse health effects of tobacco use, including the relatively recent resurrection of water-pipe tobacco use. Furthermore, smoking prevalence among dentists is reported to be the lowest among all health professionals.19,20 However, our sample of dentists show insufficient knowledge about the health hazards of waterpipe tobacco smoking and an unexpectedly high prevalence of waterpipe smoking. This prevalence could be attributed to the nature of the dental career. Dentistry is known to be a stressful career, 21 and dentists have been shown to resort to certain practices to deal with their stresses, such as drinking alcohol. 22 However, in Arabic countries where Islam is the religion of the majority of people, drinking alcohol is not acceptable on social and religious bases. Waterpipe smoking, on the other hand, is considered a popular habit that is widely available in the community and is equally socially acceptable. 9 A recent review done by Akl et al 23 on the motives for waterpipe use found that the main motives were socializing, relaxation, pleasure, and entertainment. A high prevalence of cigarette smoking was found among dentists of both genders in Brazil; this was explained by the high stress level posed by dentistry, 24 a stress that can unfortunately lead to suicide. 25 Indeed, a substantial proportion of waterpipe smokers (38.5%) in our study stated that they use waterpipe for fun and relaxation after work. The practice of waterpipe smoking by dentists as an alternative stress relief habit needs further investigation in future studies. Another possible explanation for this high prevalence is the geographic area itself, the Arabian Peninsula, which is known for popularity of waterpipe smoking. In Saudi Arabia, where this study was conducted, previous studies have shown a high prevalence of waterpipe smoking among Saudi adolescents 26 and university students. 27
None of the investigated demographic variables were significantly associated with waterpipe smoking except for gender, as waterpipe smoking was highly associated with males. However, studies have shown that waterpipe smoking is becoming the favorable type of smoking among females of different age groups and social backgrounds even in Arabic societies, which are otherwise known to be conservative and religious.9,28,29 The community of the holy city of Al-Madinah Al-Munawarah where this study was conducted does not encourage women to smoke waterpipe in public. Selling cigarettes and providing waterpipe services are prohibited within the boundaries of the old city. Even more, coffee shops outside the holy city (Haram) provide smoking services exclusively for men and not for women. This makes women who smoke waterpipe do that within the privacy of their homes or the private social outdoor gatherings of their family members and friends.
Another factor that was significantly associated with waterpipe smoking was cigarette smoking. This finding is expected since both waterpipe and cigarettes contain nicotine and can eventually lead to nicotine addiction 30 with one type of tobacco use leading to the other. After entering the body, nictotine binds to nicotinic acetylcholine receptors of the central nervous system, specifically those located in the brain, initiating drug addiction, and with the persistent interaction between nicotine and these receptors, a behavioral desire to continue the intake of nicotine results. 31 In fact, 23% of waterpipe smokers in this study stated that nicotine addiction is the reason behind waterpipe smoking. Perhaps, this is why as low as 42.3% of waterpipe smokers expressed their willingness to quit this habit.
Approximately half of the waterpipe smokers do not use disposable mouthpieces regularly, a finding that reflects health-risk behavior, particularly when considering the risks of waterpipe sharing. Infections such as cold, herpes labialis, and tuberculosis may all be transmitted orally. 32 Although disposable mouthpieces may be made of potentially unsafe materials such as plastic, their use could help lessen the likelihood of transmission of certain microorganisms present in the saliva of smokers.
Almost one in two in the sample believed that water-pipe tobacco smoking was less harmful to health than cigarette smoking or even could not determine which of them was more harmful than the other. A comparable percentage was reported among a sample of junior doctors working in the UK. 33 On contrary to the common belief that waterpipes are healthier than cigarettes, research has shown that due to the longer and more persistent duration of inhalation and exposure, a waterpipe smoker may inhale the equivalent of 100 or more cigarettes during a single session. 34
Several important health hazards are associated with waterpipe smoking, and these include cardiovascular effects such as increased heart rate and blood pressure, respiratory effects such as chronic obstructive pulmonary disease, cancer besides obstetric and perinatal complications, and osteoporosis. 35 Although the study sample reported correctly the possible health hazards of waterpipe smoking, their responses were in the form of general terms such as respiratory and cardiovascular effects and they did not explain accurately these health hazards. Further, they missed some important health hazards such as adverse pregnancy outcomes. Regarding oral health, which is the bread and butter of dental practitioners, none of the documented oral health hazards were mentioned by our participants. Waterpipe smoking was shown to be associated with certain oral health problems such as periodontal disease 36 and dry socket. 37 Its association with oral cancer also cannot be excluded. 2 While the study participants were not knowledgeable about the possible oral health hazards associated with waterpipe smoking, interestingly, they mentioned undocumented effects such as halitosis. Almost all our participants were considered as relatively recent graduates of dentistry, having graduated after the year 1980. Considering that waterpipe tobacco smoking epidemic is also known to have emerged during the 1990s, a sufficient background on this type of tobacco use should be available to all our participants, including the associated health risks.
Conclusions and Recommendations
Dental practitioners have a prevalence of waterpipe smoking that is comparable to adult populations of the Arab countries. Moreover, their knowledge of health hazards of waterpipe smoking is not sufficient.
The authors recommend integration of knowledge on health hazards of waterpipe smoking into continuing medical education for dentists and provide them with training on the methods of tobacco use cessation. Dental curricula for undergraduate students should be reformulated to include knowledge on waterpipe smoking-related diseases with a particular attention to oral health. Other aspects that may be addressed in the curricula are behavioral and social aspects of waterpipe smoking and the management of its dependence. Dental students can be motivated to play a proactive role in designing anti-waterpipe smoking campaigns considering the fact that most victims of this habit are adolescents and youth. More dental practitioners should be encouraged to enroll in smoking cessation programs to work hand in hand with other healthcare professionals in combating the emerging and popular trends in tobacco use.
Author Contributions
Questionnaire and study design, participant recruitment, and initial and final draft: ND-O. Questionnaire design, participant recruitment, and literature review: NS. Study design, participant recruitment, and initial draft: AA. Questionnaire and study design and statistical analysis: OA-H and MHA-S. All authors read and approved the final draft.